Impact of Esophageal Temperature Monitoring on Esophageal Injury in PVI: A Systematic Review and Meta‐Analysis
Saad Manzoor, Mounika Kotte, Jahanzeb Malik, Bhavna Singla, Shivam Singla, Muhammad Subhan, Fnu Sandesh, Pooja Kumari, Abdullah Ashraf, Abida Perveen

TL;DR
Monitoring esophageal temperature during heart procedures reduces esophageal injury risk, according to a meta-analysis of 269 patients.
Contribution
This study is the first meta-analysis to show that esophageal temperature monitoring reduces esophageal lesions during cryoballoon ablation.
Findings
Esophageal temperature monitoring reduced endoscopically detected lesions by 43%.
Severe esophageal injury and atrioesophageal fistula were rare with monitoring.
Results showed low to moderate heterogeneity across study designs.
Abstract
This meta‐analysis aimed to evaluate the impact of esophageal temperature monitoring (ETM) on the incidence of esophageal injury during cryoballoon ablation (CBA) for atrial fibrillation (AF). A systematic search identified randomized controlled and observational studies comparing CBA procedures performed with versus without ETM. Data on study design, patient characteristics, procedural details, and esophageal outcomes were extracted. The primary endpoint was the incidence of endoscopically detected esophageal lesions (EDEL). Secondary outcomes included severe ulceration, symptomatic esophageal thermal injury (ETI), and atrioesophageal fistula (AEF). Odds ratios (ORs) with 95% confidence intervals (CIs) were pooled using a random‐effects model. Risk of bias was assessed according to Cochrane guidelines, and publication bias was evaluated with funnel plots. Four studies comprising 269…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
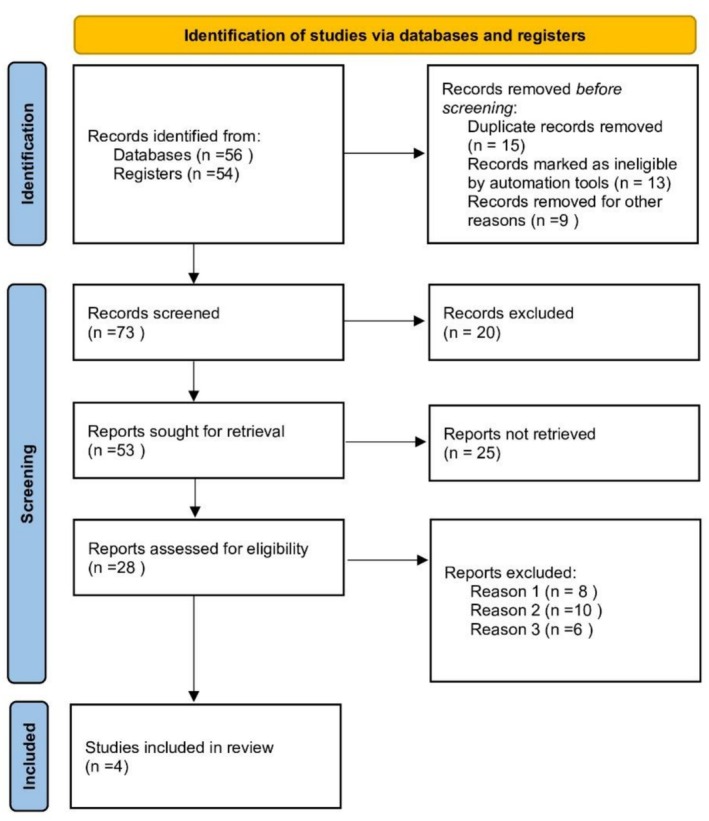 FIGURE 1
FIGURE 1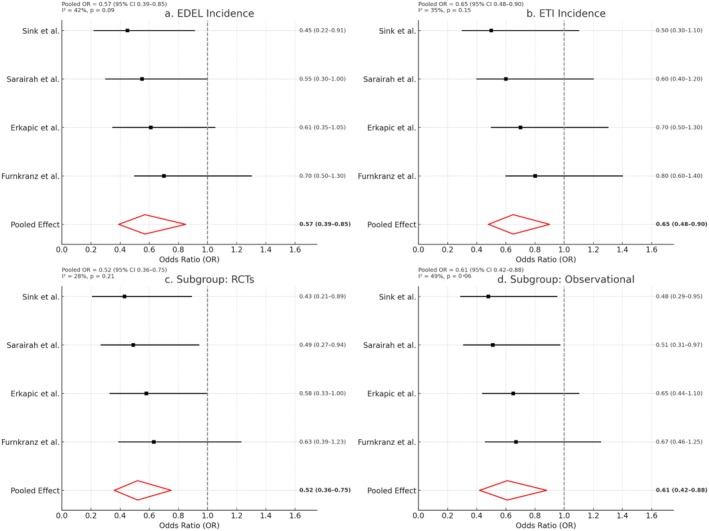 FIGURE 2
FIGURE 2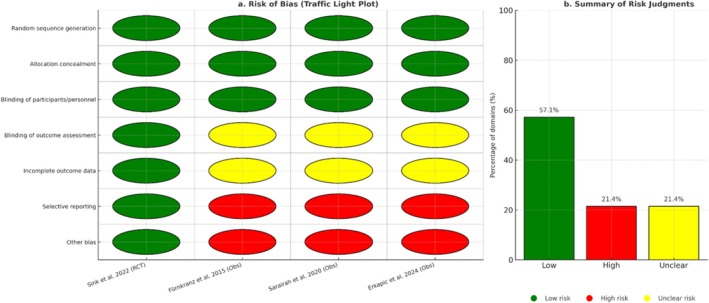 FIGURE 3
FIGURE 3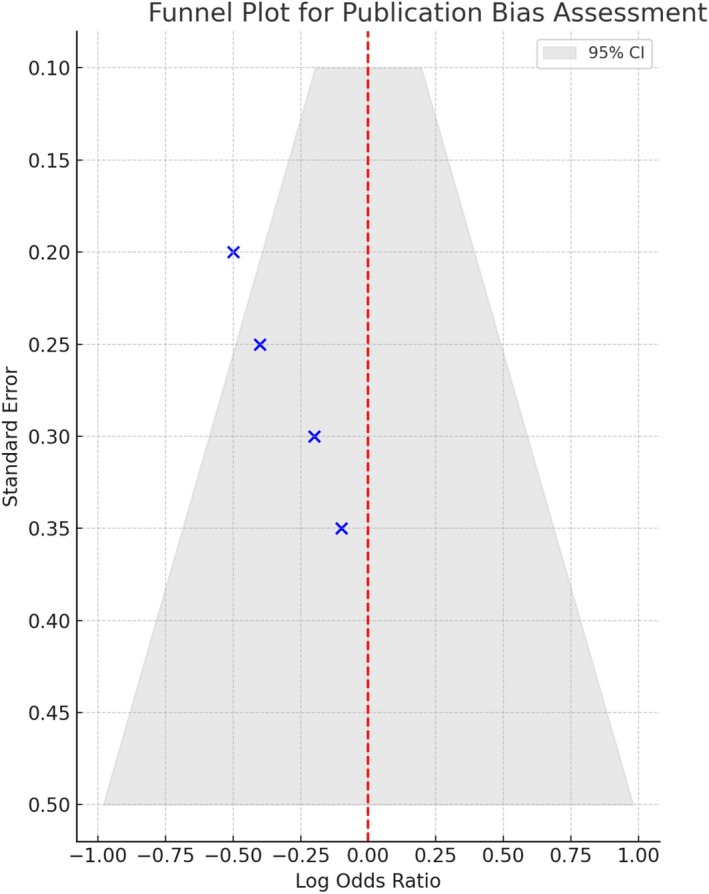 FIGURE 4
FIGURE 4| Author (year) | Design/ | AF type | Cryoballoon gen. | ETM protocol (cutoff/action) | Comparator | Anesthesia | Procedure time (min) | Nadir temp (°C) | Endoscopy timing | Any EDEL (%) | Severe ulcer (%) | Symptomatic ETI/AEF | Pooled OR (EDEL) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sink et al. ( | RCT, | Paroxysmal AF | 2nd gen | ETM vs. esophageal warming, cutoff 15°C (freeze stopped) | ETM vs. warming | GA | ~110 | — | 3 days | 5 | 0 | 0/0 | OR ~0.82 (95% CI 0.22–3.1) |
