Utilization of mental health services during the first year of the COVID-19 pandemic – a systematic review and meta-analysis
Miriam Glock, Antranik Erdekian, Mike Rueb, Francesca Uhl, Ronja Husemann, Jutta Stoffers-Winterling, Saskia Lindner, Oliver Tüscher, Lars Peer Hölzel, Klaus Lieb, Kristina Adorjan, Hauke Felix Wiegand

TL;DR
This study shows how mental health service use changed during the early stages of the COVID-19 pandemic, with fewer inpatient visits and more telemedicine use.
Contribution
The study provides a comprehensive meta-analysis of mental health service utilization changes during the initial phase of the pandemic.
Findings
Inpatient mental health services saw a significant decrease during the pandemic.
Telemedicine use increased significantly compared to pre-pandemic levels.
Psychotropic medication prescriptions remained largely unchanged.
Abstract
The COVID-19 pandemic presented significant challenges to infectious disease management and mental health services (MHS). Service demand and delivery changed due to fear of infection, economic hardships, and the psychological effects of protective measures. This systematic review with meta-analysis aims to quantify these impacts on different mental health service settings. Comprehensive searches were conducted in PubMed, Embase, and PsycINFO, focusing on studies published from the initial outbreak of COVID-19, starting in November 2019. Studies were included comparing the utilization of mental health