Prevalence of Low Back Pain in Nonworking Women in Eastern Saudi Arabia: A Cross-sectional Survey
Zahra Alhasan, Ali M Al Mousa, Hassan M Alturaiki, Othman Altaissan, Abdullah H Alramadan

TL;DR
This study found that 92% of nonworking women in Eastern Saudi Arabia experience low back pain, with age being the only significant factor.
Contribution
The study provides new prevalence data on low back pain specifically among nonworking women in Saudi Arabia.
Findings
92.1% of nonworking women in the study reported low back pain.
Age was the only factor significantly associated with low back pain (p = 0.034).
Most participants (76%) reported that low back pain did not prevent them from performing daily activities.
Abstract
Background Low back pain (LBP) is one of the most common public health, economic, and social problems worldwide. LBP has been reported to be more prevalent in nonworking populations than in working populations among both men and women. Therefore, this study aimed to evaluate the prevalence of LBP among nonworking women in the Eastern region of Saudi Arabia. Methods A cross-sectional study was conducted in the Eastern region of Saudi Arabia from October to November 2023 using an online questionnaire. Results A total of 390 eligible participants were included. The prevalence of LBP among nonworking women was 92.1%. Age was the only factor significantly associated with LBP (p = 0.034). Other factors showed no significant association, including education level (p = 0.954), marital status (p = 0.061), socioeconomic status (p = 0.305), number of children (p = 1.000), pregnancy status (p…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
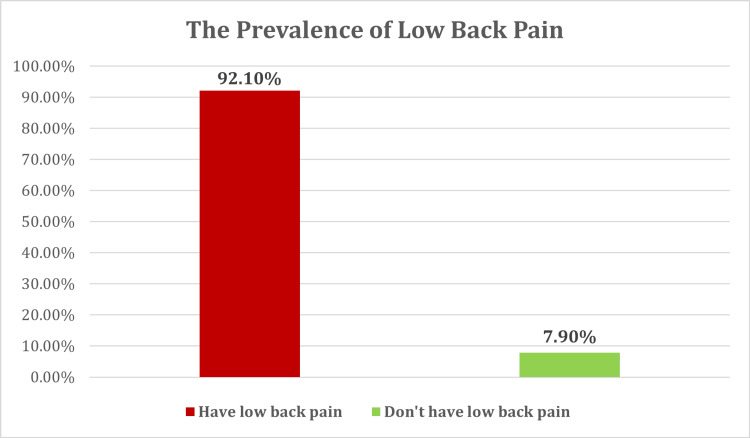 Figure 1
Figure 1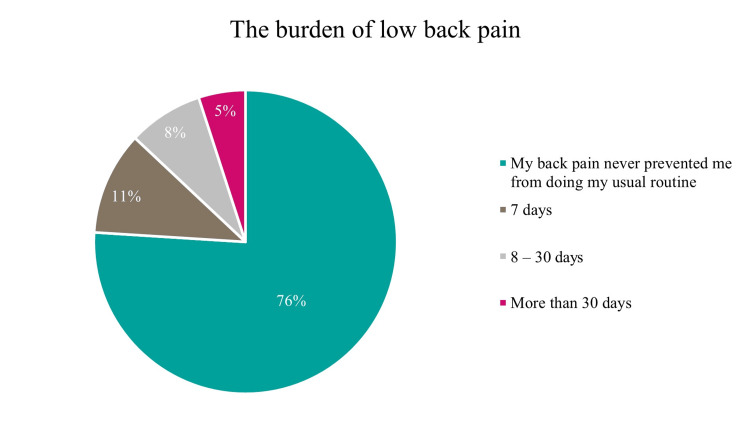 Figure 2
Figure 2| Variable | Category | N (%) |
| Age | <25 | 55 (14.1%) |
| 26-35 | 117 (30%) | |
| 36-50 | 164 (42.1%) | |
| >50 | 54 (13.8%) | |
| Education | Postgraduate | 17 (4.4%) |
| University | 203 (52.1%) | |
| Pre-university | 160 (41%) | |
| No education | 10 (2.6%) | |
| Marital status | Single | 50 (12.8%) |
| Married | 320 (82.1%) | |
| Divorced | 10 (2.6%) | |
| Widowed | 10 (2.6%) | |
| Income | <5000 SAR | 186 (47.7%) |
| 5000-10,000 SAR | 133 (34.1%) | |
| >10,000 SAR | 71 (18.2%) | |
| Number of children | 0 | 70 (17.99%) |
| 1-3 | 131 (33.68%) | |
| 4-6 | 155 (39.85%) | |
| 7-10 | 33 (8.48%) | |
| Current pregnant | Yes | 18 (4.6%) |
| No | 372 (95.4%) |
| Risk factors | Category | Frequency, n (%) |
| Nature of pain | Stiffness | 151 (42.1%) |
| Unpleasant feeling | 135 (37.6%) | |
| Numbness | 6 (1.7%) | |
| Electrical sensation | 33 (9.2%) | |
| Loss of strength | 16 (4.5%) | |
| I can’t describe | 18 (5%) | |
| Hospitalization history | Yes | 87 (24.2%) |
| No | 272 (75.8%) | |
| Pain duration (last 12 months) | 7 days | 127 (35.4%) |