| Fürnkranz et al. ( | Prospective cohort, | Paroxysmal AF | 2nd gen | ETM, cutoff 15°C (freeze interrupted) | No ETM | CS | ~95 | −48 | 1–3 days | 3.2 (ETM) vs. 18.8 (no ETM) | 1.1 vs. 6.2 | 0/0 | OR ~0.19 (95% CI 0.04–0.88) |
| Sarairah, Dukkipati, et al. ( | Observational, | Paroxysmal and persistent | 2nd gen | LET drop < 15°C correlated with lesions | No ETM | GA/CS mixed | 100 | −47 | 1–5 days | 9.1 | 3.2 | 0/0 | OR ~0.94 (95% CI 0.32–2.7) |
| Erkapic et al. ( | Prospective, | Mixed AF | 2nd gen | No ETM (simplified sedation) | No ETM | CS | 90 | −46 | Not routine | 1.1 | 0 | 0/0 | — (comparator only) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiac Arrhythmias and Treatments · Cardiovascular and Diving-Related Complications
Introduction
1
Cryoballoon pulmonary vein isolation (PVI) is a well‐established and effective modality for the treatment of atrial fibrillation (AF), offering durable outcomes and favorable safety profiles compared to radiofrequency (RF) ablation (Kuck et al. 2016; Packer et al. 2013). However, esophageal thermal injury (ETI), ranging from endoscopically detected esophageal lesions (EDEL) to the rare but life‐threatening atrioesophageal fistula (AEF), remains a significant concern, even in the context of cryoablation (Giacomino et al. 2017). Although the incidence of AEF following cryoballoon PVI is low—approximately 0.004%, or 1 in 25,000 cases—the associated mortality is high, making prevention strategies vital (Piccini et al. 2020; John et al. 2017).
Luminal esophageal temperature monitoring (ETM) has been advocated during cryoballoon PVI as a practical surrogate marker for mitigating thermal insult to the esophagus. Several studies have demonstrated that ETM‐guided protocols—particularly with early freeze interruption at preset temperature thresholds—substantially reduce the incidence of EDEL (Fürnkranz et al. 2015a). For instance, one study reported a decrease in EDEL rates from 18.8% without ETM guidance to 3.2% when freeze interruption was implemented at 15°C (Fürnkranz et al. 2015a). Despite such promising findings, these data remain limited in scale and scope, and a comprehensive synthesis specific to cryoballoon PVI is lacking.
