Successful Treatment of Neutropenia Associated With T‐Cell Large Granular Lymphocytic Leukemia Using Fludarabine
Yoshiki Uemura, Kazuto Togitani, Yoshitaka Kumon

TL;DR
An 81-year-old woman with T-cell large granular lymphocytic leukemia successfully treated with fludarabine after other therapies failed.
Contribution
This case is the first documented in Japan showing fludarabine's effectiveness in treating T-LGLL-related neutropenia.
Findings
Fludarabine increased neutrophil counts and reduced LGL levels in a patient with T-LGLL.
Common immunosuppressive therapies like methotrexate and tacrolimus failed to improve neutropenia.
The successful treatment suggests fludarabine could be a viable option for T-LGLL-related neutropenia.
Abstract
T‐cell large granular lymphocytic leukemia (T‐LGLL) is an uncommon lymphoproliferative disorder that typically follows a slow clinical course. Symptoms often remain subtle until cytopenia or infection develops. Severe infection secondary to neutropenia represents the major cause of mortality. We describe an uncommon case involving an 81‐year‐old woman diagnosed with T‐LGLL whose agranulocytosis was followed by recurrent infections. Immunosuppressive agents such as methotrexate, cyclophosphamide, and tacrolimus—commonly recommended by current guidelines—were administered but failed to improve neutropenia. Administration of fludarabine, a purine analog listed as a second‐line option in the NCCN guidelines, led to a prompt rise in neutrophil counts and a concomitant decline in LGL levels. To our knowledge, no prior Japanese report has documented successful use of fludarabine monotherapy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
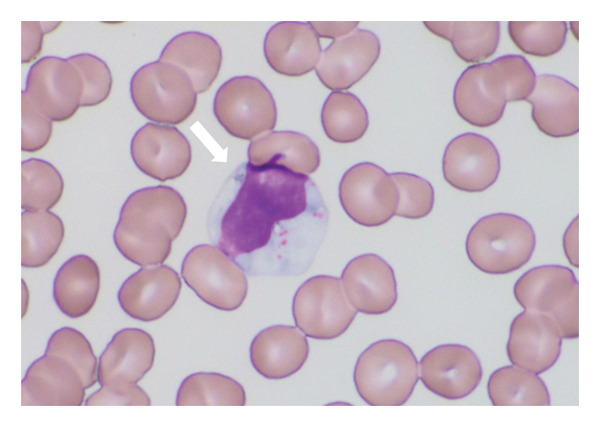 Figure 2
Figure 2| Category | Parameter | Value | Reference range |
|---|---|---|---|
| Complete blood count | WBC | 9600/μL | 3300–8600/μL |
| Seg | 87% | 45–60% | |
| Lymphocyte | 9% | 25–45% | |
| Mono | 4% | 4–7% | |
| RBC | 154 × 104/μL | 386–492 × 104/μL | |
| Hb | 6.8 g/dL | 11.6–14.8 g/dL | |
| Ht | 20.1% | 35.1–44.4% | |
| MCV | 132.2 fL | 83.6–98.2 fL | |
| PLT | 9.4 × 104/μL | 15.8–34.8 × 104/μL | |
| Urinalysis | Color | yellow | — |
| Protein | (+/−) | (−) | |
| Glucose | (−) | (−) | |
| Occult blood | (+) | (−) | |
| Urinary sediments | RBC | 1–4/H | — |
| WBC | 30–40/H | — | |
| Serological test | Haptoglobin | 87 mg/dL | — |
| Intrinsic factor Ab | (+) | (−) | |
| Genetic test | WT1 mRNA | 2.3 × 102 copy/μg RNA | < 50 copy/μg RNA |
| Category | Parameter | Value | Reference range |
|---|---|---|---|
| Biochemistry tests | TP | 5.6 g/dL | 6.6–8.1 g/dL |
| Alb | 3.5 g/dL | 4.1–5.1 g/dL | |
| AST | 22 U/L | 13–30 U/L | |
| ALT | 15 U/L | 7–23 U/L | |
| ALP | 386 U/L | 38–113 U/L | |
| γ‐GTP | 219 IU/L | 9–32 U/L | |
| CHE | 13 IU/L | 240–486 U/L | |
| LDH | 378 U/L | 124–222 U/L | |
| T‐bil | 1.0 mg/dL | 0.4–1.5 mg/dL | |
| BUN | 19.8 mg/dL | 8–20 mg/dL | |
| Cr | 0.42 mg/dL | 0.46–0.79 mg/dL | |
| UA | 3.4 mg/dL | 2.6–5.5 mg/dL | |
| T‐CHO | 137 mg/dL | 142–248 mg/dL | |
| TG | 86 mg/dL | 40–234 mg/dL | |
| Glu | 142 mg/dL | 73–109 mg/dL | |
| HbA1c | 4.80% | 4.3–5.8% | |
| Na | 137 mEq/L | 138–145 mEq/L | |
| K | 4.5 mEq/L | 3.6–4.8 mEq/L | |