| 9-30 days | 46 (12.8%) | |
| More than 30 days, but not every day | 115 (32%) | |
| Every day | 71 (19.8%) | |
| Pain burden (last 12 months) | Doesn’t affect my usual routine | 273 (76%) |
| 7 days | 40 (11.1%) | |
| 8-30 days | 29 (8.1%) | |
| More than 30 days | 17 (4.7%) | |
| Pain occurrence (last 7 days) | Yes | 225 (62.7%) |
| No | 134 (37.3%) | |
| Assumed cause of the pain | Trauma or injury | 16 (4.5%) |
| Sudden movement | 34 (9.5%) | |
| Bad posture | 154 (42.9%) | |
| Other | 155 (43.2%) | |
| Onset of the pain | Suddenly | 167 (46.5%) |
| Gradually | 192 (53.5%) | |
| Course of the pain | Intermittent | 76 (21.2%) |
| Constant | 283 (78.8%) | |
| Timing of the pain | Morning | 32 (8.9%) |
| Noon | 7 (1.9%) | |
| Evening | 30 (8.4%) | |
| Before bedtime | 57 (15.9%) | |
| Whole day | 35 (9.7%) | |
| Any time during day | 198 (55.2%) | |
| Associated symptoms | ||
| Unexplained weight loss in past few days | Yes | 36 (10%) |
| No | 323 (90%) | |
| Fever or chills at night | Yes | 41 (11.4%) |
| No | 318 (88.6%) | |
| Progressive or severe weakness in the lower extremities | Yes | 58 (16.2%) |
| No | 301 (83.8%) | |
| Progressive or severe sensory loss in the lower extremities | Yes | 74 (20.6%) |
| No | 285 (79.4%) | |
| Urine incontinence | Yes | 58 (16.2%) |
| No | 301 (83.8%) | |
| Risk factor | N | % | |
| Smoking | Never smoke | 365 | 93.6 |
| Former smoker | 12 | 3.1 | |
| Current smoker | 13 | 3.3 | |
| Weekly exercise | Very rare | 188 | 48.2 |
| 1-2 a week | 59 | 15.1 | |
| 3-5 times a week | 59 | 15.1 | |
| >5 times a week | 8 | 2.1 | |
| I don't practice physical activity | 76 | 19.5 | |
| Daily physical activity duration | 30 mins | 132 | 33.8 |
| 1 hour | 76 | 19.5 | |
| 2-3 hours | 25 | 6.4 | |
| >3 hours | 11 | 2.8 | |
| I don't practice physical activity | 146 | 37.4 | |
| Weight lifting/loading | Never | 235 | 60.3 |
| Sometimes | 133 | 34.1 | |
| Always | 22 | 5.6 | |
| Body mass index (BMI) | Underweight | 23 | 5.9 |
| Healthy weight | 122 | 31.4 | |
| Overweight | 127 | 32.6 | |
| Obese | 117 | 30.1 | |
| Variable | Category | Lower back pain | χ² (df) | p-value | |
| No | Yes | ||||
| Age | <25 | 9 (29.0%) | 46 (12.8%) | 8.543 (3) | 0.036* |
| 26-35 | 10 (32.3%) | 107 (29.8%) | |||
| 36-50 | 7 (22.6%) | 157 (43.7%) | |||
| More than 50 | 5 (16.1%) | 49 (13.6%) | |||
| Education | Postgraduate | 1 (3.2%) | 16 (4.5%) | 0.165 (3) | 0.983 |
| University | 16 (51.6%) | 187 (52.1%) | |||
| Pre-university | 13 (41.9%) | 147 (40.9%) | |||
| No education | 1 (3.2%) | 9 (2.5%) | |||
| Marital status | Single | 9 (29.0%) | 41 (11.4%) | 9.135 (3) | 0.028* |
| Married | 22 (71.0%) | 298 (83.0%) | |||
| Divorced | 0 (0.0%) | 10 (2.8%) | |||
| Widowed | 0 (0.0%) | 10 (2.8%) | |||
| Income | <5000 SAR | 16 (51.6%) | 170 (47.4%) | 2.488 (2) | 0.288 |
| 5000-10,000 SAR | 7 (22.6%) | 126 (35.1%) | |||
