Isolated mediastinal lymphangioma in a child: A rare case report
Ankita Gupta, Maheswar Chaudhury, Manoranjan Khuntia, Peeta H. Prasad, Somadatta Das

TL;DR
A rare case of a mediastinal lymphangioma in a young child is reported, emphasizing the importance of accurate diagnosis using multiple imaging techniques.
Contribution
This case report provides insights into the radiological features of isolated mediastinal lymphangioma in children.
Findings
Multimodal imaging confirmed a diagnosis of mediastinal cystic lymphangioma with internal haemorrhage.
Surgical excision and histopathology confirmed the diagnosis of cystic lymphangioma.
Accurate diagnosis helps avoid unnecessary interventions and complications.
Abstract
The mediastinum is an unusual location for cystic lymphangiomas. An 18-month-old male presented with acute fever, dry intermittent cough and respiratory distress. Chest radiography, ultrasonography, contrast-enhanced CT and MRI suggested a diagnosis of mediastinal cystic lymphangioma with internal haemorrhage. Surgical excision of the lesion and histopathological examination confirmed cystic lymphangioma. This case highlights the multimodal radiological features of isolated mediastinal cystic lymphangioma for accurate diagnosis and improved management, to avoid unnecessary interventions and complications.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
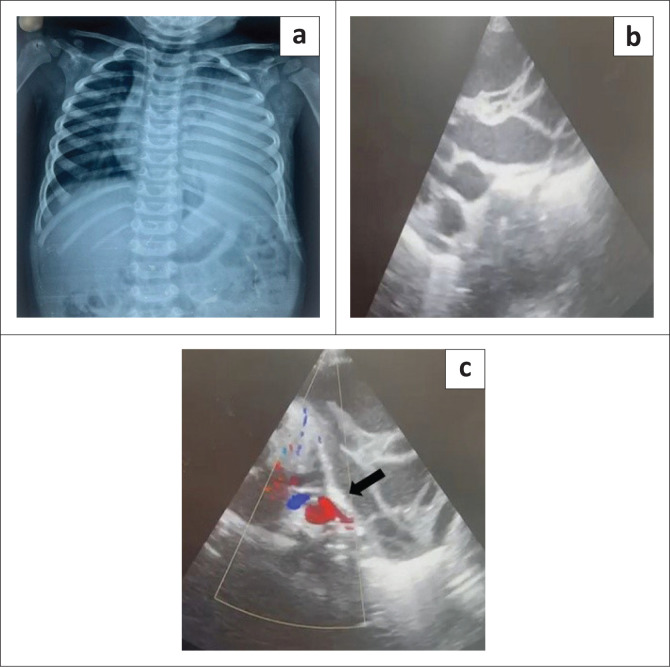 FIGURE 1
FIGURE 1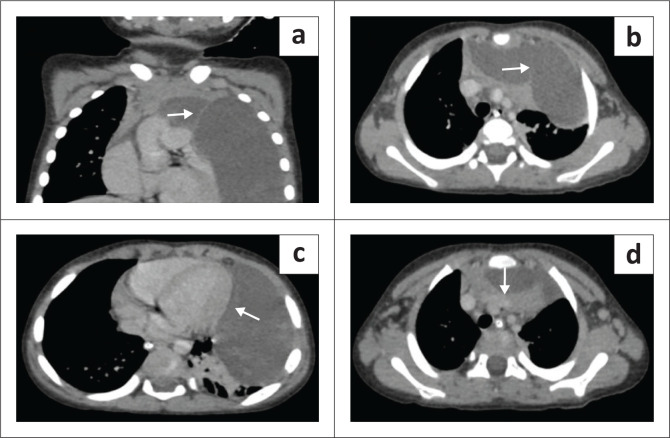 FIGURE 2
FIGURE 2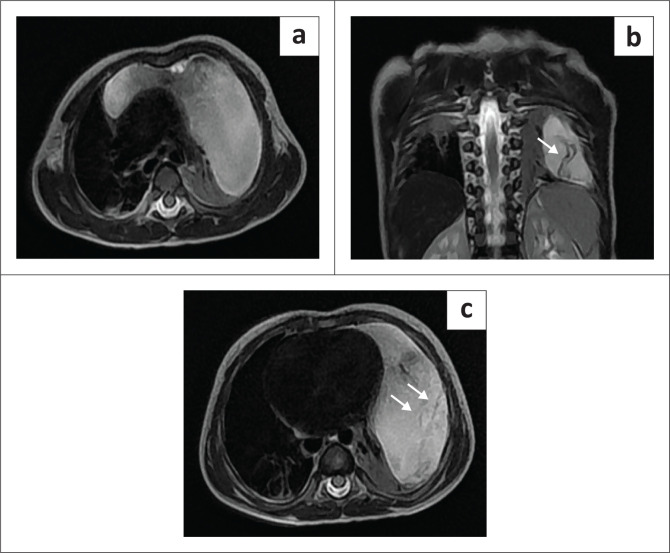 FIGURE 3
FIGURE 3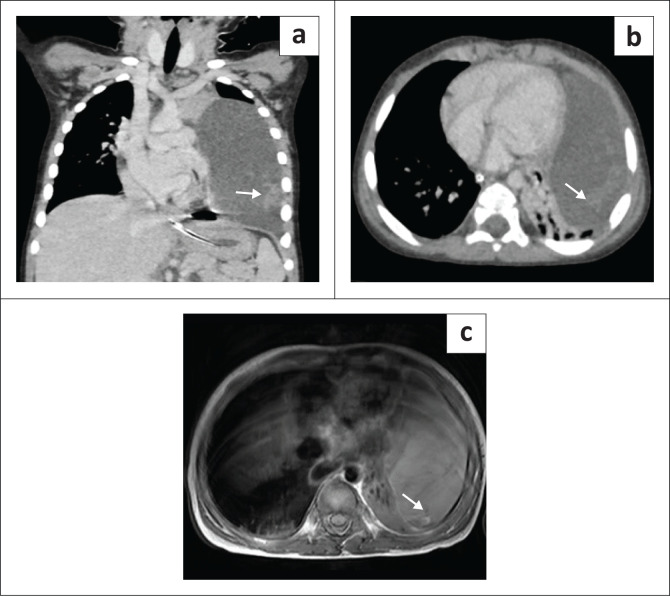 FIGURE 4
FIGURE 4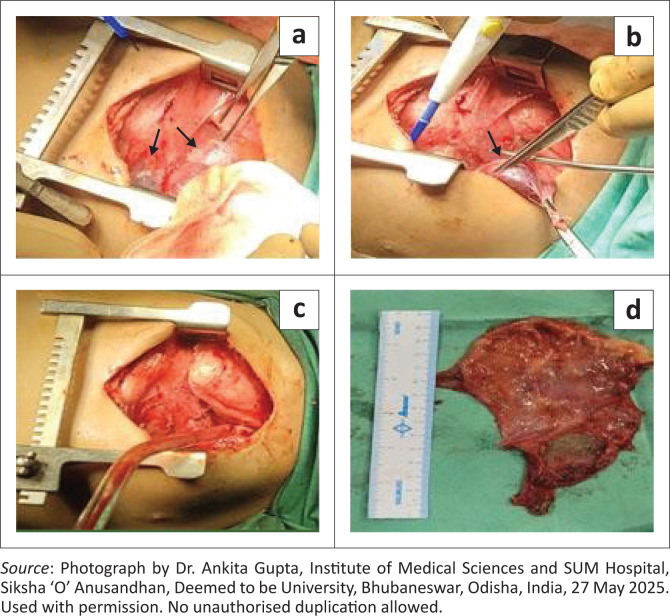 FIGURE 5
FIGURE 5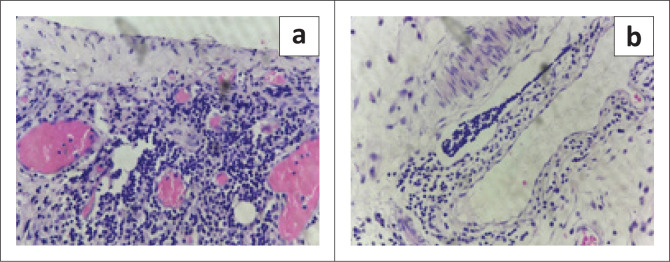 FIGURE 6
FIGURE 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations and Hemangiomas · Lymphatic Disorders and Treatments · Myasthenia Gravis and Thymoma
Introduction
Solitary cystic lymphangioma is an uncommon congenital benign vascular tumour caused by a malformation of the lymphatic vessels. Lymphangiomas can affect any site in the body, most commonly the cervical (75%) and axillary regions (20%). Less than 1% of lymphangiomas are mediastinal.^1^ Most mediastinal lymphangiomas are located in the anterior mediastinum.