inpatient, emergency department (ED), and outpatient services (including telemedicine and medication prescriptions) before and during the COVID-19 pandemic. A random-effects model was employed to estimate pooled effects, with study quality assessed using a modified Newcastle-Ottawa Scale.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
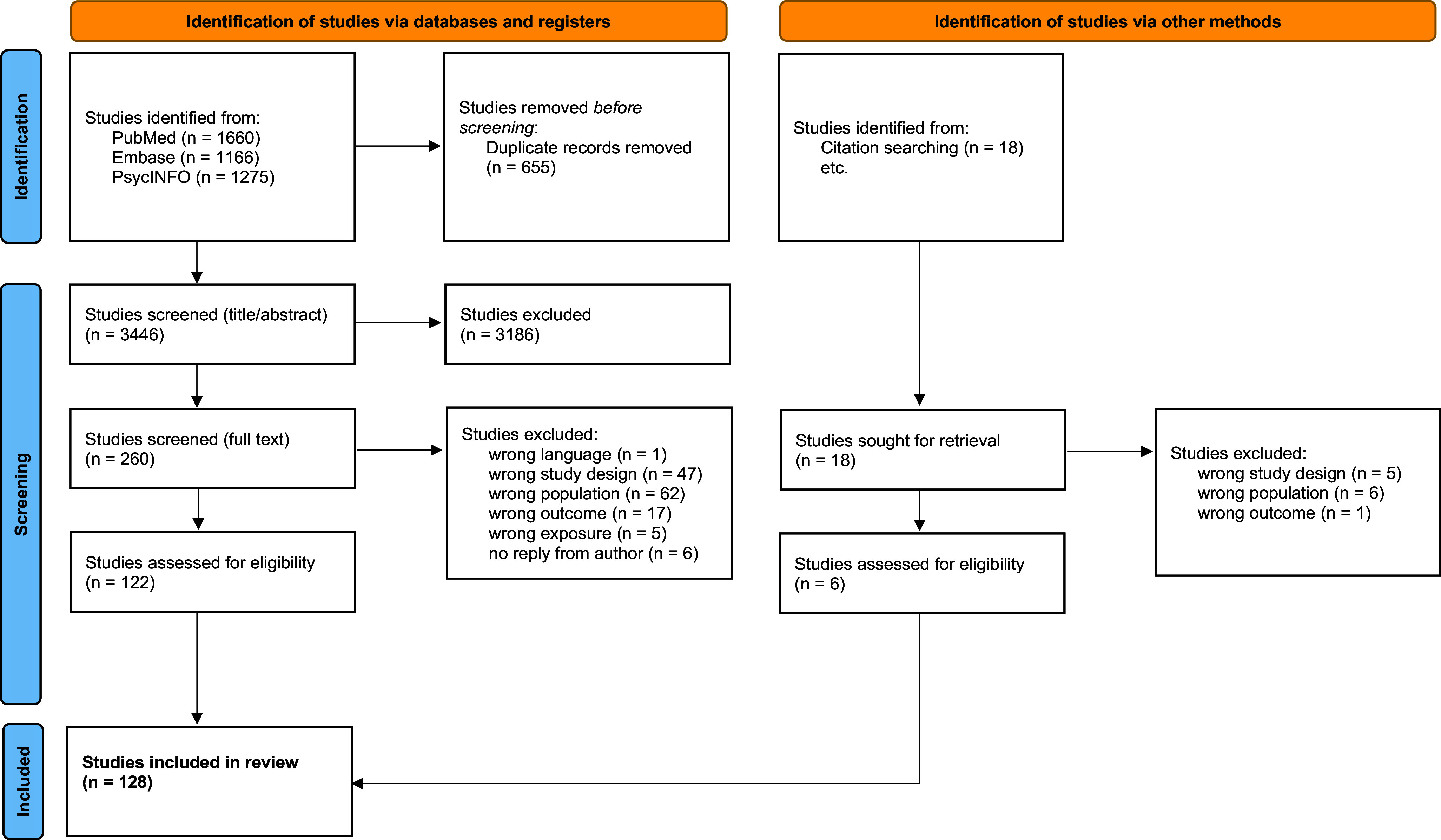 Figure 1
Figure 1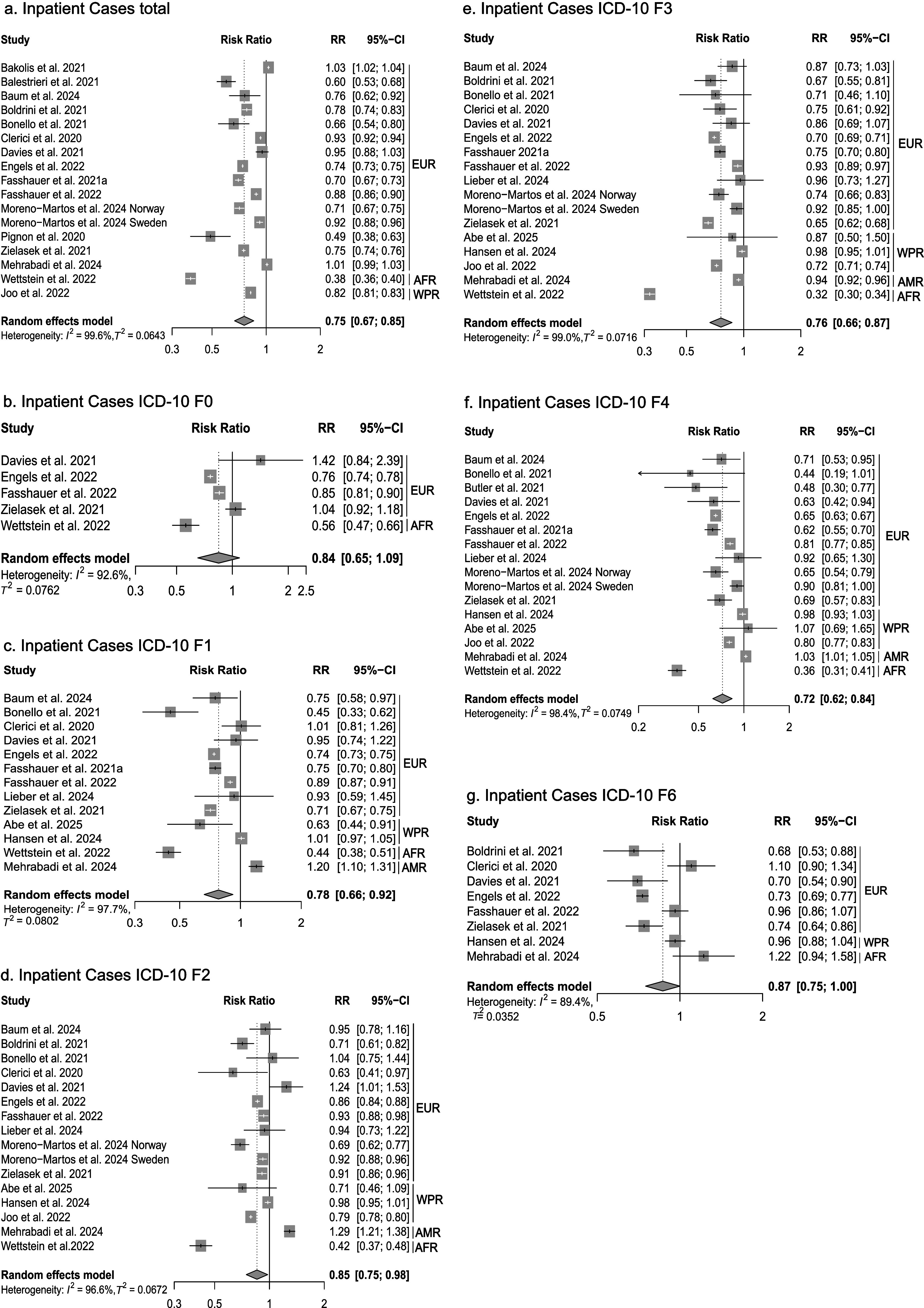 Figure 2
Figure 2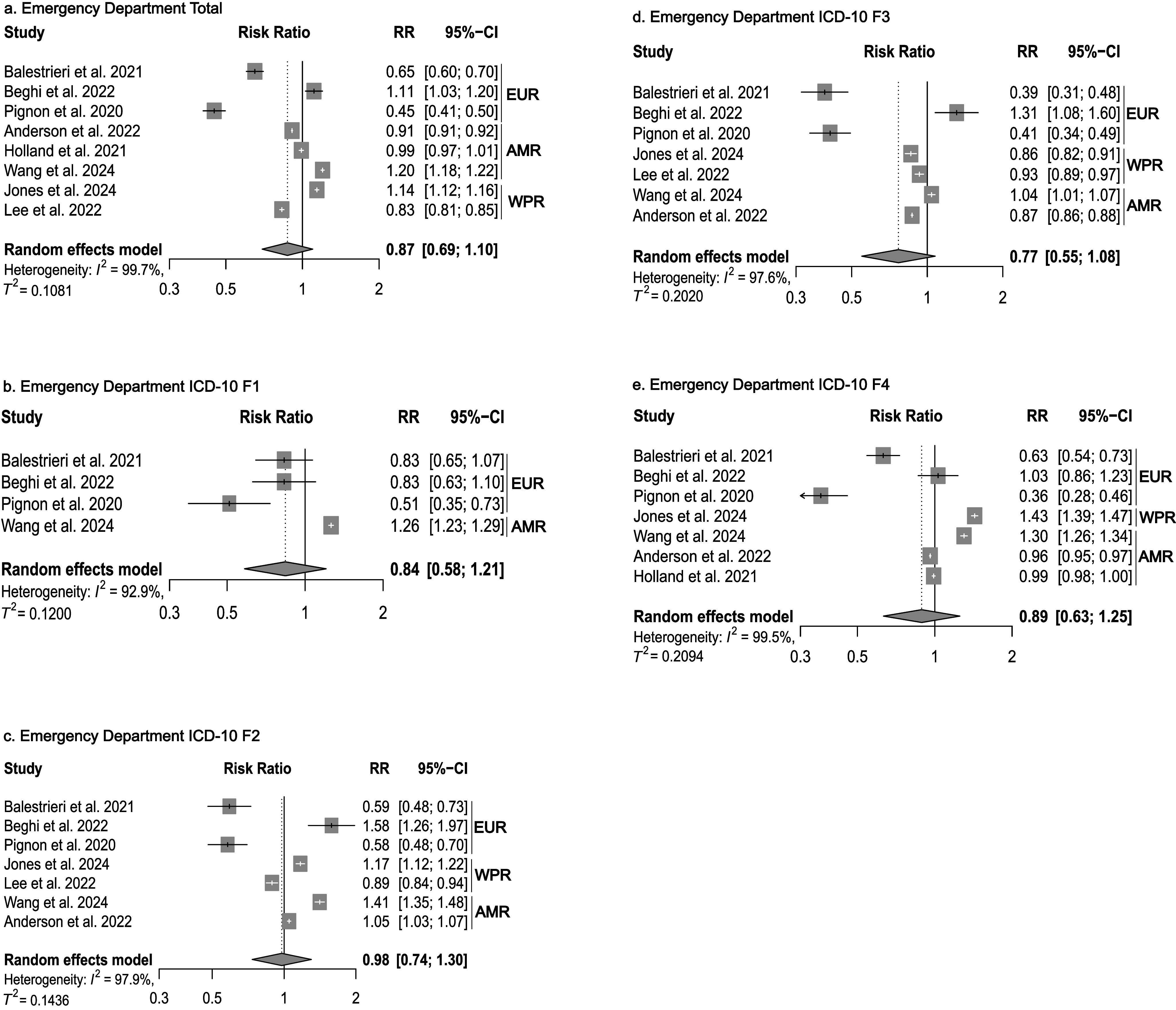 Figure 3
Figure 3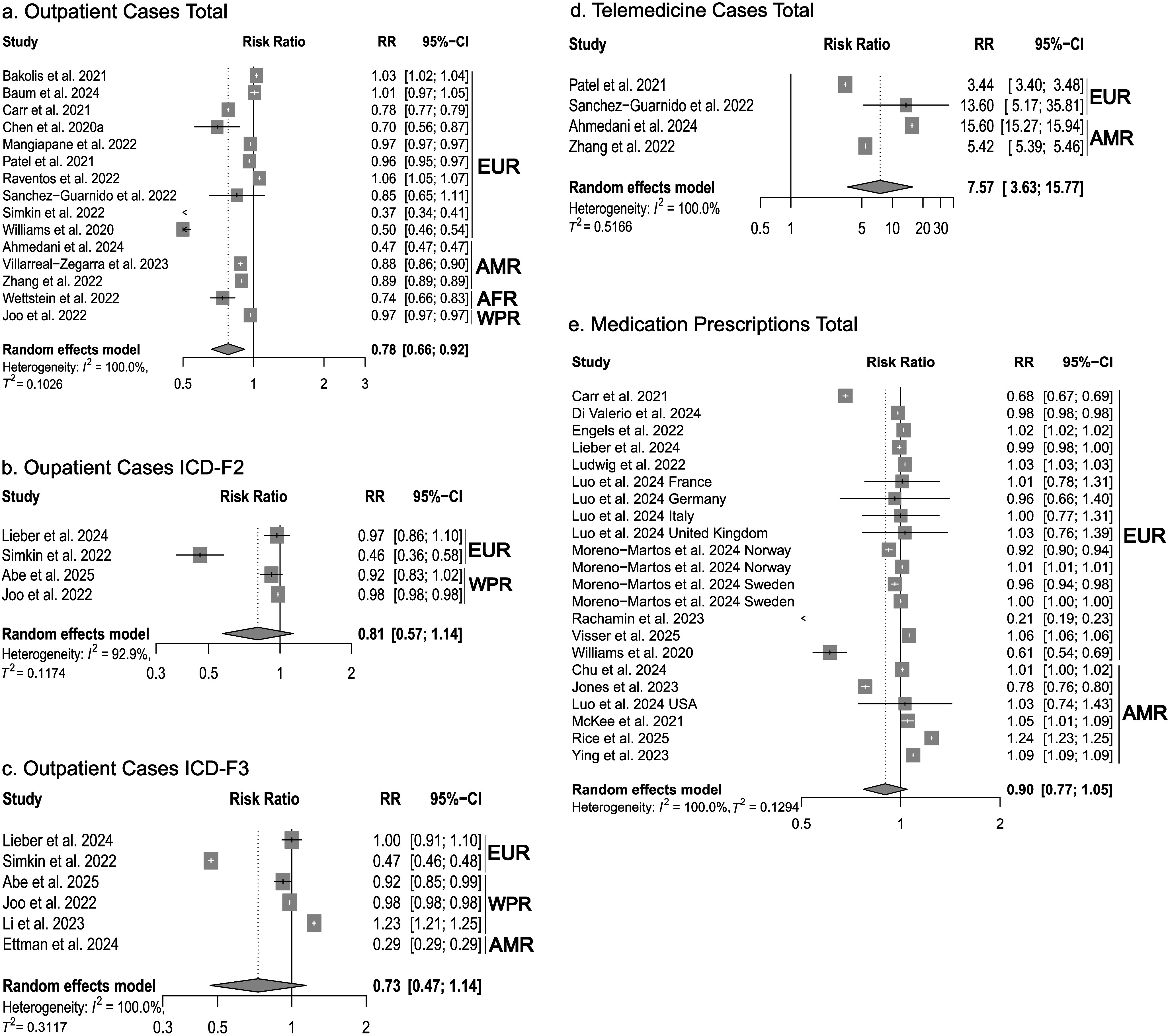 Figure 4
Figure 4 Figure 5
Figure 5- —Bundesministerium für Bildung und Forschunghttps://doi.org/10.13039/501100002347
- —Bundesministerium für Bildung und Forschunghttps://doi.org/10.13039/501100002347
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and Mental Health · Telemedicine and Telehealth Implementation · COVID-19 and healthcare impacts
Introduction
The COVID-19 pandemic posed a challenge not only for infectiology and intensive care but also for other essential healthcare services [1], such as mental health services (MHS). Fears of infection, post-COVID syndromes, the psychological effects of infection control measures, and economic hardships may have led to changes in the demand for MHS [2–4]. Similarly, infection control measures, resource reallocations, a focus on somatic medicine, and changes in incentive structures may have—among other factors—altered the provision of mental healthcare services [5–7].