| Cl | 103 mEq/L | 101–108 mEq/L | |
| CRP | 0.66 mg/dL | 0.00–0.14 mg/dL | |
| Fe | 44 μg/dL | 80–200 μg/dL | |
| UIBC | 126 μg/dL | 168–252 μg/dL | |
| Ferritin | 439.4 ng/mL | 39.4–340 ng/mL | |
| Vitamin B12 | 57 pg/mL | 180–914 pg/mL | |
| Folic acid | 2.1 ng/mL | 3–20 ng/mL | |
| Bone marrow findings | NCC | 34 × 104/μL | |
| Mgk | 345/μL | ||
| Pro‐E | 0.2% | ||
| Ba‐E | 4.4% | ||
| Poly‐E | 19.8% | ||
| Orth‐E | 1.0% | ||
| Myeloblast | 0.6% | ||
| Pro‐mye | 2.0% | ||
| Mye | 13.4% | ||
| Meta‐Myelo | 9.8% | ||
| Stab | 9.8% | ||
| Seg | 30.2% | ||
| Eosino | 1.0% | ||
| Baso | 0.2% | ||
| Lymphocyte | 0.4% | ||
| Mono | 0.4% | ||
| Plasma | 2.2% | ||
| MΦ | 0.6% | ||
| M/E | 2.7 | ||
| Chromosome | 46, XX | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Lymphocytic Leukemia Research · Immunodeficiency and Autoimmune Disorders · Blood disorders and treatments
1. Introduction
Felty syndrome (FS) is a rare complication of rheumatoid arthritis (RA), defined by the triad of splenomegaly, neutropenia, and joint destruction, occurring in fewer than 1% of RA patients [1]. Peripheral expansion of large granular lymphocytes (LGLs) occurs in roughly one‐third of FS cases [2]. Clonal proliferation of cytotoxic T‐cell–type LGLs defines T‐cell large granular lymphocytic leukemia (T‐LGLL) [3]. T‐LGLL frequently coexists with autoimmune disorders, including RA, FS, Coombs‐negative hemolytic anemia, immune thrombocytopenia, and pure red cell aplasia [4–6]. RA occurs in approximately 11%–36% of patients with LGLL [7]. Given their overlapping clinical and immunologic profiles, FS and T‐LGLL are considered possible phenotypic variants within the same pathogenic continuum [8].
Distinction between FS and T‐LGLL often relies on the presence of T‐cell receptor (TCR) gene rearrangements [9]. Our patient was diagnosed with T‐LGLL associated with RA based on confirmation of TCR gene rearrangement. Because T‐LGLL typically progresses slowly, observation without immediate treatment is reasonable in asymptomatic cases [10]. Treatment is indicated when cytopenias, infections, progressive splenomegaly, or systemic “B” symptoms develop [11].
Since leukemic LGLs function as persistently activated cytotoxic lymphocytes, immunosuppression remains the cornerstone of therapy [3, 12, 13]. First‐line options include methotrexate (MTX), cyclophosphamide (CPA), or cyclosporine (CyA), administered singly [14, 15]. MTX often benefits patients with neutropenia, whereas CPA is more effective for anemia, particularly pure red cell aplasia [16, 17]. A clinical response typically requires several months of continuous therapy [16]. Because prolonged immunosuppression can increase infection risk, therapies capable of rapidly restoring neutrophils are desirable.
2. Case Presentation
An 81‐year‐old woman had been diagnosed with RA in 2012 and was referred to our hospital in September 2020 for active arthritis and agranulocytosis. Because arthritis activity was high, so mizoribine, tacrolimus, and salazosulfapyridine were started (Figure 1(a)). Because of coexisting RA and neutropenia, FS was suspected, though splenomegaly was absent. As no infectious events were seen, she was observed without specific treatment for neutropenia.
