Artificial intelligence in emergency department triage: perspective of human professionals
Alina Petrica, Adina Maria Marza, Claudiu Barsac, Andreea Cebzan, Ioan Dragan, Daniela Zaharie, Raluca Horhat, Diana Lungeanu

TL;DR
This study explores how healthcare and IT professionals view AI in emergency department triage, finding varied attitudes and highlighting the need for education and alignment.
Contribution
The study identifies distinct stakeholder clusters and emphasizes the role of hedonic motivation and education in AI adoption for triage.
Findings
Three clusters of professionals were identified: cautious/critical, enthusiastic/optimistic, and balanced/pragmatic.
Hedonic motivation was a key driver of enthusiasm for AI in triage.
Educational strategies are needed for both developers and healthcare professionals to support AI adoption.
Abstract
The triage process in emergency departments (EDs) is complex, and AI-based solutions have begun to target it. At this pivotal stage, the challenge lies less in designing smarter algorithms than in fostering trust and alignment among medical and technical stakeholders. We explored professional attitudes towards AI in ED triage, focusing on alignments and misalignments across backgrounds. An anonymous online cross-sectional survey was distributed through professional networks of healthcare providers and IT professionals, between May 2024 and February 2025. The questionnaire covered four areas: (a) the General Attitudes towards Artificial Intelligence Scale (GAAIS); (b) professional background and career level; (c) challenges and priorities for AI applications in triage; and (d) the AI Attitude Scale (AIAS-4). Constructs from the extended Unified Theory of Acceptance and Use of Technology…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
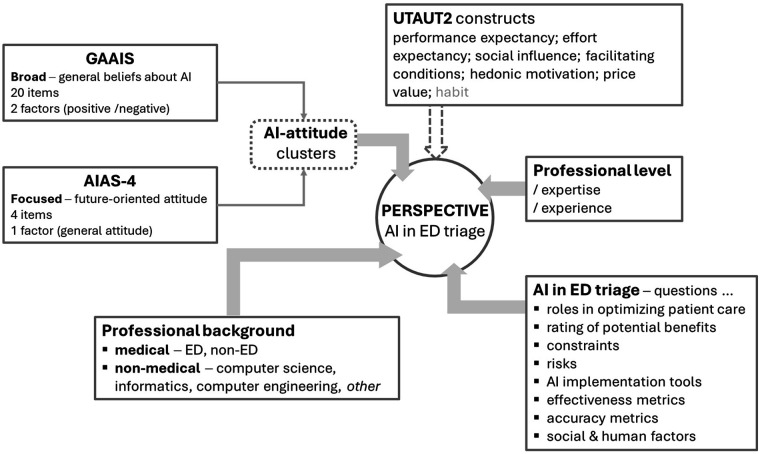 Figure 1
Figure 1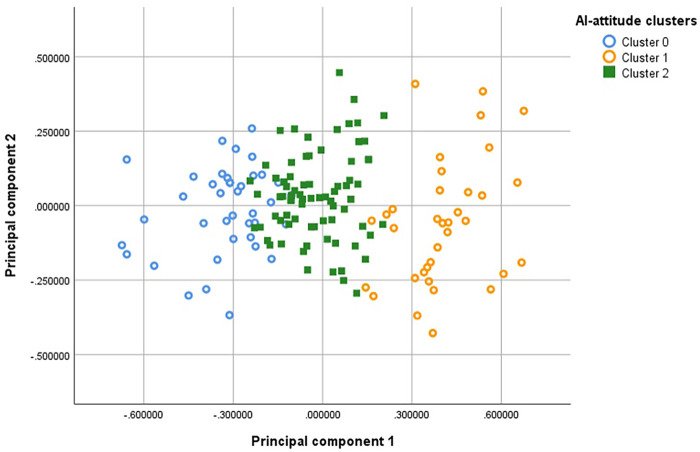 Figure 2
Figure 2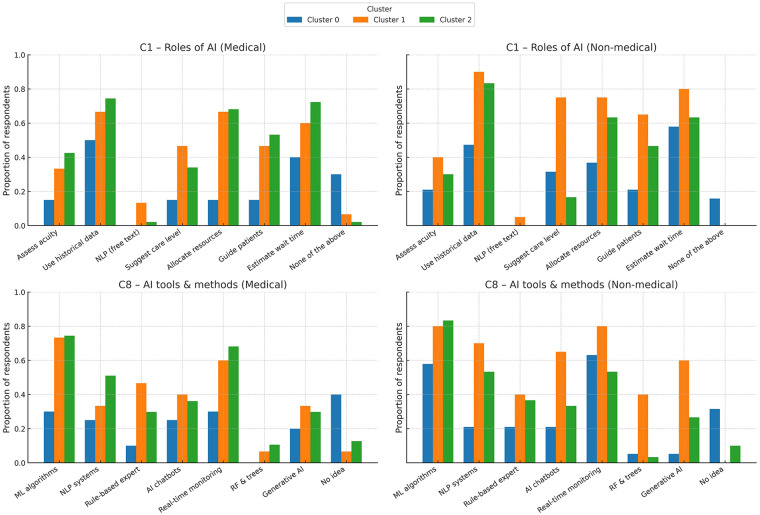 Figure 3
Figure 3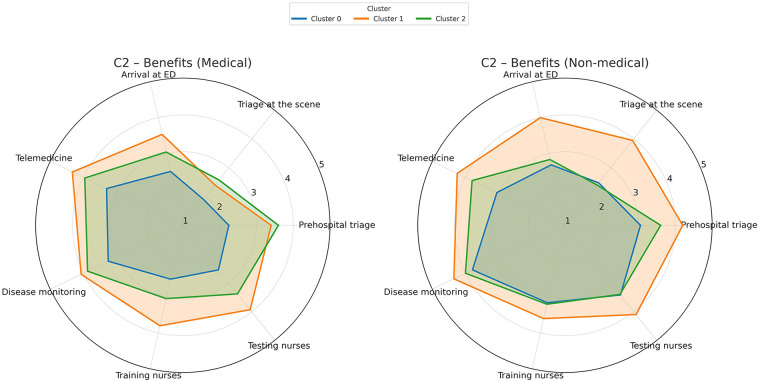 Figure 4
Figure 4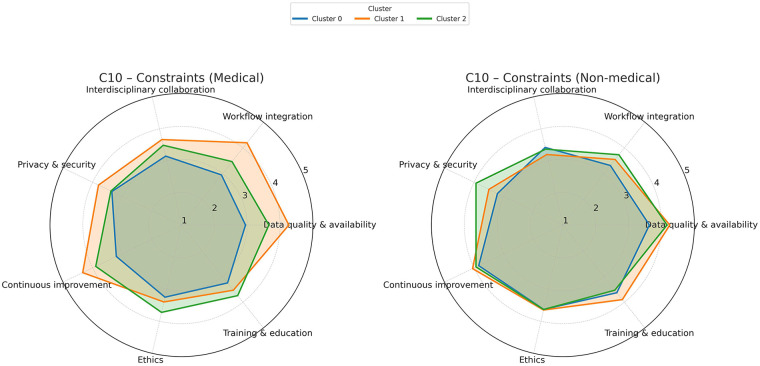 Figure 5
Figure 5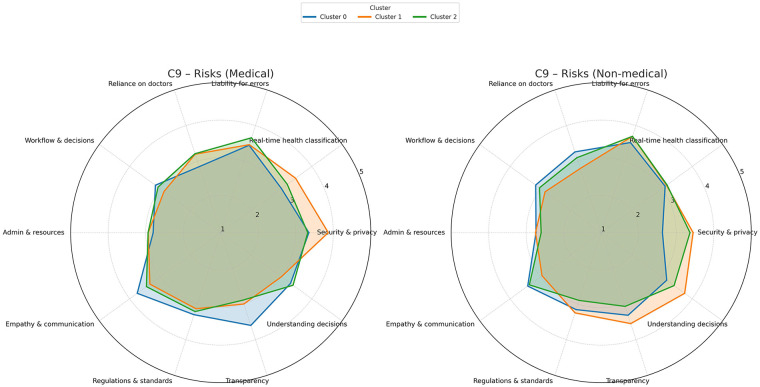 Figure 6
Figure 6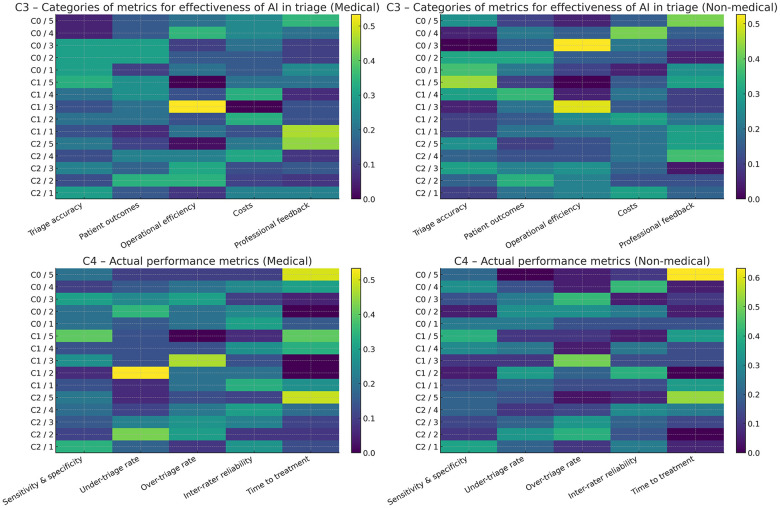 Figure 7
Figure 7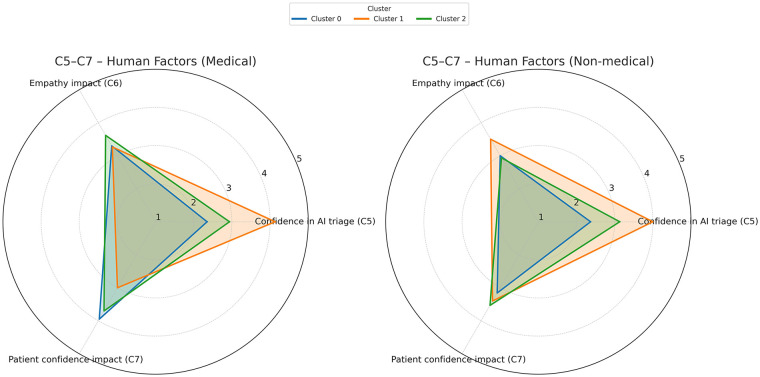 Figure 8