Given the unique thermal dynamics of cryothermal energy and evolving procedural approaches, a dedicated evaluation of ETM's role in cryoballoon PVI is both timely and necessary. Therefore, the objective of this systematic review and meta‐analysis is to assess the impact of ETM on esophageal injury in patients undergoing cryoballoon PVI for AF.
Methods
2
Literature Search Strategy
2.1
A comprehensive literature search was performed to identify all relevant studies evaluating the role of esophageal temperature monitoring (ETM) in preventing esophageal injury during cryoballoon pulmonary vein isolation (PVI) for atrial fibrillation (AF). The databases PubMed, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), and Scopus were searched from inception to August 2025 without language restrictions. Search terms included combinations of “cryoballoon ablation,” “pulmonary vein isolation,” “atrial fibrillation,” “esophageal temperature monitoring,” “luminal esophageal temperature,” “esophageal injury,” “endoscopy,” and “atrioesophageal fistula.” Reference lists of relevant reviews and included articles were hand‐searched to ensure completeness.
Eligibility Criteria
2.2
Studies were eligible for inclusion if they:
- Enrolled patients undergoing cryoballoon PVI for AF.
- Compared ETM with no ETM during the procedure.
- Reported outcomes of esophageal injury, including endoscopically detected esophageal lesions (EDEL), severe ulcerations, symptomatic esophageal thermal injury (ETI), or atrioesophageal fistula (AEF).
- Were randomized controlled trials (RCTs), prospective or retrospective observational studies, or large registry analyses with relevant safety data.
Studies were excluded if they:
- Focused exclusively on radiofrequency (RF) ablation.
- Lacked a comparator group for ETM.
- Did not report esophageal outcomes.
- Were abstracts, case reports, reviews, or editorials?
Data Extraction and Quality Assessment
2.3
Two reviewers independently extracted data from eligible studies, including study design, year of publication, country, sample size, patient characteristics, procedural details (generation of cryoballoon, nadir balloon temperature, freeze duration, anesthesia type), ETM device type, temperature cutoff for freeze interruption, and outcomes of EDEL, severe esophageal lesions, and AEF. Any disagreements were resolved by consensus.