| >10,000 SAR | 8 (25.8%) | 63 (17.5%) | |||
| Number of children | Zero | 9 (30.0%) | 61 (17.0%) | 5.445 (3) | 0.142 |
| 1-3 | 10 (33.3%) | 121 (33.7%) | |||
| 4-6 | 11 (36.7%) | 144 (40.1%) | |||
| 7-10 | 0 (0.0%) | 33 (9.2%) | |||
| Currently pregnant | Yes | 1 (3.2%) | 17 (4.7%) | 0.148 (1) | 0.701 |
| No | 30 (96.8%) | 342 (95.3%) | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal pain and rehabilitation · Occupational Health and Performance · Spine and Intervertebral Disc Pathology
Introduction
Low back pain (LBP) is a major global health problem and a leading cause of years lived with disability worldwide. Its burden continues to increase due to population growth and aging, resulting in substantial social and economic consequences, including reduced workforce productivity [1-3].
LBP is the most prevalent chronic pain and spinal condition, affecting a large proportion of individuals at some point in their lives [4]. It is a leading contributor to disability, a common reason for healthcare utilization, and a major cause of work absenteeism in many countries, including the United States [5-7]. Globally, LBP primarily affects adults, with prevalence increasing during middle age. Although women generally report higher rates of LBP, gender-related differences are not consistent across studies, and a greater impact has been observed in households with nonworking women compared with those with employed women [8].
Previous research on LBP has predominantly focused on working populations, such as office employees, military personnel, and healthcare workers [9-14]. Consequently, the burden and characteristics of LBP among nonworking individuals remain insufficiently explored. This imbalance limits a comprehensive understanding of LBP across population groups and overlooks an important and under-researched segment of society.
This study addresses this gap by focusing on nonworking women in the Eastern region of Saudi Arabia. Understanding LBP in this population is essential, as its prevalence and impact may differ from those observed in working populations. Therefore, this study aims to evaluate the prevalence of LBP among nonworking women in the Eastern region of Saudi Arabia.
Materials and methods
A cross-sectional study was conducted in the Eastern region of Saudi Arabia from October to December 2023. Data were collected using an online questionnaire distributed via social media platforms, including WhatsApp, Instagram, Telegram, and X. The inclusion criteria comprised Arabic-speaking, nonworking Saudi women aged 18 years or older residing in the Eastern region. Nonworking status was self-reported by participants. Individuals younger than 18 years, men, working women, non-Saudi citizens, those who declined participation, and respondents who did not complete the questionnaire were excluded.