Figure 8| Counts (% of total) | |
|---|---|
| Gender | |
| male | 73 (48.3%) |
| female | 75 (49.7%) |
| I prefer not to tell | 3 (2%) |
| Professional background | |
| Medical other than emergency medicine | 58 (38.4%) |
| Emergency medicine | 24 (15.9%) |
| Informatics | 19 (12.2%) |
| Mathematics | ‒ |
| Computer engineering | 17 (11.3%) |
| Software engineering | 23 (15.2%) |
| Other not in the above | 10 (6.6%) |
| Level of education & profession | |
| Ongoing undergraduate studies (1) | 61 (40.4%) |
| Graduate or junior professional (2) | 44 (29.1%) |
| Senior professional (3) | 46 (30.5%) |
|
| Level of education & profession | |||
|---|---|---|---|---|
| 1—undergraduate | 2—junior graduate | 3—senior | ||
| Counts | Counts | Counts | ||
| Gender | ||||
| male | 73 | 16 (21.9%) | 28 (38.4%) | 29 (39.7%) |
| female | 75 | 45 (60%) | 15 (20%) | 15 (20%) |
| I prefer not to tell | 3 | 0 | 1 (33.3%) | 2 (66.7%) |
| Medical background | ||||
| med ED | 24 | 3 (12.5%) | 11 (45.8%) | 10 (41.7%) |
| med non-ED | 58 | 47 (81%) | 6 (10.3%) | 5 (8.6%) |
| Technical background | ||||
| tech IT | 59 | 7 (11.9%) | 24 (40.7%) | 28 (47.5%) |
| tech non-IT | 9 | 3 (33.3%) | 3 (33.3%) | 3 (33.3%) |
| Scale | No of items | Cronbach's alpha | ICC (95% CI) |
|---|---|---|---|
| GAAIS complete | 20 | 0.564 | 0.061 (0.040–0.088) |
| GAAIS positive | 12 | 0.763 | 0.212 (0.165–0.269) |
| GAAIS negative | 8 | 0.540 | 0.128 (0.083–0.184) |
| AIAS-4 | 4 | 0.922 | 0.747 (0.69–0.798) |
| AI-attitude cluster | |||
|---|---|---|---|
| 0—cautious | 1—enthusiastic | 2—balanced | |
| Attitude scores (qualitative) | |||
| AIAS-4 | low | high | moderate-high |
| GAAIS-positive | low | moderate-high | moderate-low |
| GAAIS-negative | moderate-high | moderate-low | moderate |
| Normalized attitude scores | Mean ± | Mean ± | Mean ± |
| AIAS-4 | 0.38 ± 0.15 | 0.91 ± 0.1 | 0.73 ± 0.11 |
| GAAIS-positive | 0.22 ± 0.01 | 0.7 ± 0.13 | 0.29 ± 0.13 |
| GAAIS-negative | 0.67 ± 0.15 | 0.48 ± 0.22 | 0.6 ± 0.16 |
| Background | Counts | Counts | Counts |
| medical | 20 (51.3%) | 15 (42.9%) | 47 (61%) |
| non-medical | 19 (48.7%) | 20 (57.1%) | 30 (39%) |
| Level of career and experience | Counts | Counts | Counts |