Several studies have reviewed the effects of the COVID-19 pandemic on MHS utilization. In a systematic review, Duden et al. [8] narratively synthesized the evidence regarding challenges and changes in global MHS during the pandemic. They reported reductions in demand, access, referrals, admissions, and caseloads during the initial phases of the pandemic, followed by normalizations or even increases later on. They interpreted their results as evidence that community MHS were quite adaptable and resilient to the challenges posed by the pandemic. Another global trend was the introduction of telemedicine services [8]. Steeg et al. [9] examined presentations to MHS following self-harm. They reported a reduction in the first month of the pandemic in 2020 but a trend toward normalization in 2021 and even an increase in service use among adolescent girls. However, these latter results were based on a limited number of studies [9]. Wan Mohd Yunus et al. systematically reviewed studies on service use in children, adolescents, and young adults aged 0 to 24 years. They found decreases in service use during the early phases of the pandemic. They interpreted these findings as potentially indicative of delayed treatment and unmet needs [10]. In their systematic review of MHS use, Ahmed et al. reported decreases in inpatient admissions by 11–43%, presentations to emergency departments and walk-in services by 14–58%, and community mental health and outpatient services by 24–75%, alongside a shift from in-person to telemedicine contacts [11]. Inpatient services remained below pre-pandemic levels in late 2020 and 2021, whereas community mental health and outpatient services reported higher-than-pre-pandemic utilization [11].
These existing reviews have some limitations in estimating the effect of the pandemic on MHS utilization. They were either restricted to defined syndromes [9] or services [10] or provided only narrative syntheses [8, 11]. Furthermore, it is important to account for the considerable heterogeneity in the level of observation of the studies on MHS utilization, which ranged from single emergency departments to entire countries. Therefore, we conducted a systematic review and meta-analysis of the global literature on MHS utilization. Such a synthesis of study results is of high relevance for discussions on the evaluation of pandemic response measures in the context of their impacts on other areas of care, and for learning from a comprehensive picture of changes in order to be better prepared for future crisis situations.
Methods
Inclusion and exclusion criteria
We included studies that examined the utilization of the mental healthcare system and compared the period before the COVID-19 pandemic with the period during the COVID-19 pandemic, to quantify changes to pre-pandemic utilization levels. We excluded studies that only compared periods during the pandemic with intervals after the pandemic, because of assumed changes in offerings and utilization patterns in some areas of MHS after the pandemic. We only focused on studies employing quantitative research methodologies, including longitudinal studies (prospective and retrospective), cohort studies, and analyses of routine data, while excluding qualitative research. Results were categorized into three service types: inpatient, emergency department (ED), and outpatient services. Additionally, outpatient telemedicine services and outpatient medication prescriptions were examined separately. Inpatient services included planned inpatient hospitalizations, emergency inpatient admissions, or admissions resulting from visits to emergency departments. Outpatient services encompassed general practitioner visits, mental health specialist visits, outpatient telemedicine services (e.g., video calls, phone calls), individual or group psychotherapy, and outpatient prescriptions for psychotropic medications. A detailed overview of the settings for each study is provided in the supplementary material (Supplementary Material Figure S6). Only studies involving populations with a known or newly diagnosed mental disorder according to ICD-10 or DSM-5 were included. Participants had to be 18 years of age or older. In cases where the population age was not clearly stated or where there were mixed adult and adolescent populations, the authors were contacted to confirm that the study either did not include or only minimally (cutoff <15% of patients) included individuals under 18 years of age. Studies that focused on suicide or suicide attempts but not diagnosed mental disorders or utilization, as well as case reports, qualitative surveys, intervention studies, commentaries, and discussion papers, were excluded.
Search strategy and screening process
The methods of this systematic review were predefined and registered in the International Prospective Register of Systematic Reviews (PROSPERO, registration number CRD42022334792) [12] and were conducted according to the PRISMA guidelines [13]. We searched Embase for English-, French-, and German-language sources published from November 2019—the time when the COVID-19 disease first emerged and later developed into a pandemic—up to July 2022, and PubMed and PsycINFO from November 2019 until 30.03.2025.
The search strategy combined terms related to COVID-19 (e.g., “COVID-19,” “SARS-CoV-2,” “2019-nCoV”) and mental health (e.g., “mental health,” “mental disorders,” “psychiatric disorders”) using both free-text terms and controlled vocabulary (MeSH terms). The Supplementary Material (Supplementary Material Figure S9) presents the complete search strategy for the three databases. Using Endnote [14], the studies identified were imported into Covidence [15] for title/abstract and full-text screening. To identify additional references, we manually searched the reference lists of the identified reviews. After duplicates were removed, the reviewers performed the title, abstract, and full-text screenings in tandems of two.
Data extraction
We extracted the following data from each study: authors, study characteristics (aim of study, study design, country, setting, time periods considered), population details (age, gender), the number of visits or consultations in the respective setting, and psychiatric diagnoses according to ICD-10 or DSM-5 (for details, see Table 1). Two independent reviewers conducted the data extraction process, resolving discrepancies through discussion or consensus within the review group.Table 1.Characteristics of the included studiesStudyCountrySettingSelected data collection periodsStudy aimNumber of study participants (n)Diagnostic groups according to ICD-10, when subdivided into F-diagnosesBefore COVID-19During COVID-19BeforeCOVID-19During COVID-191Abe et al. 2025JapanInpatient, outpatientApril to December 2019April to December 2020Examine whether access to outpatient and inpatient care for psychiatric conditions was maintained in Japan during the pandemicTotal participants: 82467 RR values were taken directly from the original studyF0-F42Adorjan et al. 2021GermanyInpatientApril to May 2019April to May 2020Average number of inpatient and day-care psychiatric treatments in 38 clinics68404218total3Ahmedani et al. 2024USAOutpatient, telemedicineJune 2019 to March 2020March to December 2020Examine population-level disruption in psychotherapy before and after the rapid shift to virtual mental health care in the United States28,4826270,794total4Akkaoui et al. 2025FranceEDJanuary to December 2019January to December 2020description of the trends in the number of visits to the largest psychiatric emergency department in FranceTotal participants: 69,764. percentage reduction reported. 23.9% decrease in 2020total5Alves et al. 2021PortugalED, inpatient March to May 2019March to May 2020visits to the psychiatric ED and hospitalizations of a hospital center349158F1-F76Ambrosetti et al. 2021SwitzerlandED, inpatientApril to May 2016April to May 2020presentations to the adult psychiatric ED of the University Hospital of Geneva, admissions in consequence of visits702579F0, F1, F3, F4, F57Anderson et al. 2022USAEDFebruary to March 2019February to March 2021Mental health related ED visits from more than 3600 facilities from 49 states and District of Columbia265,682242,258F2-F6 8Andersson et al. 2022 SwedenOutpatientJanuary to December 2019March to May 2019January to December 2020March to May 2020Number of alcohol-attributable admissions at an addiction-specialized treatment facility18031675total9Bakolis et al. 2021 United KingdomInpatient, outpatient January to March 2020March to June 2020Changes in inpatient care and community services from 10 UK providers65,80761,301total10Balestrieri et al. 2021ItalyED, inpatientMarch to May 2019March to May 2020Psychiatric consultations in 9 Italian hospital EDs, consultations that led to admissions16491075F0-F411Baum et al. 2024GermanyInpatient, outpatientMarch 2019 to February 2020March to May 2020Changes in utilization in the German mental health care inpatient and outpatient mental health care systemTotal participants: 2,294,091 RR values were taken directly from the original studyF1-F412Beghi et al. 2022ItalyEDMay to August 2019May to August 2020Emergency room psychiatric consultations at all 7 public hospitals of AUSL