The research instrument was developed through a structured process that included a preparatory phase followed by a final revision by an expert spine surgeon certified as a consultant. During the preparatory phase, an extensive literature review was conducted, including published studies on the prevalence of LBP among nonworking women globally. Based on this review, a questionnaire was designed to assess the prevalence of LBP and its associated risk factors. The questionnaire was written in clear, straightforward Arabic. Content validity was assessed by the expert to ensure relevance, accuracy, and appropriateness. The final version of the questionnaire consisted of 32 items divided into four sections: demographic characteristics, risk factors associated with LBP, characteristics of LBP, and associated neurological symptoms. Body mass index (BMI) was calculated using the standard formula (weight in kilograms divided by height in meters squared, kg/m²) and categorized according to the World Health Organization (WHO) criteria as underweight, normal weight, overweight, or obese.
Data analysis was performed using IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize the data in frequency tables. Inferential analysis was conducted using the chi-square test to compare variables. A p-value < 0.05 was considered statistically significant.
Results
The electronic questionnaire received a total of 685 responses. Of these, 390 participants were eligible for inclusion based on the study’s inclusion and exclusion criteria, while 43 responses were excluded due to incomplete questionnaires, resulting in an acceptance rate of 56.94%.
Sociodemographic profile
As shown in Table 1, the demographic analysis of nonworking women in the Eastern region of Saudi Arabia revealed that the largest proportion of participants (42.1%) were aged 36-50 years. Most participants were married (82.1%). Regarding educational attainment, 52.1% held a university degree, while 41.0% had completed pre-university education.
Socioeconomically, Table 1 shows that 47.7% of participants reported a monthly income of <5000 SAR, 34.1% reported an income between 5000 and 10,000 SAR, and 18.2% reported an income exceeding 10,000 SAR. Family size also emerged as a relevant factor, with nearly 40% of participants having 4-6 children, suggesting a potential influence of caregiving responsibilities and associated physical demands on the occurrence of LBP.
Prevalence of LBP
The prevalence of LBP among nonworking women in the Eastern region of Saudi Arabia, as evaluated in this study, was notably high, as shown in Figure 1. A total of 359 participants (92.1%) reported experiencing LBP, while only 31 participants (7.9%) reported not having this condition.
Prevalence of low back pain among nonworking women in the Eastern region, Saudi Arabia
Characteristics of LBP
As shown in Table 2, the characteristics of LBP reported by participants varied. Stiffness was reported by 42.1% of participants, followed by an unpleasant sensation in 37.6%, numbness in 1.7%, an electrical sensation in 9.2%, and loss of strength in 4.5%. The remaining 5.0% of participants were unable to describe the nature of their pain. Regarding hospitalization history related to LBP, 24.2% of participants reported having been hospitalized, while 75.8% had not. The duration of pain over the preceding 12 months varied: 35.4% experienced pain for up to 7 days, 12.8% for 9-30 days, 32.0% for more than 30 days but not daily, and 19.8% experienced pain daily, as illustrated in Figure 2. Concerning the burden of pain during the past 12 months, 76.0% of participants reported that LBP never prevented them from performing their usual daily activities. Pain occurrence within the last 7 days was reported by 62.7% of participants, whereas 37.3% reported no pain during this period.
The burden of low back pain among the nonworking women in the Eastern region, Saudi Arabia
Risk factors
Among the nonworking women in the Eastern region of Saudi Arabia, the majority (93.6%) reported that they had never smoked, indicating a minimal contribution of smoking to LBP in this population. A small proportion of participants were former smokers (3.1%) or current smokers (3.3%). With respect to physical exercise, nearly half of the participants (48.2%) reported exercising very infrequently. Equal proportions (15.1% each) reported exercising 1-2 times per week and 3-5 times per week, while only 2.1% exercised more than five times weekly. Additionally, 19.5% reported no engagement in physical exercise.