| 1 (ongoing undergraduate studies) | 13 (33.3%) | 14 (40%) | 34 (44.2%) |
| 2 (early career) | 12 (30.8%) | 7 (20%) | 25 (32.5%) |
| 3 (senior professional) | 14 (35.9%) | 14 (40%) | 18 (23.4%) |
| Insight summary | |||
| Dominant background | Balanced | Technical | Medical |
| Experience skew | Med students | Junior & senior | Mixed |
| General AI view | Critical, cautious | Positive, confident | Moderate, thoughtful |
| UTAUT2 constructs ( | Definition | Mapped items |
|---|---|---|
| Performance expectancy | Belief that using AI will provide benefits (e.g., job performance, outcomes) | GAAIS2, GAAIS5, GAAIS11, GAAIS14, GAAIS17, GAAIS18, AIAS1, AIAS2, AIAS3 |
| Effort expectancy | Ease of use, how effortless using AI feels | Could be implied by AIAS3—not directly measured; was not included in further analysis |
| Social influence | Perceived social pressure to use or trust AI | GAAIS3, GAAIS6, GAAIS10, GAAIS19, C6, C7 |
| Facilitating conditions | Availability of support, resources, and infrastructure | Items in C10 group (constraints required to ensure effective use of AI in the triage process) |
| Hedonic motivation | Fun/enjoyment associated with using the technology | GAAIS12, AIAS4 |
| Price value | Cost-benefit perception | C3m4aiCosts, GAAIS2, GAAIS11 |
| Habit | Behavioral tendency from past use | Could be AIAS3 (intention to use AI in the future) but no past use was captured in this study; was not included in further analysis |
| Cluster 0 (blue) | Cluster 1 (orange) | Cluster 3 (green) | |
|---|---|---|---|
| UTAUT2 constructs ( | Mean ± | Mean ± | Mean ± |
| Performance expectancy | 1.71 ± 0.19 | 2.02 ± 0.18 | 1.86 ± 0.18 |
| Social influence | 3.36 ± 1.09 | 3.31 ± 0.95 | 3.49 ± 0.85 |
| Facilitating conditions | 3.34 ± 0.8 | 3.8 ± 0.95 | 3.68 ± 0.8 |
| Hedonic motivation | 3.41 ± 1 | 6.86 ± 0.97 | 5.07 ± 1.08 |
| Price value | 3.38 ± 1.27 | 2.94 ± 1.41 | 3.05 ± 1.51 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsArtificial Intelligence in Healthcare and Education · Simulation-Based Education in Healthcare · AI in Service Interactions
Introduction
1
Artificial intelligence (AI) is increasingly present in society and it has also been successfully leveraged to improve medical decision making (1). While many healthcare professionals welcome AI-based solutions aimed at improving clinical work, others are more cautious, even skeptical, about its widespread use in daily clinical practice (2–6).