Figure 1. Clinical parameters and treatments from December 2022 to September 2025. (a) Clinical course from the first visit to near‐zero neutrophil count (February 5, 2021–December 20, 2022). MZB, mizoribine; TAC, tacrolimus hydrate; SASP, salazosulfapyridine; WBC, white blood cell; Hb, hemoglobin; PLT, platelet; Neut, neutrophil. (b) After febrile neutropenia (FN) treatment, neutrophils temporarily increased but later declined, while WBC showed an upward trend (December 20, 2022–May 7, 2024). FN treatment was initiated with meropenem (MEPM) but fever persisted; therefore, ceftriaxone (CTRX) and vancomycin (VCM) were added. As these were ineffective, cefepime (CFPM) combined with lenograstim led to defervescence and an increase in neutrophil count. ABT, abatacept; LGL, large granular lymphocyte; PSL, prednisolone; CFPM, cefepime; MEPM, meropenem; CTRX, ceftriaxone; VCM, vancomycin; LENO, lenograstim. (c) Immunosuppressive therapy was ineffective for severe neutropenia and increased LGL count. Combination therapy with fludarabine and pegfilgrastim (May 21, 2024–September 25, 2025) improved both parameters. RIT, rituximab; MTX, methotrexate; CPA, cyclophosphamide; FIL, filgrastim; PEGFIL, pegfilgrastim; Flu, fludarabine; MCFG, micafungin.(a)(b)(c)
By November 2022, her neutrophil count had declined to < 100/μL. In February 2023, febrile neutropenia (FN) developed and was treated with antibiotics and filgrastim, resulting in transient recovery and fever resolution. To avoid recurrence, mizoribine and salazosulfapyridine were discontinued, and abatacept was introduced. Nevertheless, neutropenia worsened again in December 2023, while total WBC gradually increased (Figure 1(b)). By May 2024, WBCs were 11,200/μL, but neutrophils remained absent. Peripheral smear showed LGLs (34% of WBCs) (Figure 2). Flow cytometric analysis of peripheral lymphocytes revealed a CD2+CD3+CD5+CD7+CD8+CD57+ T‐cell population, consistent with cytotoxic T‐cell proliferation. TCR gene rearrangement analysis demonstrated clonality in both the TCR‐γ and TCR‐β chains, confirming the diagnosis of T‐LGLL. The laboratory findings at diagnosis are summarized in Tables 1 and 2)
May–Grünwald–Giemsa staining of peripheral blood (× 1000). A white arrow indicates a large granular lymphocyte.
A recurrent FN episode in July 2024 required broad‐spectrum antibiotics. Rituximab on July 11 plus filgrastim achieved minimal response [18]. MTX (5 mg/week) was started on July 19, 2024, with PSL 30 mg/day (tapered thereafter); due to persistent neutropenia, MTX was stopped on August 23 and CPA 50 mg/day was given from August 30 to September 19, 2024, with only incidental overlap from PSL tapering—not intentional combination therapy. Because alemtuzumab was unavailable in Japan, oral fludarabine was selected per NCCN guidance. Treatment began on October 11, 2024. The first course consisted of (40 mg/day x 5 days per month) was followed by filgrastim for 8 days. During the second and third courses (40 mg/day x 3 days, no G‐CSF), transient neutropenia and LGL resurgence occurred. From the fourth course onward, fludaraine (40 mg/day x 4 days) plus pegfilgrastim after each cycle lead to sustained neutrophil recovery and continuous LGLs decline. This response persisted throughout the observation period until September 25, 2025 (Figure 1(c)). Because of arthritis flare, salazosulfapyridine and tacrolimus were reintroduced. The overall course is summarized in Figure 1(c).
3. Discussion
FS is defined by the coexistence of RA, splenomegaly, and neutropenia [19]. It usually emerges > 10 years after RA onset [20]. In our patient, severe neutropenia appeared over 10 years after RA diagnosis but without splenomegaly, so FS was initially suspected. LGLL is not always indolent; rather, the disease frequently has an indolent course. Approximately 85% are T‐cell type [21].
RA is present in 11%–36% of T‐LGLL patients [7, 22], whereas clonal LGL expansion occurs in 5%–10% of RA patients, indicating a bidirectional association and shared pathogenesis [8, 23]. Our patient presented with RA and persistent agranulocytosis; TCR gene rearrangement confirmed T‐LGLL, demonstrating this overlap.
Given its indolent nature, T‐LGLL is often observed without therapy, but treatment is warranted for severe cytopenia or infection. Because RA, FS, and T‐LGLL are considered to lie on a pathogenic continuum, we initially attempted to suppress RA activity using rituximab, hoping this would attenuate LGL‐driven neutropenia. Although previous reports describe improvement of cytopenias in RA‐associated LGL disorders following rituximab therapy [18], our patient showed only minimal hematologic response. Therefore, we proceeded with conventional immunosuppressive agents. First‐line immunosuppressants (MTX, CPA, and CyA) remain standard [7, 12–15]. In this case, MTX plus prednisolone followed by CPA were ineffective, underscoring the limitation of conventional therapy.
Although methotrexate and cyclophosphamide usually require several weeks to months for an adequate assessment of efficacy in T‐LGLL, our patient had profound agranulocytosis and recurrent infections, making prolonged treatment under severe neutropenia clinically unsafe. Neither MTX nor CPA produced any early indication of hematologic improvement, which justified the decision to discontinue these agents earlier than the conventional treatment duration.