Lymphangiomas, although benign, can present with complications such as infection, cystic haemorrhage, superior vena cava syndrome, airway compromise, chylothorax and chylopericardium.^2^ Landing and Farber classified lymphangiomas into three categories:
simple or capillary lymphangioma – dilated, capillary-sized lymphatic vessels connected to a normal lymphatic networkcystic lymphangioma – multiple large cyst-like spaces lined by flat endothelial cells; the cystic spaces may be empty or filled with clear proteinaceous or chylous fluid containing lymphocytes, or occasionally red blood cellscavernous lymphangioma – dilated lymphatic sinuses in an actively growing lymphoid stroma, also connected to normal lymphatics.^3,4^
A compilation of clinical presentation, radiological imaging and histopathological investigation aids in diagnosing lymphangioma. A case of anterior mediastinal cystic lymphangioma with chief complaints of fever, intermittent cough and excessive crying in an 18-month-old male is presented.
Ethical considerations
Written informed consent was obtained from the legal guardian of the patient.
Patient presentation
An 18-month-old male was admitted to a tertiary care hospital for persistent fever and intermittent dry cough associated with excessive crying. He was delivered at term as the 1st order twin (the 2nd twin was stillborn), requiring admission to the neonatal intensive care unit for early-onset sepsis on day 2 of life, for which he received antibiotics and was discharged with no subsequent illness documented. On admission, physical examination revealed decreased air entry in the left mammary, infra-mammary and infra-axillary regions. The patient was febrile and irritable, with a per-abdominal examination suggesting hepatomegaly. An initial suspicion of meningitis was made, for which IV fluids and empiric antibiotics were commenced. Examination of the CSF revealed two white cells/µL, excluding meningitis.
Chest radiography revealed a homogeneously opacified left hemithorax, silhouetting the ipsilateral cardiac margin and hemidiaphragm, and a widened mediastinum (Figure 1a). Ultrasound with Doppler of the thorax showed a well-defined, multiseptated, cystic lesion in the left hemithorax measuring 8 × 4 cm, abutting the pericardium (Figure 1b and Figure 1c). Contrast-enhanced CT (CECT) of the thorax with angiography was advised to exclude congenital pulmonary airway malformation (CPAM). Imaging with CT revealed a large, non-enhancing, septated, cystic lesion measuring 8.7 × 8.5 × 6.4 cm,without a perceptible wall, in the anterior mediastinum and left hemithorax (Figure 2a and Figure 2b). The mass extended to the superior mediastinum but did not involve the neck, abutting the right mediastinal pleura and pericardium and indenting the anterior wall of the thymus, causing secondary collapse of the left lung basal segments and deviation of the trachea to the right (Figure 2c and Figure 2d). The MRI showed a large T2 hyperintense cystic lesion with thin septations in the anterior mediastinum and left hemithorax compressing the left lung, consistent with the CECT findings (Figure 3). Dependent, non-enhancing, hyperdense content within the lesion on the CT scan corresponded to T1 hyperintensity on the MRI, likely indicating haemorrhage (Figure 4).