Emergency department (ED) triage is a complex task and a crucial decision point in emergency medicine. Its overcrowding is a growing global challenge, fueled by increased admission delays and patient influx, leading to prolonged ED length of stay (ED-LOS), treatment delays, decreased patient satisfaction, and poor outcomes. Validated triage systems, such as the Emergency Severity Index (ESI), the Canadian Triage and Acuity Scale (CTAS) or the Manchester Triage Scale (MTS), are not only administrative: they have demonstrated strong predictive value for admission, resource utilization, and mortality (7–9).
Nevertheless, there is room for improvement and AI-based solutions have already targeted emergency triage (8, 10–20); the literature emphasizes existing or future benefits in disease detection and prediction (regarding chief complaint, level of emergency, or clinical outcome), actual triage practice (e.g., improving AI-assisted ED triage, e-triage, or home-based patient triage), and human autonomy (e.g., disease tracking, activity detection, and mobile health) (12, 14, 17, 18, 21–25). Triage time in particular, defined as the time between ED check-in and triage code assignment, is frequently prolonged during peak hours, when patient volume increases dramatically and triage nurses may inadvertently overlook the most urgent cases; AI-powered solutions have been shown to be beneficial (14, 17–20). Despite these reported successes, some authors have expressed concerns about issues such as AI applications trained for single tasks, thus performing poorly in complex situations, i.e., better than lay individuals, rather than healthcare providers; such issues involve ethical and liability concerns, so these authors recommend using the AI-driven applications only in conjunction with human professionals who are expected to assume responsibility (10, 11, 13, 22, 24). At the same time, healthcare prompt engineering is developing (22, 23, 25), and promising high-performance AI-driven systems are integrating medical records, multimodal imaging, and medical literature (3, 4, 26).