Romagna12201358F0-F613Berardelli et al. 2021ItalyInpatientMay 2019 to March 2020March to December 2020Adult psychiatric inpatients consecutively admitted to the psychiatric unit of Sant ‘Andrea Hospital315317F2-F614Bhagavathula et al. 2024USATelemedicineJanuary to December 2019January to December 2020Impact of the COVID–19 pandemic on utilization of telehealth services for SUDs and MHC in ND and MN25,2371,181,248F115Boldrini et al. 2021ItalyInpatientMarch to June 2018/2019March to June 2020Psychiatric admissions in 12 general psychiatric wards32701280F2, F3, F616Bonello et al. 2021MaltaInpatientMarch to June 2019March to June 2020Admissions to the only national mental health facility in Malta262172F1-F417Bruckner et al. 2023USAEDJanuary 2018 to March 2020March to May 2020COVID–19-related perturbations in psychiatric care in the largest safety-net hospital in Los Angeles74,7434414total18Cafaro et al. 2022ItalyED, inpatientMarch to May 2019March to May 2020Impact of COVID–19 on the EDs access of psychiatric patients in two of the main hospitals of Milan1023539total19Capuzzi et al. 2020ItalyEDFebruary to May 2019February to May 2020Patients receiving psychiatric consultations in two psychiatric emergency services360203F1, F2, F3, F4, F6, F720Caselli et al. 2023ItalyOutpatientJanuary 2019 to February 2020March 2020 to May 2021Psychiatric consultation before and after the COVID–19 pandemic at the psychiatric outpatient services of Varese395346F0-F421Carr et al. 2021 United Kingdom Outpatient, medication prescriptionsJanuary 2010 to February 2020March to September 2020, March to April 2020Patients registered from 1697 UK general practices, referrals to mental health services, medication prescriptions (expected versus observed)128,87199,888F3-F422Chen et al. 2020aUnited KingdomOutpatientJanuary to May 2019January to May 2020Referrals to secondary mental health care services from Cambridgeshire and Peterborough NHS Foundation Trust (CPFT)386328F0, F1, F5, F6, F823Chow et al. 2021NetherlandsOutpatient, telemedicineApril to June 2019April to June 2020Number of care contacts of patients with mental health care professionals from a large Dutch mental healthcare institute66,38769,430F1, F2, F3, F4, F5, F6, F824Chu et al. 2024CanadaInpatient, outpatient, ED, medicationJune 2018 to June 2019June 2021 to June 2022Describe and compare the characteristics of people with SUD and their use of healthcare services259,497276,459total25Clerici et al. 2020ItalyInpatientJanuary to March 2019January to March 2020Hospital admissions in seven General Hospital Psychiatric Wards695648F1, F2, F3, F626Correia et al. 2024CanadaOutpatient, inpatientJanuary to March 2019January to March 2021Incidence of mental health (MH) among perinatal people in three different COVID–19 phasesTotal population: 72,242. antenatal MH diagnoses, 2019 versus 2021: aRR = 1.32 (CI = 1.20–1.46). postpartum MH diagnoses: 2019 versus 2021: aRR = 1.16 (CI = 1.08–1.25). study not included in meta-analysis due to highly specific population.27Davies et al. 2021United KingdomInpatientMarch to August 2019March to August 2020In-patient psychiatric admissions to Kent and Medway NHS and Social Care Partnership Trust15371457F0-F828deDiegoRuiz et al. 2023SpainInpatientMarch to May 2019March to May 2020Sociodemographic and clinical profile of psychiatric patients admitted to Gregorio Marañón Hospital during lockdown194204F2-F629Der et al. 2023USAMixed (ED, inpatient)January 2016 to March 2020April 2020 to March 2021Proportion of hospital and emergency department encounters for MH/SUD diagnoses in the United States45,14110,433Total30Di Lorenzo et al. 2021aItalyOutpatient, telemedicineMarch to August 2019March to August 2020Urgent psychiatric consultations performed at the outpatient Mental health Center of Modena425488F0-F731Di Lorenzo et al. 2021bItalyED, inpatientMarch to August 2019March to August 2020Urgent psychiatric consultations in ED of two Modena General Hospitals, admissions from the ED602476F2-F432Di Valerio et al. 2024ItalyMedication dispensingJanuary to December 2019January to December 2020Changes in antidepressant drug use post-COVID–19 to understand the pandemic’s effect on mental health.341,891336,596Antidepressants33Dindar et al. 2024TurkeyInpatientMarch to September 2019March 2019 to September 2020March to September 2021March 2020 to September 2021Effect on the clinical conditions of the patients with bipolar disorder and schizophrenia spectrum disorders in a community mental health center (CMHC)6860F2, F334Engels et al. 2022GermanyInpatient, medication prescriptionJanuary to December 2019, March to May 2019January to December 2020, March to May 2020A secondary data analysis based on AOK insurance data427,811368,543F0-F835Ettman et al. 2024USAOutpatient, telemedicineNovember 2017 to March 2020March 2020 to October 2022Differences in appointment completion rates between telepsychiatry and in-person outpatient psychiatric care294,103292,163Total36Fasshauer et al. 2021aGermanyInpatientMarch to May 2019March to May 2020Number of admissions for psychiatric disorders and length of stay from 67 hospitals47753327F0-F637Fasshauer et al. 2021bGermanyInpatient20192020Inpatient admissions for psychiatric diagnoses from 13 hospitals22,25119,691F0-F938Fasshauer et al. 2022 GermanyInpatientJanuary to December 2019, April to June 2018/2019January to December 2020, April to June 2020Number of emergency admissions and length of stay from several psychiatric hospitals25,41522,469F0-F639Fellinger et al. 2023AustriaInpatientJanuary 2018 to December 2019January to December 2020Examine the association between COVID–19 lockdowns and involuntary psychiatric admissions in Austria44,63021,486Total40Flament et al. 2021BelgiumEDMay 2019May 2020Number of psychiatric visits to the ED of a university hospital5550Total41Flodin et al. 2023NorwayLatviaSwedenNetherlandsoutpatientJanuary 2015 to December 2021March to December 2020Characterize the impact of the pandemic on common mental disorders recorded prevalence in primary careTotal population: 7905 person-months. RR values were taken directly from the original studyTotal42Fuster-Casanovas et al. 2024SpainOutpatient, telemedicineJanuary 2017 to December 2022January to December 2020Analyze the approach to depressive episodes and the role of eHealth in the Catalan health care system from 2017 to 202224,00423,778F343Fstkchian et al. 2023USAMedication prescriptionNovember to December 2019March to April 2020Number of patients with OUD who received a prescription78F144Fu et al. 2024United KingdomMedication prescriptionMarch 2018 to March 2020March 2020 to July 2020Impact of pandemics on primary care before, during, and after lockdowns in England, UKTotal population: 19,356. data reported as average monthly number of prescriptionsTotal45Gajdics et al. 2023HungaryInpatientMarch 2017 to March 2020March 2020 to May 2022Impact of the COVID–19 pandemic on patients diagnosed with AUD753329F146Giménez-Palomo et al. 2024SpainEDJanuary to December 2019January to December 2020Consultation trends of adults to the Psychiatric ED to one of the main third-level hospitals of Barcelona48144007F1-F947Gómez-Ramiro et al. 2021SpainED, inpatientDecember 2019 to March 2020March to June 2020Psychiatric emergency attendances to the Hospital Clinic of Barcelona, admissions from the ED1208750F0-F948Goldschmidt et al. 2023GermanyED, inpatientMarch to May 2019March to May 2020Psychiatric emergency presentations and admissions during the first wave of COVID–19 at a Berlin psychiatric hospital894813F2, F3, F649Golubovic et al. 2022SerbiaInpatientMay to August 2019May to August 2020Adult psychiatric inpatients admitted at University Clinic Center96103F0, F2, F3, F4, F6, F750Goncalves-Pinho et al. 2020PortugalEDMarch to May 2019March to May 2020Visits to the ED of the University Hospital Center1633780F2, F3, F4, F6, F951Hamlin et al. 2022SwedenED, inpatientMarch to June 2018 and 2019March to June 2020Changes in the rate and pattern of visits and hospital admissions for psychiatric disorders at a large Swedish hospital330290F1, F2, F3, F4, F652Hansen et al. 2024New ZealandInpatientJanuary to December 2019January to December 2020All hospitalizations in New Zealand with a primary psychiatric diagnosis before and during the pandemic27,91627,808F1-F653Hakansson et al. 2021SwedenEDJanuary to December 2019March to December 2020Number of patients seen in two emergency psychiatric facilities58165127total54Holland et al. 2021USAEDMarch to October 2019March to October 2020Changes in US ED visits for mental health conditions from more than 3500 EDs40,49240,230total55Irigoyen-Otiñano et al. 2024aSpainED, inpatient, outpatientJanuary to March 2020March to June 2020Differences in emergency psychiatric visits before and during the COVID–19 lockdown in Lleida, Spain697902F1-F556Irigoyen-Otiñano et al. 2024bSpainED, inpatientJanuary to March 2020March to June 2020Emergency care and continuity of care for patients with substance use disorders at the Hospital Universitario Santa María de Lérida206317F157Jagadheesan et al. 2021 aAustraliaInpatientMarch to September 2019March to September 2020Patients admitted to inpatients units of a large mental health network in Melbourne14871307F0, F1, F2, F3, F4, F658Jagadheesan et al. 2021 bAustraliaEDMarch