(a) Chest radiograph revealing a large homogeneous opacity in the left hemithorax silhouetting the left cardiac margin and ipsilateral hemidiaphragm, and a widened mediastinum. (b) Ultrasound demonstrating a well-defined, multiseptated cystic lesion in the left hemithorax. (c) Doppler ultrasound indicates the lesion abutting the pericardium (black arrow).
(a, b) Contrast-enhanced CT (CECT) revealing a large, non-enhancing, cystic lesion without a perceptible wall, occupying almost the entire left hemithorax, extending to the superior mediastinum and demonstrating non-enhancing septations (white arrows). (c) The lesion is abutting the pericardium (white arrow). (d) Axial CECT shows the lesion indenting the anterior wall of the thymus (white arrow).
(a) Axial T2 MRI showing a large, hyperintense, cystic lesion in the anterior mediastinum and left hemithorax, compressing the left lung. (b, c) Coronal and axial T2-weighted MRI demonstrates septations within the lesion (white arrows).
(a, b) Contrast-enhanced CT (CECT) coronal and axial images show hyperdense content within the lesion, suggestive of haemorrhage (white arrows). (c) Axial non-contrast T1-weighted MRI shows hyperintensity, indicating haemorrhage (white arrow).
Following a suggested diagnosis of mediastinal cystic lymphangioma complicated by internal haemorrhage, median sternotomy with excision of the anterior mediastinal cystic mass (Figure 5) was performed under general anaesthesia. Histopathological examination revealed fibro-adipose tissue, cystic spaces lined by a corrugated, single layer of cuboidal epithelium and adjacent fibrovascular connective tissue showing dense lymphoplasmacytic infiltrates and scattered, dilated mature lymphocytes, suggesting a benign vascular malformation compatible with lymphangioma (Figure 6). The patient developed a Candida infection at the central line site on day 10 post-surgery, for which antifungals and antibiotics were administered. The patient was discharged on day 12 post-surgery.
(a, b) Anterior mediastinal cystic mass (black arrows), (c) post-excision, and (d) excised cystic lymphangioma.
(a) Cystic space revealing a dense lymphoid aggregate and proliferated capillaries. (b) Dilated lymphatic channels containing mature lymphocytes.
Discussion
Cystic lymphangiomas most commonly develop superficially on the body surface and are often detected before the age of 2 years.^1,5^ Only 2% – 3% of the cervical lymphangiomas may be associated with an intrathoracic extension. An isolated mediastinal lymphangioma without a cervical component is rare, accounting for less than 1%.^5^ The child in the presented case had an isolated mediastinal cystic lymphangioma without any cervical component.
Cystic lymphangiomas are usually asymptomatic until they reach dimensions large enough to cause compression of the adjacent structures, leading to respiratory distress and causing internal haemorrhage at a later stage of progression.^6,7^ The index patient presented with respiratory distress, which required supportive treatment pre-operatively.