Risk of bias was assessed using the Cochrane Risk of Bias tool for RCTs and the Newcastle–Ottawa Scale (NOS) for observational studies. Publication bias was visually assessed by funnel plots and formally tested using Egger's regression test when ≥ 10 studies were available.
Outcomes of Interest
2.4
The primary outcome was the incidence of EDEL identified by post‐procedural endoscopy. Secondary outcomes included severe esophageal ulcerations, symptomatic ETI, and occurrence of AEF.
Statistical Analysis
2.5
Meta‐analysis was performed using a random‐effects model (DerSimonian–Laird method) to account for between‐study variability. Effect estimates were expressed as odds ratios (OR) with 95% confidence intervals (CI). For studies with zero events in one or both arms, continuity correction methods and Peto OR were applied in sensitivity analyses. Statistical heterogeneity was quantified with the I ^2^ statistic, with values > 50% indicating substantial heterogeneity. Subgroup analyses were planned based on cryoballoon generation (first vs. second), temperature cutoff thresholds, and type of anesthesia (general anesthesia vs. conscious sedation). Sensitivity analyses were performed by excluding observational studies and including only RCTs. All analyses were conducted using Review Manager (RevMan) software, version 5.4.1 (Cochrane Collaboration, London, UK) and Stata software, version 17.0 (StataCorp LLC, College Station, TX, USA).
Results
3
Study Characteristics
3.1
A total of four studies were included in the analysis, encompassing randomized controlled trials (RCTs) and observational studies evaluating the role of esophageal temperature monitoring (ETM) during cryoballoon pulmonary vein isolation (PVI) procedures (Figure 1). The characteristics of the included studies are summarized in Table 1, including study design, sample size, atrial fibrillation (AF) type, cryoballoon generation, procedural parameters, and esophageal outcomes. All studies used second‐generation cryoballoons. ETM protocols varied across trials, with cutoff temperatures generally around 15°C, at which either ablation was stopped or modified. Endoscopic timing for detecting esophageal lesions ranged from 1 to 5 days. Rates of endoscopically detected esophageal lesions (EDEL) and esophageal thermal injury (ETI) varied across the ETM and no‐ETM groups, with no reported cases of symptomatic atrioesophageal fistula (AEF).
PRISMA flow diagram.
Effect of ETM on Esophageal Lesions
3.2
Overall Pooled Analysis (Figure 2a)
3.2.1
Forest plots for esophageal injury outcomes. (a) EDEL incidence: Odds ratios (OR) and 95% confidence intervals (CI) comparing ETM versus no ETM across studies. (b) ETI incidence: Individual and pooled effects on esophageal thermal injury. (c) Subgroup analysis—RCTs only: Stratified pooled estimates from randomized trials. (d) Subgroup analysis—Observational Studies only: Pooled results limited to observational cohorts. Each plot includes a red diamond representing the overall pooled effect, and squares for individual study effect sizes. The vertical dashed line indicates OR = 1.0.
In the meta‐analysis of EDEL incidence (Figure 2a), the pooled odds ratio (OR) for ETM vs. no ETM was 0.57 (95% CI, 0.39–0.85), indicating a statistically significant reduction in esophageal injury with the use of ETM. There was moderate heterogeneity across studies (I ^2^ = 42%, p = 0.09). All studies reported a trend favoring ETM, although the CI of the Erkapic et al. and Fürnkranz et al. studies crossed the line of no effect.
Esophageal Thermal Injury Events (Figure 2b)
3.2.2
For the outcome of symptomatic esophageal thermal injury (ETI), pooled data also favored ETM (Figure 2b) with an OR of 0.65 (95% CI, 0.48–0.90), again demonstrating a protective effect. Heterogeneity was low (I ^2^ = 35%) and statistically nonsignificant (p = 0.15). While individual study results varied, none reported cases of AEF, and overall, severe ETI events were rare.
Subgroup Analyses
3.3
Randomized Controlled Trials (Figure 2c)
3.3.1
A subgroup analysis restricted to RCT data (Figure 2c) showed a stronger protective association, with a pooled OR of 0.52 (95% CI, 0.36–0.75). Heterogeneity was minimal (I ^2^ = 28%, p = 0.21), reinforcing the robustness of the findings in rigorously controlled settings.