to September 2019March to September 2020The rate of ED presentations at a public mental health service of the Royal Melbourne Hospital467451F2-F359Jahlan et al. 2022Saudi-ArabiaOutpatientMarch to June 2019March to June 2019Effects of COVID–19 pandemic lockdown on the utilization of mental health services in King Abdulaziz Medical City in Jeddah14169total60Jones et al. 2023USATelemedicine medication prescriptionSeptember 2018 to February 2020September 2019 to February 2021Examine the association of the Receipt of telehealth services and medications for OUD with fatal drug overdoses before and during the pandemic11,89422,635F161Jones et al. 2024AustraliaEDJanuary 2018 to March 2020March to June 2020Effect of the pandemic on mental health ED presentations by comparing observed presentation numbers to predictions from pre-pandemic data98,99514,983F2-F562Joo et al. 2022South KoreaInpatient, outpatientFebruary to August 2019February to August 2020Investigate changes in the use of psychiatric services during the early phase of the COVID–19 pandemic at the nationwide level10,792,85410,449,486F2-F463Kim et al. 2023bUSAInpatientMarch to July 2019March to July 2020Characterize and compare inpatient psychiatric admissions in West Texas before and during the initial months of the pandemic674718total64Kim et al. 2023aSouth KoreaInpatient, outpatientJanuary to December 2019January to December 2020Impact of the coronavirus disease 2019 (COVID–19) pandemic on mental health service utilization232,858196,911total65Lee et al. 2020ChinaInpatient, outpatient, telemedicineNovember 2019 to January 2020February to April 2020Psychogeriatric admissions, number of outpatient services in a major psychiatric unit in Hong Kong16321685F0, F1, F2, F3, F4, F766Lee et al. 2022KoreaEDJanuary to June 2019January to June 2020Psychiatric patients visiting 402 nationwide EDs88,52073,281F2-F367Lee et al. 2023USAOutpatientJanuary to December 2019January to December 2020Care delivery and patient characteristics in outpatient mental health clinics within an academic health system57,62961,766total68Lee et al. 2024USAOutpatientMarch to December 2019March to December 2020Mental healthcare utilization patterns among individuals with pre-existing mental disorder130,749133,272total69Leonhardt et al. 2024NorwayMixed (inpatient, outpatient)January to December 2019January to December 2020Frequency of substance-induced psychosis (SIP) during COVID–19 among individuals621545F170Li et al. 2023ChinaOutpatientJanuary to December 2019January to December 2020Effect of the COVID–19 pandemic on the use of serious mental illness (SMI)-related outpatient services in Ningbo, China235,667237,889F2-F371Lieber et al. 2024SwedenInpatient, outpatient, medication prescriptionsJanuary to December 2019January to December 2020Impact of the COVID–19 pandemic on mental health in Sweden in terms of mental health service utilization5793057,308F1-F472Lin et al. 2023USAOutpatientMarch 2019 to February 2020March 2020 to February 2021Patients enrolled in a large academic hospital’s outpatient psychiatry programs80308224total73Luo et al. 2024FranceGermanyItalyUnited KingdomSouth KoreaUSAMedication prescriptionsApril to December 2019April to December 2020Examine the changes in psychotropic drug prescribing during the pandemic among people with depressive and anxiety disorders in six countriesomitted for clarity due to multiple countriestotal74Ludwig et al. 2022GermanyMedication prescriptionJanuary to December 2019January to December 2020Verordnungen von Psychopharmaka aus dem Arzneiverordnungs-Report, Verodnungsvolumen in DDD2,069 Mrd.2,141 Mrd.total75Mangiapane et al. 2022GermanyOutpatientJanuary to May 2019January to May 2020Changes in utilization in psychiatry – data from the German Trend Report3,896,8923796335total76McAndrew et al. 2021IrelandEDMarch to May 2019March to May 2020Number of psychiatry presentations to the ED of a large academic teaching hospital176139F0-F677McDowell et al. 2021USAEDMarch to May 2019March to May 2020ED psychiatric presentation in a large tertiary care hospital561358total78McKee et al. 2021CanadaMedication prescriptionMarch to May 2019March to May 2020Long-acting injectable antipsychotics prescribing practices during the pandemic from Canadian retail pharmacies43034518total79Mehrabadi et al. 2024USAInpatientMarch to October 2019March to October 2020Influence of the COVID–19 pandemic, including public health measures, on new onset mental health diagnoses32,64732825total80Minian et al. 2021 CanadaOutpatientJanuary 2017 to March 2020March to December 2020Pandemic related changes in enrollments in a smoking cessation program (nicotine dependence)51,2759098F17.281Molina et al. 2022USAEDJanuary 2012 to December 2019January to December 2020Examine natural trends in ED during an extended period and assess whether these trends differed during COVID–19Total population: 8967 RR values were taken directly from the original studytotal82Montalbani et al. 2021ItalyED, inpatientJanuary to March 2020March to May 2020Psychiatric consultation in the ED of an Italian hospital, admissions from the ED13358F2, F3, F4, F683Moreno-Martos et al. 2024Norway SwedenInpatient, medication prescriptionJanuary 2018 to February 2020March 2020March to December 2020Impact of the early COVID–19 pandemic on mental health-related care in Norway and SwedenTotal population: 4,232,459 (Norway) 8 180 542 (Sweden) RR values were taken directly from the original studyF2-F484Mukadam et al. 2021United KingdomEDJanuary to December 2019January to December 2020Acute mental health presentations to three mental health liaison teams and two mental healthcare centers96658296total85Muştucu et al. 2023TurkeyEDMarch to September 2019March to September 2020Number and characteristics of emergency psychiatric consultations to Emergency Department of Bursa Uludağ University357367F0-F486Nejati et al. 2021CanadaInpatientJanuary to March 2020March to June 2020Admissions to an urban acute care psychiatric centre190185total87Palzes et al. 2022USAMixed (inpatient, outpatient, telemedicine)March to December 2019March to December 2020Impact of the COVID– 19 pandemic on alcohol treatment utilization from Kaiser Permanente of Northern California1560613302F188Panariello et al. 2021ItalyInpatientFebruary to April 2019February to April 2020Variation in psychiatric hospitalization rates at the “Maggiore” Hospital in Bologna8147total89Patel et al. 2021United KingdomOutpatient, telemedicineMarch 2019 to March 2020March to May 2020Clinical contacts with mental healthcare professionals (South London and Maudsley NHS Foundation Trust)216878207530total90Perozziello et al. 2023FranceInpatient, EDJanuary to December 2019January to December 2020The medium and long-term impact of the COVID–19 pandemic on the use of mental health services1358611189F1-F691Pignon et al. 2020FranceED, inpatientMarch to April 2019March to April 2020Number and characteristics of psychiatric consultations in three emergency services, admissions from the ED1224553F1, F2, F3, F4, F692Pikkel Igal et al. 2021 IsraelEDMarch to April 2018 and 2019March to April 2020Psychiatric visits to the ED in a Health Care Center1308462F1, F2, F3, F4, F693Qamruddin et al. 2022United Arab EmiratesInpatientMarch to June 2019March to June 2020Effect of the pandemic on the socio-demographic and clinical profiles of patients who were admitted to a tertiary psychiatric hospital in the UAE189337F1-F394Rachamin et al. 2023SwitzerlandInpatient, outpatient, telemedicine, medicationJanuary to December 2019January to December 2020Impact of the COVID–19 pandemic on the utilization of inpatient and outpatient mental healthcare in Switzerland84465718513022total95Romer et al. 2021DenmarkInpatientJanuary to December 2019January to December 2020Number of psychiatric admissions (records from hospitals and Emergency Medical Services)1402113749F0-F996Ramadan et al. 2022 Saudi-arabiaEDJanuary 2018 to December 2019January 2020 to March 2021Trends in mental health disorder ED visits – multi center data298705F2-F497Raventos et al. 2022 SpainOutpatientMarch 2018 to February 2020March to June 2020Incidence of anxiety and depressive disorder – primary care records in Catalonia15345027030F3-F498Rice et al. 2025USAOutpatient, telemedicine, medication prescriptionMarch 2019 to March 2020March to December 2020Mental health care delivered to rural and urban Department of Veterans Affairs patients across the COVID–19 pandemic27200292772922total99Ross et al. 2023USAinpatientOctober 2019 to February 2020March to October 2020Trends concerning admissions due to psychosis in the ED before and after the beginning of the COVID–19 pandemic90277total100Rugova et al. 2024KosovaMedication prescriptionJanuary to December 2019January to December 2020Mental health situation in Kosovo and the impact of the COVID–19 pandemic16,7per 1000 inhabitants27,7per 1000 inhabitantsantidepressants anxiolytics101Russolillo et al. 2024CanadaInpatientMarch to December 2019March to December 2020Admissions for psychiatric-related hospitalizations before and during the COVID–19 pandemic in Vancouver472467F1-F4, F6102Salamah et al. 2024United Arab EmiratesInpatientJanuary to December 2019January to December 2020Impact of COVID–19 on sociodemographic trends and diagnostic