However, AI in ED triage is not just a new tool, and its applications are still underexplored beyond the performance of algorithms. The adoption of AI-supported triage could mark a turning point, forcing the ED professionals to reexamine their positions, moving from being sole clinical decision-makers to roles such as team leaders collaborating with digital tools. At this pivotal stage of medical AI, many acknowledge that the real challenge is not developing the smartest algorithm, but cultivating the right mindset, trust, and cultural environment for AI to enhance—rather than degrade—the art of emergency care (2, 10, 12, 27).
While AI-based solutions in healthcare and medical decision-making are developed by computer scientists or other technical experts, medical professionals play an important role as consumers, facilitators, and even developers (i.e., as leaders participating in the development of digital tools) (15, 28–32). The overlapping in visions and expectations of these stakeholders has received little attention, even though it could be crucial to the success of the AI-driven solutions and their subsequent implementation.
We conducted an anonymous cross-sectional survey of medical and technical professionals to gather their perspectives on AI in ED triage. Our investigation aimed to explore: (a) the opinions and attitudes of professionals with various roles (i.e., consumers, facilitators, developers) towards AI in ED triage; (b) the (mis-)alignments in perspectives among these professionals; and (c) potential common paths for development in AI tools and AI-competent human resources, namely identifying priorities in professionals' perspective.
Materials and methods
2
Study design, participants and data collection
2.1
An anonymous online cross-sectional survey (implemented by Google Forms) was distributed via professional networks and specifically targeted relevant respondents: healthcare providers (medical doctors and nurses), advanced medical students (after their fourth year course of emergency medicine), computer engineers, computer scientists, programmers, advanced students in computer science and computer engineering. Snowball sampling approach was employed: potential respondents in Romania were targeted and invited to further recruit other fellow professionals (regardless of their country, nationality, or place of residence), rather than acquaintances from the general population. This type of non-probability sampling was deemed acceptable given the survey's objectives, which focused on exploratory investigations rather than hypothesis testing; therefore, no prior sample size calculation was performed.
The questionnaire was administered in English, as a universal professional language, so there was no need to translate emergent AI terminology and no language barriers in sampling. Data collection began only after participants confirmed informed consent through a mandatory initial item.
The study was conducted in accordance with the Declaration of Helsinki. Ethics Committee approval was waived due to the anonymous and professionally targeted nature of the questionnaire.
A panel of experienced professionals in emergency medicine and computer science designed the survey questionnaire based on the research objectives, related reviews and expert opinion articles (2, 5, 8–12, 14, 20), and their own professional expertise. A Delphi technique was applied to reach expert consensus and to determine: (i) the main contributors to the perspective on AI in ED triage; (ii) the relevant topics, and metrics to assess or gauge in order to achieve the objectives (i.e., identify alignments or misalignments in perspectives).
The questionnaire comprised four areas: (a) the General Attitudes towards Artificial Intelligence Scale (GAAIS); (b) information on professional background, and education/ profession level (three levels, i.e., undergraduate, junior graduate, and senior professional); (c) questions on challenges and priorities for future AI applications in the triage process; and (d) the AI Attitude Scale (AIAS-4). Both AI-related attitude scales had been previously validated and published (33–36). The face validity of the triage-specific questions (i.e., their relevance to this project) was established through the aforementioned Delphi technique during their development; no prior formal validation was performed for these items. All questions were mandatory. To compensate for possible common method bias (37), AI-related scales were included at the beginning and end of the questionnaire, with the sections of factual questions and ED triage questions between them. In addition, related topics were addressed in non-adjacent questions, and different question formats were alternated (such as, checkboxes, linear scales, and multiple choice grids).
The General Attitudes towards Artificial Intelligence Scale (GAAIS) comprises 20 items measured on a 5-point Likert scale, considering two factors: positive (12 items) and negative (8 items) components (33, 34). It has a broad scope, assessing general beliefs about AI with psychological references, including positive/ negative perceptions, risk/ opportunity evaluations, and emotional responses.
The AI Attitude Scale (AIAS-4) consists of four items measured on a 10-point proportional scale, considering a single factor (35, 36). It focuses more specifically on future-oriented attitudes towards AI and complements the GAAIS.