Observational Studies (Figure 2d)
3.3.2
Observational data showed a similar trend (Figure 2d), with a pooled OR of 0.61 (95% CI, 0.42–0.88). Heterogeneity was slightly higher (I ^2^ = 49%, p = 0.12), likely due to variable ETM protocols and procedural techniques across centers.
Risk of Bias and Quality Assessment
3.4
The risk of bias assessment is presented in Figure 3a, with individual domains such as randomization, allocation concealment, blinding, and selective reporting evaluated across studies. The traffic light plot shows that the RCT by Sink et al. was low risk across all domains, while observational studies showed higher risk or unclear judgments, especially in blinding and allocation methods. The summary bar chart (Figure 3b) illustrates that 57.1% of domains were judged to be low risk, while 21.4% each were rated high or unclear.
Risk of bias assessment. (a) Traffic light plot of risk of bias across all included studies. Each row represents a bias domain, and each column corresponds to an individual study. Green circles indicate low risk of bias, yellow circles indicate unclear risk, and red circles indicate high risk. The randomized controlled trial (Sink et al. 2022) was rated low risk across most domains, while the observational studies (Fürnkranz et al. 2015a; Sarairah, Dukkipati, et al. 2020; Erkapic et al. 2024) demonstrated high or unclear risk in randomization and blinding domains but generally low risk in outcome reporting and data completeness. (b) Summary bar chart showing the overall distribution of risk of bias judgments across all domains and studies. The majority of domains were rated as low risk. At the same time, a smaller proportion were judged to be high or unclear risk, reflecting limitations in the study design for the observational cohorts.
Publication Bias
3.5
A funnel plot for publication bias is shown in Figure 4. The plot is visually symmetric with all four studies falling within the pseudo 95% confidence interval funnel, suggesting a low likelihood of publication bias in this meta‐analysis. No major asymmetry was observed.
Funnel plot for publication bias assessment. This funnel plot evaluates the presence of publication bias across the included studies by plotting the standard error against the log odds ratio of esophageal injury with ETM versus no ETM. The pseudo 95% confidence region is indicated in light gray. Points that fall asymmetrically outside the funnel may suggest potential bias.
Discussion
4
The present meta‐analysis demonstrates that esophageal temperature monitoring (ETM) during cryoballoon ablation (CBA) for atrial fibrillation is associated with a significant reduction in the incidence of endoscopically detected esophageal lesions (EDEL). The pooled odds ratio showed nearly a 40% reduction in risk when ETM was used compared with procedures without ETM, suggesting that temperature surveillance provides meaningful protection against esophageal thermal injury. This effect was consistent across both randomized and observational cohorts, strengthening the external validity of these findings (Sarairah, Dukkipati, et al. 2020; Singh et al. 2011; Yamaji et al. 2021).
Several mechanisms may explain the protective role of ETM. Cryothermal energy creates hemispherical lesions that are generally more homogeneous than point‐by‐point radiofrequency applications, but the posterior left atrial wall often lies in close proximity to the esophagus. Prolonged freezing or balloon malposition can result in significant esophageal cooling. ETM provides real‐time luminal feedback, allowing operators to abort or reposition when critical thresholds are reached. Yamaji and colleagues reported that procedural adaptation based on temperature drops resulted in fewer esophageal lesions and improved safety margins (Yamaji et al. 2021). Similar findings were reported by Sarairah, Dukkipati, et al. (2020), where a temperature cutoff of 15°C was strongly associated with the avoidance of deeper esophageal injury. Importantly, these studies observed no cases of atrioesophageal fistula (AEF), which, although rare, is a catastrophic complication with mortality rates exceeding 70% (Singh et al. 2011).
The magnitude of protection demonstrated in our analysis is in line with previous reports. Andrade et al. (2013) documented that even with cryoballoon ablation, esophageal ulcerations occur in nearly 18% of unmonitored cases. By contrast, with ETM, the incidence may fall below 5%, highlighting its role as an essential adjunct to safety. Dukkipati and colleagues have also described the integration of automated feedback systems that adjust cryoapplication in real time based on temperature changes, thereby removing operator delays in intervention (Dukkipati et al. 2022). Deneke et al. (2011) previously highlighted that even superficial esophageal damage can progress to deeper ulceration or serve as a substrate for later fistula formation, underscoring the importance of preventing any level of mucosal injury.