profiles of outpatient attendees at Rashid Hospital, Dubai627468F2-F4103Sanchez-Guarnido et al. 2022SpainOutpatient, telemedicineJanuary to March 2020March to May 2020Records of 270 service users of fifteen outpatient mental health services across SpainTotal104Savić et al. 2022CroatiaInpatient, outpatient, EDJanuary to December 2019January to December 2020Changes in out- and in-patient services utilization in the largest Croatian psychiatric institution1872115899Total105Seifert et al. 2021GermanyED, inpatientMarch to May 2019March to May 2020Psychiatric ED visits in an academic teaching hospital, admissions from the ED476374F1, F2, F3, F4, F6106Seo et al. 2021South KoreaOutpatientOctober to December 2019March to May 2020Mental health service use in a tertiary hospital1405312119F0, F2, F3, F4107Silva-Valencia et al. 2024Argentina AustraliaCanadaChinaNorwayPeruSingapore, USASwedenOutpatient, telemedicineJanuary 2018 to February 2020April 2020 to February 2021Primary care visit trends related to mental health conditions in Argentina, Australia, Canada, China, Norway, Peru, Singapore, Sweden, and the USAomitted for clarity due to multiple countriesTotal108Simkin et al. 2022United KingdomOutpatientMarch to July 2019March to July 2020Analyzing data on routine referrals to mental health services for older adults services of a large mental health trust1455536F0-F3109Simpson et al. 2021USAEDJanuary to December 2019January to December 2020Change in hospitalization rates among three psychiatric emergency services2301221552Total110Sobetzko et al. 2021GermanyED, inpatientMarch to May 2019March to May 2020Presentations to the ED in a hospital – single center data, admissions from the ED374387F1, F2, F3, F4, F6111Stein et al. 2020ItalyEDJanuary to May 2019January to May 2020ED visits for mental health-related conditions at a University Hospital819625Total112Sweet et al. 2022 USAOutpatient, telemedicineNovember 2019 to February 2020March 2020 to February 2021Use of tele-mental health services using a large health system database628372922338880F3-F4113Villarreal-Zegarra et al. 2023PeruOutpatientMarch 2019March 2020number of users receiving care during a given month at all Community Mental Health Centres2366020915F2, F3, F4114Visser et al. 2025NetherlandsMedication prescriptionMarch 2019 to March 2020March 2020 to March 2022Trends and dynamics of out-patient prescribing of psychotropic medications during the COVID–19 pandemic in the Netherlands4827424741021813377Total115Vukićević et al. 2025CroatiaInpatientMarch 2019 to February 2020March 2020 to March 2021Number of psychiatric hospitalizations in a tertiary hospital in South Croatia15011084F0-F7116Vukojevic et al. 2021CroatiaInpatientFebruary to November 2019February to November 2020Number of emergency psychiatric admissions – single center study34162371F0, F1, F2, F3, F6, F7117Wang et al. 2024USAEDMay to December 2019May to December 2020Emergency department (ED) utilization from 20 EDs across a large Midwest3232038711F1-F4118Warwicker et al. 2023MaltaInpatientJanuary to December 2019January to December 2020Impact of the pandemic on inpatient mental health, by reviewing the clinical parameters of all psychiatric admissions to Mount Carmel Hospital13481378F0-F7119Wettstein et al. 2022South AfricaInpatient, outpatientMarch to May 2019March to May 2020Hospital admissions and outpatient consultations from a large private sector medical insurance scheme475998473985F0-F4 120Williams et al. 2020United KingdomOutpatient, medication prescriptionMarch to May 2019March to May 2020Primary care data on common mental health problems and SSRI medication prescriptions from 47 general practices28851522Total121Wullschleger et al. 2023SwitzerlandInpatientJanuary to December 2019January to December 2020Patients admitted to the Department of Psychiatry of the Geneva University Hospital1526313533Total122Yalcin et al. 2021 TurkeyEDApril to June 2019March to May 2020Psychiatric ED visits in a mental health epicenter32012638F0-F9123Yang et al. 2022ChinaInpatientJanuary to April 2019January to April 2020Changes in hospitalization in a tertiary teaching hospital (mental and behavioral disorders)20029Total124Ying et al. 2023CanadaMedication dispensingDecember 2018 to January 2020February 2020 to March 2021changes in dispensing patterns of mental health medications in Alberta, Canada712151776301Total125Zaki et al. 2022AustraliaInpatient, medication prescriptionJanuary to December 2019January to December 2020Investigate whether COVID–19 has led to increased usage of benzodiazepines in acute psychiatric settings1681622242F1-F4, F6 benzodiazepines126Zhang et al. 2022USAOutpatient, telemedicine, medication prescriptionsMarch to May 2019March to May 2020Trends in patients treated for mental health disorders and adverse events during Pandemic-related health care transformation8918301289338Total127Zhang et al. 2023ChinaEDJanuary to December 2019January to December 2020Changes in the frequency or patients’ demographics of visiting the PED in the largest psychiatric hospital in China136241F4128Zielasek et al. 2021GermanyInpatientMarch to May 2019March to May 2020Routine data of all inpatient and day-patient admission cases in nine psychiatric hospitals of the Landschaftsverband Rheinland1406710545F1, F2, F3, F4, F6
Study observation periods
We selected 2019 as the reference year for studies comparing multiple years with 2020 to ensure consistency and enhance comparability across studies. However, studies with different comparison periods were also included. Whenever possible, we compared the same periods before and during the pandemic to minimize the influence of seasonal variations on service utilization. An overview of the observation periods for each study can be found in the Supplementary Material in Table S5. For analysis we separated studies that examined the initial phase of the pandemic outbreak in 2020 (short term), using a cut-off of 8 months, from those that investigated longer periods, such as the entire year 2020 or subsequent years (long term).
COVID-19 containment and health index
To show the country-specific degree of COVID-19 containment measures for the respective periods of the included studies, we added the COVID-19 Containment and Health Index (CCHI) [16] to Supplementary Table 2. This index “is a composite measure based on 13 policy response indicators, including school closures, workplace closures, travel bans, testing policy, contact tracing, face coverings, and vaccine policy, rescaled to a value from 0 to 100 (100 = strictest)” [16].
Quality assessment
The quality of the included studies was assessed using a modified version of the Newcastle-Ottawa Scale (NOS) for cohort studies [17]. This scale evaluates studies across three main categories—Selection, Comparability, and Outcome—comprising eight subcategories in total. A maximum of seven stars could be awarded, with a star (“☆”) indicating that the criterion was met. If a criterion was not met, it was marked with a “/” symbol (for details, see Table S1 and S2 in the Supplementary Materials).
Level of observation
To estimate the quantitative changes in service utilization during the pandemic more reliably, we categorized the studies into three groups based on the varying data foundations:
- Category A studies: Complete or nearly complete surveys of a larger region, state, or country (e.g., regional health register data, health insurance data, or healthcare data from main regional community health providers).
- Category B studies: Samples covering several departments or clinics that do not represent the main or only healthcare provider within a defined larger region or cover the complete or nearly complete population of such a region (e.g., “13 Germany-based hospitals”).
- Category C studies: Data from individual clinics or departments (e.g., “Geneva University Medical Center”).
Data analysis
In our meta-analysis, the natural logarithm of the rate ratio (ln(RR)) was used as the effect size for statistical computations. Random-effects models were employed to estimate summary effect sizes, accounting for both within-study and between-study variability. After conducting the analyses, the ln(RR) values were exponentiated to obtain the rate ratios (RR), which are presented in all figures and tables for ease of interpretation. All analyses were performed using RStudio (Version 2023.09.1) with R (Version 4.4.1). Heterogeneity was assessed using the I ^2^ statistic from Cochran’s Q and τ ^2^ calculated with the restricted maximum likelihood (REML) method. To assess publication bias, funnel plots were generated for each setting (Supplementary Figure S2a–e).
Results
Initially, 4101 records were retrieved and 655 duplicates were excluded. After title/abstract screening, 260 studies remained for full-text screening. Following the full-text screening, 122 studies from the database search were included. The interrater-agreement showed a Cohen’s Kappa of 0.74. Citation screening identified 18 additional studies, of which 6 were selected for inclusion, resulting in a total of 128 studies included in the review [13]. Figure 1 illustrates the PRISMA flow diagram, outlining the steps involved in the screening and selection process.Figure 1.PRISMA flow diagram of study selection.