Daily physical activity duration varied, with 33.8% reporting 30 minutes of activity per day, 19.5% reporting one hour, 6.4% reporting 2-3 hours, and 2.8% reporting more than three hours. Notably, 37.4% did not engage in any daily physical activity. Regarding weight lifting or loading activities, most participants (60.3%) reported never performing such tasks, 34.1% did so occasionally, and 5.6% engaged in these activities regularly. Body mass index (BMI) was distributed across the cohort, with 31.4% classified as underweight, 32.6% as normal weight, 30.1% as overweight, and the remainder classified as obese, indicating that LBP was observed across all BMI categories (Table 3).
Associated factors
With regard to the relationship between demographic characteristics and the prevalence of LBP, age was the only variable that showed a statistically significant association (p = 0.034) among nonworking women in the Eastern region of Saudi Arabia. As shown in Table 4, participants in the 36-50-year age group represented the highest proportion of those reporting LBP.
Table 4: Association between demographic profile and the prevalence of low back pain among nonworking women in Eastern region, Saudi Arabia*Significant (p < 0.05).
Although Table 2 indicates that LBP affected nonworking women across a wide range of lifestyles and body weight categories, association analysis revealed no statistically significant relationships between LBP and education level (p = 0.954), marital status (p = 0.061), socioeconomic status (p = 0.305), number of children (p = 1.000), or current pregnancy status (p = 0.135).
Discussion
This study demonstrates a very high prevalence of LBP among nonworking women in the Eastern Province of Saudi Arabia. The overall pattern suggests that symptoms are often persistent, commonly described as stiffness, and most prominent in midlife. Although overweight and obesity were common in this cohort, BMI did not show a statistically significant association with LBP in the present analysis.
The findings confirm the hypothesis of a high prevalence of LBP among nonworking women. Previous studies suggest that women may be biologically predisposed to LBP, particularly during the perimenopausal and menopausal periods, due to hormonal changes, reduced bone density, altered muscle function, and weight gain, all of which may increase mechanical stress on the spine [15,16]. In this study, the highest prevalence of LBP was observed among women aged 36-50 years. This may be related to a combination of physiological changes, lifestyle stressors, sedentary behavior, hormonal fluctuations, and pre-existing musculoskeletal conditions. A substantial proportion of participants with low socioeconomic status (47.4%) reported LBP, consistent with findings from previous studies [17]. Factors such as financial strain, inadequate housing, and limited access to health resources may contribute to the development and persistence of LBP. These factors are also closely linked to psychological stress, which has been associated with increased muscle tension and heightened pain perception [18-23].
Married participants were more likely to report LBP than unmarried participants, possibly reflecting increased household responsibilities, reduced opportunities for self-care, and greater emotional and physical demands. In addition, a large proportion of participants with LBP (39.8%) had four to six children, consistent with prior studies reporting a higher prevalence of LBP among women with multiple pregnancies [24]. This finding reflects the relatively larger family size among nonworking women in this region and suggests a potential cumulative physical burden related to childcare and domestic activities. Most participants with LBP (78.8%) reported persistent symptoms, with 19.8% experiencing daily pain over the preceding year. Despite this, 75.8% had no history of hospitalization for LBP. This suggests that many women may rely on self-management strategies, such as rest, home remedies, or alternative therapies, and may not seek hospital care unless symptoms become severe or disabling.
Notably, most participants with LBP (76%) reported that their pain did not interfere with their usual daily activities. This contrasts with findings from other studies that reported greater functional limitation among housewives with chronic or recurrent LBP [9]. Smoking did not show a significant association with LBP in the present study, consistent with several previous reports [14,15], although other studies have identified smoking as a risk factor for LBP [25]. Although a large proportion of participants who reported LBP were overweight (32.6%) or obese (31.5%), BMI was not significantly associated with LBP in this cohort. This finding is consistent with some studies that reported no difference in BMI between individuals with and without LBP [26], although other studies have demonstrated a positive association between higher BMI and LBP [14,15,24]. Weight reduction and lifestyle modification may nonetheless be beneficial, as excess body weight can increase spinal load and negatively affect musculoskeletal health. Physical inactivity was common in this population, with nearly half of participants reporting infrequent exercise and over one-third reporting no regular physical activity. Sedentary behavior may increase susceptibility to LBP by contributing to muscle weakness and poor postural control. Regular physical activity is known to strengthen supporting musculature and improve spinal stability, potentially reducing LBP risk. However, further studies are needed to clarify the role of exercise in this specific population. Prior research has identified a lack of regular physical activity as a risk factor for LBP in other groups, including healthcare workers [27].