The triage-specific questions employed the following measurement tools: (a) 5-point Likert scales; (b) ranking scales imposing a 5-point hierarchy in the items provided; (c) checkboxes; (d) open-ended questions for free-text comments. This report presents the analysis of the quantitative data collected using the questionnaire.
To enable comparisons of the perspectives and attitudes identified in this investigation with studies conducted using various research approaches, the constructs of the extended Unified Theory of Acceptance and Use of Technology (UTAUT2)—namely, performance expectancy, effort expectancy, social influence, facilitating conditions, hedonic motivation, and price value (38, 39)—were also applied to interpret the findings of this project. UTAUT2 is based on the paradigm of technology acceptance and incorporates previous theories; its reliability has been validated (40, 41). UTAUT2 is widely used in studies on acceptance of, or attitudes towards, technologies such as digital health, telemedicine, web-based technology, or blockchain technology (41, 42).
Figure 1 presents a schematic overview of the factors shaping professionals' perspectives, as targeted in our survey. The full questionnaire of this study is openly provided on figshare with the curated data file https://doi.org/10.6084/m9.figshare.30847343.
Study diagram with the factors shaping professionals’ perspective on AI in ED triage. AIAS-4, 4-item AI attitude scale; ED, emergency department; GAAIS, general attitudes towards artificial intelligence scale; UTAUT2, extended unified theory of acceptance and use of technology.
Data analysis
2.2
Reliability of the scale measurements was assessed using Cronbach's alpha, calculated for each scale and subscale. Values above 0.7 were interpreted as indicating moderate internal consistency. The intraclass correlation coefficient (ICC) with a 95% confidence interval (CI) was also computed to evaluate measurement reproducibility, with values greater than 0.5 considered evidence of moderate to good reproducibility.
Data analysis followed an exploratory approach without formal statistical hypotheses. Descriptive statistics included observed frequency counts and percentages for categorical variables, and means with standard deviations (SD) for numerical variables, regardless of distribution. Data visualization employed column diagrams, heatmaps, and radar plots with aggregated metrics.
To examine differences in professional attitudes towards AI use in ED triage, respondents were grouped into clusters based on the three attitude-related subscales: GAAIS-positive, GAAIS-negative (reverse-scored items were inverted to align directionality), and AIAS-4. This approach aimed to identify distinct perspectives and further explore respondents' perspective in relationship with their backgrounds, experience, and ED triage–related answers (i.e., opinions or priorities). All three scorings were rescaled to a 0–1 range using min–max normalization, then KMeans clustering was performed using these normalized scorings. The silhouette score (43) was used to evaluate clustering quality. Clusters were visualized using principal components analysis (PCA), and subsequently applied as a grouping variable in downstream analyses regarding ED triage, including: preferences for AI tools; perceived risks, constraints, and benefits; priorities in evaluation metrics; and alignment with UTAUT2 constructs.
Data analysis was performed with the statistical software IBM SPSS v. 26 and R v. 4.4.3 packages.
Declaration of generative AI and AI-assisted technologies
2.3
In the research process, ChatGPT-5 from Open AI was used as research assistant to analyze the data. Authors checked the generated R code and all results, and they assume full responsibility and accountability for the contents of the work.
ChatGPT-5 was also used to improve readability and language of the work. The technology was used with human oversight and control, and all work was reviewed and edited carefully.
Results
3
A total of 151 professionals answered the questionnaire between May 2024 and February 2025. Tables 1, 2 present the general characteristics of the respondents and their characteristics in the three professional groups, respectively. There is an apparent imbalance: many advanced medical students responded to the call (hence the high percentage of undergraduate respondents with non-ED medical background), while few students with technical IT background completed the questionnaire.
Clustering based on AI-attitude
3.1
Table 3 shows low values for both Cronbach's alpha and the ICC of the GAAIS-negative factor, indicating contradictory or inconsistent opinions regarding this construct. Due to the specifics of this project which targeted two distinct classes of professionals, as opposed to a general audience as the scale's developers had done, we decided to continue with the three scales for AI-attitude: GAAIS-positive, GAAIS-negative, and AIAS-4.
KMeans clustering was applied to the standardized feature space. The final model used k = 3 clusters, and two PCA factors (which would account for 84.64% of variance). The mean silhouette scores with Euclidean distance as a dissimilarity measure were: 0.496, 0.457, and 0.344 for Clusters 0, 1, and 2, respectively. Half of the respondents belong to Cluster 2, and about a quarter to each of the Clusters 0 and 1.