Four studies [18–21] report results from multiple countries. The following countries are represented in our review: the United States [19, 21–43] with 25 studies, Italy [19, 44–57] with 15 studies, Germany [19, 58–69] with 13 studies, the United Kingdom [19, 70–78] with 10 studies, Spain [79–86] with 8 studies, Canada [21, 87–93] and Sweden [18, 20, 21, 94–97] with 7 studies each, South Korea [19, 98–101], Australia [21, 102–105] and China [21, 106–109] with 5 studies each, France [19, 110–112] with 4 studies, Croatia [113–115], Netherlands [18, 116, 117], Switzerland [118–120] and Turkey [121–123] with 3 studies each, Malta [124, 125], Portugal [126, 127] and Saudi Arabia [128, 129] with 2 studies each. Additionally, one study originated from each of the following countries: Belgium [130], Denmark [131], Ireland [132], Israel [133], Serbia [134], South Africa [135], Argentina [21], Austria [136], Hungary [137], Japan [138], Kosovo [139], Latvia [18], New Zealand [140] and Singapore [21] (Supplementary Table S3). All continents were represented. However, the majority of studies came from the European Region (86 studies), followed by 35 studies from the Americas, 18 from the Western Pacific, 4 from the Eastern Mediterranean Region, and 1 from the Africa Region (Supplementary Figure S1), according to World Health Organization (WHO) specifications [141]. According to the World Bank classification, only high-income and upper-middle-income economies were represented (Supplementary Table S4). Detailed data are provided in Table 1. Furthermore, Supplementary Table 2 presents the individual index values of the COVID-19 Containment and Health Index for each studies region and the corresponding comparison period during the COVID-19 pandemic.
Most studies included in our analysis compared periods from 2019 with similar periods during the pandemic. The length of comparison periods varied, with some studies examining only a few months, mainly during COVID-19 high-incidence or lockdown periods, while others covered an entire year. Some studies also compared non-equivalent periods within the same year (e.g., the end of 2019 to the beginning of 2020) (Supplementary Table S5). Supplementary Table 2 outlines the distribution of the studies across different settings and the respective periods during the pandemic. In some cases (e.g. 58, 59, 94, 122), it was possible to extract and analyze data from both the short-term and long-term comparison periods and data for these extended time periods.
Sixty-four studies examined inpatient services. Forty-three studies addressed ED services, and 43 studies covered outpatient services. Twenty studies focused on psychotropic medication and 16 studies on telemedicine services (Table 1).
Four studies, listed in Table 1 and Supplementary Table 2 were excluded from the meta-analysis either due to insufficient comparability [60, 91] or because the data combined multiple service settings, preventing a disaggregated analysis of individual settings [40, 142].
Supplementary Figure S7 shows the classification of studies into one of the three levels of observation categories, as described in the Methods section. We performed separate calculations for the meta-analysis, including only the most representative category A and B studies and all three categories (Supplementary Table 2). In the following, we outline results for studies that belong to level of observation categories A or B, and we report short-term (first 8 month of the pandemic) separately from long-term comparison periods. The results for category C studies are presented in Supplementary Table 2. The corresponding forest plots for category C, as well as the forest plots for the long-term observations, can be found in the Supplementary Material (Figure S8a-d).
For the initial phase of the pandemic, all settings, except for telemedicine, showed a decrease in service utilization (Supplementary Table 2). High τ ^2^ values, particularly for telemedicine (τ ^2^: 0.51), reflect substantial between-study variability. We performed detailed subgroup analyses based on ICD-10 F-diagnosis disease categories for inpatient (Figure 2), emergency department (Figure 3), and partly outpatient service (Figure 4) as a sufficient number of Category A or B studies were only found for these settings.Figure 2.Forest plots of inpatient services utilization. AFR = African Region, AMR = Americas, EUR = European Region, WPR = Western Pacific Region. Figure 3.Forest plots of emergency department service utilization. AFR = African Region, AMR = Americas, EUR = European Region, WPR = Western Pacific Region. Figure 4.Forest plots of health care service utilization. (a–c) outpatient services, (d) telemedicine cases, (e) medication prescriptions. AFR = African Region, AMR = Americas, EUR = European Region, WPR = Western Pacific Region.
Inpatient services utilization
First, we analyzed changes in inpatient service utilization. During the initial phase of the pandemic, a significant decrease in utilization was observed across all diagnosis groups (RR: 0.75, 95% CI: 0.67 to 0.85, n = 16 studies, I ^2^ = 99.6%, Tau^2^ = 0.064) (Figure 2a). The analysis of diagnostic subgroups showed significant decreases in utilization for substance-related disorders (ICD-10 F1) (RR: 0.78, 95% CI: 0.66 to 0.92, I ^2^ = 97.7), schizophrenia, schizotypal, delusional, and other non-mood psychotic disorders (ICD-10 F2) (RR: 0.85, 95% CI: 0.75 to 0.98, I ^2^ = 96.6%), mood disorders (ICD-10 F3) (RR: 0.76, 95% CI: 0.66 to 0.87, I ^2^ = 99.0%), anxiety, dissociative, stress-related, and somatoform mental disorders (ICD-10 F4) (RR:0.72, 95% CI: 0.62 to 0.84, I ^2^ = 98.4%), and personality disorders (ICD-10 F6) (RR: 0.87, 95% CI: 0.75 to 1, I ^2^ = 89.4%) (Figure 2c–g). No significant changes were observed for organic mental disorders (ICD-10 F0) (Figure 2b). For the long-term comparison period, a less pronounced but statistically significant decline in inpatient utilization was observed (RR: 0.93, 95% CI: 0.89 to 0.98, I ^2^ = 99.8%) (Supplementary Table 2).
Emergency department service utilization
Next, we examined ED utilization for mental disorders. The meta-analytic model showed a reduction of RR: 0.87 (95% CI: 0.69 to 1.10, n = 8 studies, I ^2^ = 99.7%, Tau^2^ = 0.108) across all diagnosis groups for the initial phase of the pandemic (Figure 3a). The analysis for diagnosis subgroups (ICD-10 F1, F2, F3, and F4) showed no significant change (Figure 3b–e). For the long-term comparison periods, a non-significant, slight increase in the utilization of mental health ED services was observed, with substantial heterogeneity in primary studies (RR: 1.18, 95% CI: 0.66 to 2.09) (Supplementary Table 2).
Outpatient services, telemedicine, medication
Finally, we examined changes in outpatient and telemedicine service utilization and psychotropic medication prescriptions. Due to the small number of studies, no diagnostic subgroup analyses were performed for telemedicine and medication prescriptions. During the initial phase of the pandemic, we observed a significant decrease in outpatient service utilization (RR: 0.78, 95% CI: 0.66 to 0.92, n = 15 studies, I ^2^ = 100%, Tau^2^ = 0.102) (Figure 4a). The analysis for diagnosis subgroups (ICD-10 F2 and F3) in the outpatient setting showed no significant change, whereas meta-analysis showed a significant increase in the utilization of telemedicine (RR: 7.57, 95% CI: 3.63 to 15.77, n = 4 studies, I ^2^ = 100%, Tau^2^ = 0.516) (Figure 4d) and no significant change in psychotropic medication prescriptions (RR: 0.90, CI: 0.77 to 1.05, n = 15 studies, I ^2^ = 100%, Tau^2^ = 0.129) (Figure 4e).
For the long-term comparison periods, a significant decrease in the utilization of outpatient services (RR: 0.79, 95% CI: 0.65 to 0.97, I ^2^ = 100%), and telemedicine services (RR: 18.38, 95% CI: 3.63 to 93.08, I ^2^ = 100%) was observed, whereas medication prescriptions showed no significant change (RR: 0.91, 95% CI: 0.74 to 1.11, I ^2^ = 100%).
Regional differences in service utilization
For some regions, meta-analysis of regional results were possible: For Europe inpatient psychiatric service utilization declined consistently across all ICD-10 F groups (F1 = RR: 0.78, 95% CI: 0.69 to 0.88, F2 = RR: 0.88, 95% CI: 0.80 to 0.97, F3 = RR: 0.78, 95% CI: 0.72 to 0.85, F4 = RR: 0.71, 95% CI: 0.64 to 0.78), while decreases in the Western Pacific Region were smaller and non-significant (F2 = RR: 0.86, 95% CI: 0.71 to 1.03, F3 = RR: 0.84, 95% CI: 0.66 to 1.07, F4 = RR: 0.90, 95% CI: 0.76 to 1.07). For the ED setting, Europe showed significant reductions only for organic mental disorders (F1 = RR: 0.72, 95% CI: 0.54–0.97). Studies from the Americas showed stable or slightly increased utilization (total = RR: 1.03, 95% CI: 0.87 to 1.21). Corresponding forest plots are in Supplementary Figure S3.