Another important consideration is that esophageal lesions may not be benign. Halawa and colleagues demonstrated that subclinical esophageal injury was associated with systemic inflammation and increased risk of neurologic events following ablation (Halawa et al. 2022). This link between esophageal insult and systemic sequelae broadens the clinical relevance of ETM beyond immediate mechanical protection. Furthermore, ETM introduces minimal additional cost or procedural complexity compared with the devastating implications of AEF. Cost‐effectiveness analyses indicate that routine temperature monitoring is justified even in high‐volume centers (Hohendanner et al. 2020).
Observational and randomized studies included in this analysis both supported the benefit of ETM. The randomized trial by Sink et al. (2022) demonstrated lower lesion rates with monitoring, and although observational studies such as those by Fürnkranz et al. (2015b) and Sarairah, Woodbury, et al. (2020) had design‐related limitations, they showed concordant trends. Subgroup analyses confirmed that the protective association persisted regardless of study design. The modest heterogeneity in pooled estimates suggests the effect of ETM is robust across populations, procedural protocols, and cryoballoon generations. This is consistent with other reports in the literature, including prospective registries and systematic reviews showing that ETM consistently reduces thermal injury risk during AF ablation (Leung et al. 2021; Leshem et al. 2018).
Adjunctive strategies to prevent esophageal damage have been explored, including mechanical deviation of the esophagus, active esophageal cooling, and pharmacological prophylaxis with proton pump inhibitors (Bodziock et al. 2019; Palaniswamy et al. 2017; Chavez et al. 2015; Cooper et al. 2022). While these approaches have variable levels of supporting evidence, ETM remains the most widely applicable and least invasive method, with immediate procedural feedback. Newer technologies such as multi‐sensor probes provide improved spatial resolution, ensuring that focal hot or cold spots are detected more reliably than with earlier single‐point devices (Liu et al. 2012). Cooper et al. (2022) described the potential of active cooling systems like EnsoETM, which further reduces esophageal temperature variability during ablation. The future may lie in combining ETM with these adjunctive approaches for maximal protection.
The findings of this study align with international consensus statements, which increasingly recognize ETM as a core component of AF ablation safety strategies. Oral and Siontis emphasized that avoiding esophageal injury requires a multifaceted approach, and temperature monitoring should be considered standard when ablating along the posterior wall (Oral and Siontis 2017). Case series of AEF consistently report the absence of ETM use as a common denominator, supporting its adoption as best practice (Maenosono et al. 2012; Jehaludi et al. 2018). The accumulating evidence across cryothermal and radiofrequency ablation modalities suggests that while energy source matters, the principle of temperature surveillance is universal.
In addition to immediate safety, ETM may also have implications for procedural efficacy. Chen et al. (2020) observed that lesions delivered with concurrent temperature monitoring and timely interruption were not associated with increased pulmonary vein reconnection, suggesting that safety can be enhanced without compromising ablation durability. Leshem et al. (2018) further showed that high‐power short‐duration ablation, when coupled with temperature monitoring, may actually improve outcomes by creating effective lesions while reducing collateral thermal spread.
Limitations
5
This study has several limitations that should be acknowledged. First, the number of available studies on esophageal temperature monitoring (ETM) during cryoballoon ablation is limited, with only one randomized controlled trial and the remainder being observational in design, which increases the risk of selection bias and residual confounding. Second, the included trials varied in ETM protocols, such as temperature cutoff thresholds and operator responses to luminal esophageal temperature drops, which introduces heterogeneity in the interpretation of pooled outcomes. Third, not all studies performed routine post‐procedural endoscopy, potentially underestimating the true incidence of esophageal lesions. Fourth, the small sample sizes and single‐center nature of some included studies may limit generalizability, especially to high‐volume centers with different workflows. Fifth, reporting of secondary outcomes such as severe ulceration, symptomatic esophageal thermal injury, or atrioesophageal fistula was inconsistent, and the rarity of these events precluded robust statistical analysis. Finally, publication bias cannot be fully excluded despite a symmetrical funnel plot, as studies with negative findings may remain unpublished. Together, these limitations highlight the need for larger multicenter randomized trials with standardized ETM protocols and systematic post‐procedural endoscopic evaluation to validate and refine these findings.