Each cluster contains a mix of medical and technical professionals from all three levels of career and experience. Table 4 synthesizes these characteristics in numbers, and a qualitative summary based on the attitude scale scores (i.e., AIAS-4, GAAIS-positive, GAAIS-negative).
Figure 2 shows the three clusters with the PCA factors on the axes: Cluster 0 (blue), cautious/ critical attitudes; Cluster 1 (orange), optimistic/ enthusiastic/ supportive attitudes; Cluster 2 (green), balanced/ pragmatic attitudes.
The three AI-attitude clusters of respondents, with the two principal components on the axes.
Tasks AI could address in ED triage. AI methods and tools for implementation
3.2
Question C1 offered a list with potential tasks AI could address (i.e., roles AI applications could play) in optimizing ED triage and patient care; respondents could check as many as they considered feasible, realistic or appropriate. Similarly, question C8 requested opinions on the appropriate AI tools to implement such applications. Figure 3 synthesizes the responses, taking into account medical vs. non-medical background. Machine learning algorithms and real-time monitoring systems are the most widely supported tools across all clusters. Non-medical respondents in Cluster 1 (AI enthusiasts) endorsed almost all tools, including natural language processing systems, and generative AI. Each of them checked at least one task/ role and at least one AI method/ tool. Cluster 0 (AI skeptics)—especially medical professionals—showed limited support and the highest rates of “no ED task AI can address” and “I have NO idea of AI tools and methods”, indicating uncertainty or lack of familiarity.
Types of tasks that AI could address in the ED, along with appropriate AI tools or methods to achieve them. AI chatbots, generative AI (such as, ChatGPT, Mistral, Gemini, etc.); ML, machine learning; NLP, natural language processing; RF & Trees, random forest and decision trees.
Figure 4 synthesizes the opinions on levels of benefits AI can provide for various potential employments, such as prehospital triage, triage at the scene of the event, triage upon ED arrival, telemedicine applications, disease monitoring, training and testing the triage nurses. In Cluster 1 (enthusiasts), the contrast between medical and non-medical professionals regarding the triage itself (namely, prehospital triage, triage at the scene of the event, and ED arrival triage) is particularly notable, even enthusiastic medical practitioners being substantially more reserved compared to the technicians.
Opinions on the benefits AI could provide in areas such as prehospital triage, on-scene triage, ED arrival triage, telemedicine, disease monitoring, and training/testing of triage nurses. A 5-point Likert scale was used to score the answers.
Constraints and risks
3.3
Figure 5 summarizes opinions on the categories of constraints needed to ensure the effective use of AI in the triage process. All respondents in Cluster 1, both with a medical and a technical background, recognized the importance of imposing such constraints. In contrast, only medical professionals in Cluster 1 (the enthusiasts) emphasized constraints such as data quality, workflow integration, and continuous evaluation and improvement.
Opinions on constraints needed for effective AI use in triage. All technical professionals recognized their importance. A 5-point Likert scale was used to score the answers.
Figure 6 presents opinions on potential sources of concern and risk associated with AI use in emergency medicine. The misalignments between the clusters, and between professional groups are substantial, although all groups acknowledged some AI-related risks. Medical professionals in Cluster 1 (enthusiasts) expressed substantial concern about data security and privacy, and less concern about AI explainability (namely, the transparency in decision-making and its comprehensibility). Interestingly, medical practitioners in Cluster 2 (the pragmatics) reported few concerns apart from liability and accountability for error. In contrast to all medical professionals, the enthusiastic technicians in Cluster 1 were more concerned about AI explainability, particularly in regard to understanding the decision making.
Concerns and risks of AI in emergency medicine. A 5-point Likert scale was used to score the answers.
Metrics of effectiveness and performance
3.4
Questions C3 and C4 asked the respondents to prioritize the categories of metrics for AI-solutions' effectiveness, and performance (i.e., accuracy) relevant to AI-driven triage in emergency departments, respectively. Figure 7 summarizes their opinions in the form of heatmaps, with rank 5 being the most important. All professionals in Cluster 0 and Cluster 1 emphasized the average importance of operational metrics, while opinions on the other categories varied considerably.
Prioritization of categories and metrics relevant to AI-driven triage in emergency departments. Ranking was enforced in the questionnaire (rank 5 = most important). The clusters (from 0 to 2) and corresponding ranks (from 5 to 1) are on the vertical axes.
Opinions of the importance of accuracy indicators to assess the success of an AI-driven triage is notably dependent on the respondents' background: a higher proportion of technicians considered it as the key indicator of effectiveness, while most healthcare professionals considered it in balance with the professional feedback.