The differential diagnosis of an anterior mediastinal lymphangioma includes bronchogenic cyst (well defined, non-enhancing, homogeneous cystic lesion with thin smooth walls in the carinal, paratracheal, oesophageal or retrocardiac areas); pericardial cyst; duplication cyst (features same as bronchogenic cyst with their location being the differentiating feature); necrotic neoplasm (thick- or irregular-walled mass on CT); thymic cyst (imperceptible, thin-walled unilocular cyst if congenital and multiloculated cyst associated with thymic neoplasias if acquired); haematoma, seroma or abscess (low-attenuation mass with an enhancing rim); as well as mature teratoma (cystic mediastinal mass with a combination of multiple tissue elements – fat and cystic components or fat-fluid level within the mass on CT and a heterogenous mediastinal mass with a variable mixture of fat, fluid, soft tissue and calcification on MRI).^8^ Shape, cyst wall thickness, intracystic septations, presence of a solid component, fat, or calcification, and infiltration of surrounding structures are the differentiating criteria between benign congenital cysts and other cyst-like lesions.^9^
Lymphangiomas can also mimic recurrent pleural effusion, which may lead to unnecessary interventional procedures. This further highlights the importance of multimodal imaging investigations for the assessment and diagnosis of lymphangiomas. Although unusual, lymphangiomas should be considered as a differential in cases of recurrent thoracic fluid accumulation.^10,11,12^ Ultrasound, being a non-invasive, cost-effective and non-radiation imaging modality, is considered the first level investigation for a mass suspicious of cystic lymphangioma. It is then integrated with higher modalities such as CT and MRI to obtain additional information such as structural features, internal and peripheral contrast enhancement, as well as loco-regional lesion spread. Radiological imaging plays an important role in excluding malignancy and providing the exact anatomic location of the mass before surgery.^13^
Surgical excision of the mass is the treatment of choice and a confirmatory diagnosis is made through histopathological examination.^7^ In the case presented, the patient underwent open sternotomy with excision of the space-occupying lesion under general anaesthesia. Post-operative complications include infection, chylothorax, fistula formation, injury to the phrenic nerve, vagus nerve, lungs, or major vessels.^7^ In the index patient, the whole tumour was resected successfully. The chances of recurrence are lower following a complete resection, which is otherwise relatively common (35% vs. 6% recurrence in the case of complete resection).^14^ Follow-up is therefore indicated for any event of recurrence. If complete surgical resection is deemed inconvenient, as in cases of large tumour size, mediastinal or neurovascular bundle infiltration, or multiple loculations, chemotherapy, radiotherapy, and sclerotherapy combined with partial resection can be considered as alternative treatments with varied results.^12,15^
Conclusion
This report describes a case of an isolated mediastinal cystic lymphangioma without any cervical component, contributing to existing literature based on its rarity and unusual location.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Minato H, Kaji S, Kinoshita E, et al. Solitary intrapulmonary cystic lymphangioma in an infant: A case report with literature review. Pathol Res Pract. 2006;206(12):851–856. 10.1016/j.prp.2010.09.00420952134 · doi ↗ · pubmed ↗
- 2Bender B, Murthy V, Chamberlain RS. The changing management of chylothorax in the modern era. Eur J Cardio-Thorac Surg. 2015;49(1):18–24. 10.1093/ejcts/ezv 04125732972 · doi ↗ · pubmed ↗
- 3Landing BH, Farber S. Tumors of the cardiovascular system. Atlas of tumor pathology. Washington, DC: Armed Forces Institute of Pathology; 1956.
- 4Copeland J, Müller KM, Müller AM. Pulmonary haemangiolymphangioma – A new entity of pulmonary vascular tumours? Histopathology. 2008;52(4):527–529. 10.1111/j.1365-2559.2008.02946.x 18315611 · doi ↗ · pubmed ↗
- 5Khalilzadeh S, Hassanzad M, Cheraghvandi A, Abdollah MP, Khodayari AA, Javaherzadeh M. Mediastinal lymphangioma in a child. Tanaffos. 2012;11(2):58–60.25191417 PMC 4153197 · pubmed ↗
- 6Riquet M, Briere J, Le Pimpec-Barthes F, et al. Les lymphangiomes kystiques du cou et du médiastin: existe-t-il des formes acquises? A propos de 37 cas [Cystic lymphangioma of the neck and mediastinum: Are there acquired forms? Report of 37 cases]. Rev Mal Respir. 1999;16(1):71–79.10091263 · pubmed ↗
- 7Correia FM, Seabra B, Rego A, Duarte R, Miranda J. Cystic lymphangioma of the mediastinum. J Bras Pneumol. 2008;34(11):982–984. English, Portuguese. 10.1590/S 1806-3713200800110001519099107 · doi ↗ · pubmed ↗
- 8Odev K, Arıbaş BK, Nayman A, Arıbaş OK, Altınok T, Küçükapan A. Imaging of cystic and cyst-like lesions of the mediastinum with pathologic correlation. J Clin Imaging Sci. 2012;2:33. 10.4103/2156-7514.9775022919547 PMC 3424852 · doi ↗ · pubmed ↗