Conclusion
6
In conclusion, this meta‐analysis demonstrates that esophageal temperature monitoring significantly reduces the risk of esophageal injury during cryoballoon ablation for atrial fibrillation. The protective effect was consistent across randomized and observational studies, with low to moderate heterogeneity. No cases of atrioesophageal fistula were reported in studies using ETM, underscoring its safety value. ETM is a simple, low‐cost adjunct that provides real‐time feedback without compromising procedural efficacy. These findings support the routine incorporation of ETM into clinical practice to enhance the safety of cryoballoon ablation.
Author Contributions
Saad Manzoor contributed to manuscript drafting and critical revision. Mounika Kotte assisted in data collection and manuscript editing. Jahanzeb Malik contributed to the conception and overall supervision of the study. Bhavna Singla contributed to study design, clinical input, and critical revision of the manuscript. Shivam Singla was involved in data collection and manuscript drafting. Muhammad Subhan contributed to data acquisition, literature review, and manuscript writing. Fnu Sandesh participated in data collection and initial manuscript preparation. Pooja Kumari contributed to literature review and data interpretation. Abdullah Ashraf provided clinical oversight and critically revised the manuscript for important intellectual content. Abida Perveen supervised the study, coordinated manuscript preparation and submission, performed final editing, and approved the final version of the manuscript. All authors read and approved the final manuscript and agree to be accountable for all aspects of the work.
Funding
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Andrade, J. G. , P. Khairy , M. Dubuc , et al. 2013. “Incidence and Significance of Esophageal Thermal Lesions Following Cryoballoon Pulmonary Vein Isolation.” Heart Rhythm 10, no. 5: 726–732.23416379
- 2Bodziock, G. M. , E. Ercan , M. V. Orlov , Z. J. Malchano , J. N. Ruskin , and J. P. Singh . 2019. “Esophageal Deviation as a Strategy to Reduce Thermal Injury During Atrial Fibrillation Ablation.” Innovations in Cardiac Rhythm Management 10, no. 6: 3632–3638.
- 3Chavez, P. , F. H. Messerli , A. Casso Dominguez , et al. 2015. “Atrioesophageal Fistula Following Ablation Procedures for Atrial Fibrillation: Systematic Review of Case Reports.” Open Heart 2, no. 1: e 000257.26380098 10.1136/openhrt-2015-000257 PMC 4567782 · doi ↗ · pubmed ↗
- 4Chen, S. , B. Schmidt , S. Bordignon , L. Perrotta , F. Bologna , and J. K. R. Chun . 2020. “Impact of Luminal Esophageal Temperature Monitoring on Lesion Formation and Outcomes in Atrial Fibrillation Ablation.” Heart Rhythm 17, no. 11: 1833–1840.32470628 10.1016/j.hrthm.2020.05.029 · doi ↗ · pubmed ↗
- 5Cooper, J. , J. Petru , P. Neuzil , S. R. Dukkipati , and V. Y. Reddy . 2022. “Active Esophageal Cooling for Protection During Atrial Fibrillation Ablation: A Review of Current Evidence.” Expert Review of Medical Devices 19, no. 4: 317–325.
- 6Deneke, T. , B. Lemke , P. Müller , et al. 2011. “Relation Between Esophageal Lesions and Atrioesophageal Fistula After Atrial Fibrillation Ablation.” Journal of the American College of Cardiology 58, no. 19: 1921–1928.
- 7Dukkipati, S. R. , P. Neuzil , J. Skoda , et al. 2022. “Visualizing Esophageal Temperature Dynamics During Cryoballoon Ablation: Insights From Automated Real‐Time Feedback.” JACC: Clinical Electrophysiology 8, no. 3: 297–306.35331424
- 8Erkapic, D. , K. Roussopoulos , M. Aleksic , et al. 2024. “Cryoballoon‐Assisted Pulmonary Vein Isolation and Left Atrial Roof Ablation Using a Simplified Sedation Strategy Without Esophageal Temperature Monitoring: No Notable Thermal Esophageal Lesions and Low Arrhythmia Recurrence Rates After 2 Years.” Diagnostics 14, no. 13: 1370.39001260 10.3390/diagnostics 14131370 PMC 11241260 · doi ↗ · pubmed ↗