Discussion
This systematic review and meta-analysis of MHS utilization demonstrates significant changes during the COVID-19 pandemic compared to the pre-pandemic period. The most prominent change is a significant decrease in inpatient service utilization during the first month of the pandemic. In contrast, reductions in ED, outpatient services, and psychotropic medication utilization were less pronounced. The analysis of ED studies showed the importance of relying on representative samples, as the Category C studies showed significant reductions, whereas the analysis of the more representative Category A and B studies showed (for all diagnostic groups together) no significant change, even for the initial month of the pandemic. For the long-term observations, reductions in MHS service utilization were smaller, which might reflect an adaptation of patients and systems seeking to balance infection protection with the need for services. The introduction of telemedicine and modifications to clinical practices likely contributed to this recovery. Overall, the reductions in the initial period seemed to be more pronounced in Europe, as meta-analyses of studies from other world regions, like the Western Pacific Region or the Americas, did not indicate significant changes.
For the initial period of the pandemic, the analyses showed differential effects depending on subgroups of mental disorders (according to ICD-10). Significant reductions in inpatient care were noted for substance use disorders (ICD-10 F1), affective disorders (F3), neurotic, stress-related, and somatoform disorders (F4), and personality disorders (F6), whereas for organic mental disorders (F0) and schizophrenia, schizotypal, and delusional disorders (F2), no significant reductions were observed. Regarding ED utilization, a reduction reaching statistical significance was only observed for substance use disorders (F1).
There are no indications that the prevalence or treatment needs for substance use disorders (ICD-10 F1), affective disorders (ICD-10 F3), and neurotic, stress-related, and somatoform disorders (ICD-10 F4) declined during the pandemic. It is more likely that disruptions in service availability and access, as well as patients’ fears of infection or general policy measures like curfews and so forth led to decrease in inpatient treatment utilization for these patients. As well, it is not known in which regions and to what degree existing flexible healthcare models like assertive community treatment or telemedicine were able to compensate for reduce inpatient or outpatient in-person offerings. In that sense, some mental healthcare systems might have been better equipped to deal with the challenges of the pandemic. However, to our knowledge, no large-scale systematic studies have investigated the effects of the reductions on treatment quality, treatment outcomes, or infection prevention. Therefore, these reductions and the potential harm from delayed treatment cannot be assessed. This underscores the need for more systematic monitoring of mental health system utilization and quality at national and international levels.
In this context, the regional and economic imbalance of the included studies is notable: most were from Europe, but even within the European Union, studies were from only 12 of the 27 member states. 27 countries were classified as high-income economies and seven as upper-middle-income economies. No countries from lower-middle-income or low-income economies were represented in our review. Within Europe, this calls for a harmonized mental health system utilization and quality indicators to become an essential part of the planned European Health Data Space, which would enable more comparable European health policies and their effects. This would allow us to learn from the most successful models.
The remarkable increase in telemedicine service utilization (RR: 7.57) can be seen as an essential adaptation of mental healthcare systems. It would be desirable for these service levels to be maintained beyond the pandemic, as they could help mitigate the shortage of qualified mental healthcare professionals, especially in rural areas, and provide low-barrier, low-stigma access options. However, in this context, the evidence base for telemedicine interventions, especially for long-term treatments for severely ill patients, needs further expansion, and access barriers to digital services need to be taken into consideration [81, 143].
Our findings are consistent with previous studies during times of health crisis and longer-term disasters like the SARS outbreaks in Taiwan and Toronto, the West African Ebola outbreak or following Hurricane Katrina, that were showing significant declines in healthcare utilization for outpatient, inpatient, and emergency services. Those reductions were due to fears of infection and restrictive measures [144, 145, 146] as well as infrastructure loss and system fragmentation [147].
This review has several limitations: It focuses only on the first year of the pandemic. Trends in service utilization may have evolved in subsequent years. Continued monitoring and analysis of service usage in the following years are needed to capture the long-term effects and recovery processes in mental health care. The aforementioned geographic and economic imbalance of the included studies limits the generalizability of the findings to global contexts. Future research should aim for studies from a broader, more representative range of regions to enhance the external validity of the findings. The review was limited to studies identified in three databases and restricted to publications in three languages, thus potentially impacting the comprehensiveness of the review. Furthermore, we analyzed only shifts in utilization, but we could not take into account differential access to services, e.g., to telemedicine due to lack of access to technology or digital literacy. In general, the restriction to quantitative studies limits the interpretation, e.g., with regard to the background of changes and experiences of those affected. This review included only studies on adult MHS. It should be repeated for child and adolescent MHS utilization, as those populations seemed to be especially burdened by the pandemic.
The heterogeneity of study results was high, and care must be taken when interpreting these results. This, in comparison to the meta-analysis of randomized-controlled trials, high heterogeneity was not unexpected, as healthcare system organization (see Supplementary Table S3), regional infection protection policies (see CCHI in Supplementary Table 2), and the impact of COVID-19 varied between countries and world regions. Another contributing factor was the heterogeneity of study designs, and sample sizes, ranging from studies with millions of participants to those with as few as 100. This variability may affect the robustness and comparability of the meta-analytic findings, potentially introducing bias and reducing the reliability of the overall conclusions. Therefore, the effects should not be evaluated in terms of their absolute value, but it should be emphasized that they were observed despite the great heterogeneity in MHS organization and protection measures. Consensus on further methodological standardization for studies of healthcare utilization should be pursued [9].
Overall, our analyses suggest that the COVID-19 pandemic led to substantial shifts in mental healthcare utilization, with increased reliance on telemedicine alongside reductions in inpatient and emergency services. It remains unclear to what degree telemedicine or other flexible care interventions were able to compensate for those reduced services, especially as they can also have significant access barriers. The reductions were likely to have left specific patient populations, such as people with substance use disorders, affective disorders, or neurotic, stress-related, and somatoform disorders, underserved. To prepare MHS better for future public health challenges, better internationally comparable longitudinal mental health system utilization and quality surveillance data are needed. Such data would allow us to learn which care models are able to maintain needs-oriented, high-quality care even during disruptive crises like the COVID-19 pandemic.
Supporting information
10.1192/j.eurpsy.2025.10119.sm001Glock et al. supplementary material 1Glock et al. supplementary material
10.1192/j.eurpsy.2025.10119.sm002Glock et al. supplementary material 2Glock et al. supplementary material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO – Coronavirus disease (COVID-19) pandemic.
- 2Ahrens KF, Neumann RJ, Kollmann B, Plichta MM, Lieb K, Tüscher O, et al. Differential impact of COVID -related lockdown on mental health in Germany. World Psychiatry. 2021;20:140–1.33432755 10.1002/wps.20830 PMC 7801843 · doi ↗ · pubmed ↗
- 3Gilan D, Röthke N, Blessin M. Psychomorbidity, resilience, and exacerbating and protective factors during the SARS-Co V-2 pandemic. Dtsch Ärztebl Int. 2020. 10.3238/arztebl.2020.0625.PMC 781778433200744 · doi ↗ · pubmed ↗
- 4Kunzler AM, Röthke N, Günthner L. Mental burden and its risk and protective factors during the early phase of the SARS-Co V-2 pandemic: systematic review and meta-analyses. Glob Health. 2021;17:34.10.1186/s 12992-021-00670-y PMC 800662833781283 · doi ↗ · pubmed ↗
- 5Chevance A, Gourion D, Hoertel N. Ensuring mental health care during the SARS-Co V-2 epidemic in France: a narrative review. L’Encéphale. 2020;46:193–201.10.1016/j.encep.2020.04.005PMC 717415432370982 · doi ↗ · pubmed ↗
- 6Rojnic Kuzman M, Vahip S, Fiorillo A. Mental health services during the first wave of the COVID-19 pandemic in Europe: results from the EPA Ambassadors Survey and implications for clinical practice. Eur Psychiatry. 2021;64:e 41.34103102 10.1192/j.eurpsy.2021.2215 PMC 8314055 · doi ↗ · pubmed ↗
- 7Wiegand HF, Bröcker A-L, Fehr M. Changes and challenges in inpatient mental health care during the first two high incidence phases of the COVID-19 pandemic in Germany – results from the COVID Ψ psychiatry survey. Front Psych. 2022;13:855040.10.3389/fpsyt.2022.855040 PMC 909190635573380 · doi ↗ · pubmed ↗
- 8Duden GS, Gersdorf S, Stengler K. Global impact of the COVID-19 pandemic on mental health services: a systematic review. J Psychiatr Res. 2022;154:354–77.36055116 10.1016/j.jpsychires.2022.08.013PMC 9392550 · doi ↗ · pubmed ↗