Fludarabine, cladribine, and pentostatin are NCCN category 2A options for refractory T‐LGLL [7]. Fludarabine inhibits DNA synthesis in proliferating lymphocytes and may explain the rapid neutrophil recovery observed here. Although previous reports showed variable responses [24–26], our case suggests that combining fludarabine with pegfilgrastim may accelerate hematologic recovery without LGL re‐expansion.
While a durable response was achieved, long‐term safety in elderly patients with autoimmune backgrounds remains uncertain. Because the observation period in this case remains relatively short, longer follow‐up is required to determine whether hematologic remission and clinical stability can be maintained over the long term.
In summary, this case highlights that oral fludarabine combined with pegfilgrastim can induce rapid and sustained neutrophil recovery in T‐LGLL refractory to standard immunosuppressive therapy, providing a feasible outpatient option for elderly patients with RA‐associated disease.
Ethics Statement
Ethical approval was waived by the institutional review board of Chikamori Hospital because this is a single‐patient case report that does not contain identifiable patient information.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Disclosure
All authors have read and approved the final version of the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Author Contributions
Yoshiki Uemura contributed to the conception, design, and drafting of the manuscript. Kazuto Togitani supervised the clinical management and critically reviewed the manuscript. Yoshitaka Kumon contributed to the diagnosis and management of rheumatoid arthritis and provided rheumatologic expertise. Yoshiki Uemura had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
No specific grant or funding was received from any public, commercial, or not‐for‐profit sector for this study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rosenstein E. D. and Kramer N. , Felty’s and Pseudo-felty′s Syndromes, Seminars in Arthritis and Rheumatism. (1991) 21, no. 3, 129–142, 10.1016/0049-0172(91)90002-H, 2-s 2.0-0026317245.1788550 · doi ↗ · pubmed ↗
- 2Bowman S. J. , Bhavnani M. , Geddes G. C. et al., Large Granular Lymphocyte Expansions in Patients with Felty’s syndrome: Analysis Using Anti-t Cell Receptor V Beta-specific Monoclonal Antibodies, Clinical and Experimental Immunology. (1995) 101, no. 1, 18–24, 10.1111/j.1365-2249.1995.tb 02271.x.PMC 15533097621587 · doi ↗ · pubmed ↗
- 3Loughran T. P.Jr., Kadin M. E. , Starkebaum G. et al., Leukemia of Large Granularlymphocytes: Association with Clonal Chromosomal Abnormalities and Autoimmune Neutropenia, Thrombocytopenia, and Hemolytic Anemia, Annals of Internal Medicine. (1985) 102, no. 2, 169–175, 10.7326/0003-4819-102-2-169, 2-s 2.0-0021909118.3966754 · doi ↗ · pubmed ↗
- 4Savola P. , Bhattacharya D. , and Huuhtanen J. , The Spectrum of Somatic Mutations in Large Granular Lymphocyte Leukemia, Rheumatoid Arthritis, and Felty’s syndrome, Seminars in Hematology. (2022) 59, no. 3, 123–130, 10.1053/j.seminhematol.2022.07.004.36115688 · doi ↗ · pubmed ↗
- 5Shvidel L. , Duksin C. , Tzimanis A. et al., Cytokine Release by Activated T-cells in Large Granular Lymphocytic Leukemia Associated with Autoimmune Disorders, The Hematology Journal. (2002) 3, no. 1, 32–37, 10.1038/sj.thj.6200149, 2-s 2.0-85047683364.11960393 · doi ↗ · pubmed ↗
- 6Wang S. Y. and Li Y. , A Case of T-cell Large Granular Lymphocytic Leukemia with Autoimmune Hemolytic Anemia and Literature Review, Am J Transl Res. (2024) 16, no. 10, 5735–5742, 10.62347/URFI 7647.39544786 PMC 11558414 · doi ↗ · pubmed ↗
- 7Lamy T. and Loughran T. P.Jr., How I Treat LGL Leukemia, Blood. (2011) 117, no. 10, 2764–2774, 10.1182/blood-2010-07-296962, 2-s 2.0-79953074500.21190991 PMC 3062292 · doi ↗ · pubmed ↗
- 8Naji R. S. , Rafiee B. , Raju G. , Solhjoo M. , and Anand P. , T-cell Large Granular Lymphocyte Leukemia in a Patient with Rheumatoid Arthritis, J Investig Med High Impact Case Rep. (2020) 8, 1–4, 10.1177/2324709620941303.PMC 735701832646239 · doi ↗ · pubmed ↗