Understanding the prevalence and associated factors of LBP in specific populations is essential for effective prevention and management strategies. This study highlights the potential contribution of poor sitting habits to LBP, as reported in earlier literature [27]. Public health initiatives that promote ergonomic awareness, physical activity, and healthy lifestyle practices may help reduce the burden of LBP and improve the quality of life among nonworking women. Several limitations should be acknowledged. The absence of a psychological assessment limits the evaluation of psychosocial contributors to LBP. Coexisting medical conditions were not analyzed, which may have influenced pain prevalence. The relatively limited sample size restricts generalizability and may increase the risk of selection bias. Sleep patterns and sleep disorders, which may have a bidirectional relationship with LBP, were not assessed. Finally, the use of an online, self-administered questionnaire introduces potential sampling and self-report bias, including recall bias and social desirability bias. Future studies should address these limitations by incorporating psychological variables, medical comorbidities, objective measures, and larger, more representative samples to further elucidate the determinants of LBP in this population.
Conclusions
LBP appears to be highly prevalent among nonworking women in the Eastern Province of Saudi Arabia, with age emerging as the only factor significantly associated with LBP in this sample. Notably, many women reported continuing their usual daily activities despite symptoms, suggesting that LBP in this group may be underrecognized and underaddressed rather than absent. These findings highlight the need for proactive community awareness, early assessment, and access to conservative management strategies, including education, exercise guidance, and ergonomic advice, particularly for women in midlife. Given the cross-sectional, self-reported, online design of this study, future research should incorporate validated pain and disability measures and evaluate healthcare-seeking behavior, psychosocial factors, and comorbidities to better define functional impact and identify modifiable contributors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A systematic review of the global prevalence of low back pain Arthritis Rheum Hoy D Bain C Williams G 202820376420122223142410.1002/art.34347 · doi ↗ · pubmed ↗
- 2Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015 Lancet GBD 2015 Disease and Injury Incidence and Prevalence Collaborators 1545160238820162773328210.1016/S 0140-6736(16)31678-6PMC 5055577 · doi ↗ · pubmed ↗
- 3Prevalence of chronic low back pain: systematic review Rev Saude Publica Meucci RD Fassa AG Faria NM 149201510.1590/S 0034-8910.2015049005874 PMC 460326326487293 · doi ↗ · pubmed ↗
- 4Prevalence of low back pain in the elderly population: a systematic review Clinics (Sao Paulo) de Souza IM Sakaguchi TF Yuan SL Matsutani LA do Espírito-Santo AS Pereira CA Marques AP 074201910.6061/clinics/2019/e 789PMC 680768731664424 · doi ↗ · pubmed ↗
- 5Years lived with disability (YL Ds) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010 Lancet Vos T Flaxman AD Naghavi M 2163219638020122324560710.1016/S 0140-6736(12)61729-2PMC 6350784 · doi ↗ · pubmed ↗
- 6Measuring the global burden of low back pain Best Pract Res Clin Rheumatol Hoy D March L Brooks P Woolf A Blyth F Vos T Buchbinder R 1551652420102022763810.1016/j.berh.2009.11.002 · doi ↗ · pubmed ↗
- 7Characteristics of physician visits for back symptoms: a national perspective Am J Public Health Cypress BK 389395731983621958810.2105/ajph.73.4.389PMC 1650784 · doi ↗ · pubmed ↗
- 8Low back pain: a call for action Lancet Buchbinder R Tulder M Öberg B 238423883912018 https://www.thelancet.com/journals/lancet/article/PIIS 0140-6736(18)30488-4/abstract 2957387110.1016/S 0140-6736(18)30488-4 · doi ↗ · pubmed ↗