Based on the prior assumption that triage accuracy is an important category of effectiveness metrics, question C4 aimed at identifying the highest priority metric(s) of accuracy. Background-related variability was less regarding actual triage accuracy, compared to effectiveness in general: “time to treatment” and “sensitivity/specificity” were the most frequently ranked highest criteria, despite still notable variability across clusters (Figure 7).
Social and human factors
3.5
Questions C5, C6, and C7 explored respondents' confidence in AI systems for ED triage, perceptions of AI's impact on doctors' empathy towards patients, and patients' confidence in the care received during triage. Figure 8 summarizes these “confidence triangles” for medical and non-medical professionals. Among medical professionals, Cluster 1 (the enthusiasts) showed high trust in AI's triage ability and less concern about empathy impact or patients' confidence, while Cluster 2 (the pragmatics) and Cluster 0 (the cautious) showed higher concern about the impact on the patients’ confidence in the care they receive. All medical professionals expressed concern about the impact on the empathy in doctors' interaction with patients during the triage process. Non-medical professionals followed similar patterns but were generally less worried about patients' confidence than their medical counterparts.
Opinions on confidence in AI systems for ED triage, AI's impact on doctors’ empathy, and patients’ confidence during triage. A 5-point Likert scale was used to score the answers.
Integration with UTAUT2
3.6
Data collected were mapped on the UTAUT2 constructs. Table 5 shows the mapping: GAAIS and AIAS-4 items were searched first. Not all UTAUT2 constructs were retrievable from the data: for example, information regarding the effort expectancy and habit was not collected (mainly because AI is too young a field for a habit to be developed and acknowledged).
Table 6 synthesizes the descriptive statistics for these constructs within each AI-attitude cluster. They are meaningful within each construct, but not across them (i.e., they were not normalized). The hedonic motivation appears to make a substantial difference between the clusters; it might also be associated to the cost-benefit perception, which similarly has the highest values in Cluster 0.
Discussions
4
Our cross-sectional survey collected opinions and attitudes about AI in general, and AI-supported ED triage in particular. One hundred and fifty-one professionals answered the questionnaire: healthcare providers on the one hand, and technicians, mainly IT-related, on the other hand. Irrespective of their background and level of career, the respondents were grouped into three clusters, based on their general attitude towards AI: Cluster 0 (cautious or skeptical); Cluster 1 (generally enthusiastic and supportive); Cluster 2 (pragmatic and implementation-focused). Approximately half of the respondents belong to Cluster 2, of which more than 60% had medical training; more than half of this pragmatic respondents (43/77, 55.9%) were professional graduates, namely early career professionals and senior professionals from both backgrounds.
On many ED triage-related topics, the opinions appeared to be primarily related to the general AI-attitude. Such attitude-based opinions comprised: AI-based solutions would be useful in ED triage to solve problems like assessing the level of acuity and urgency of patients' condition and direct them to appropriate care level, processing historical data of patients, optimizing resource allocation, or estimating the waiting time; anticipated benefits comprise disease monitoring, telemedicine, and testing in education; time to treatment is an important metric to assess the accuracy of ED triage; most AI tools or methods could be employed in AI-driven triage. There were also topics on which opinions were rather determined by the respondents' backgrounds (i.e., medical vs. non-medical): healthcare professionals had notably higher rates of negative opinions of prospective AI-based ED triage design, implementation, and employable methods, i.e., “no ED task AI can address” and “I have no idea of AI tools and methods”, respectively; healthcare providers were more reserved regarding the AI-driven solutions for triage at the scene of an event; medical vs. non-medical respondents showed rather divergent opinions about the constraints and risks associated with AI-supported solutions, and regarding most human factors related to empathy or trust.
Our data showed substantial mis-alignment between medical and non-medical professionals regarding the classes of constraints required to ensure effective use of AI in the triage process and the potential risks associated with such AI-driven systems. Quality and availability of data in healthcare systems is acknowledged only by the enthusiastic (i.e., a quarter) healthcare professionals; this topic has already been raised as a potential issue at an organizational level (5, 15, 17, 32). Moreover, the importance of integration of such a system with existing workflow is only acknowledged by the same enthusiastic medical practitioners who answered our survey.
There was high variability in perspective of the potential risks associated with AI-driven ED triage. For example, surprisingly, the potential lack of explainability in the AI-driven triage was not seen as an issue by the medical professionals in Clusters 1 and 2 (i.e., the enthusiasts and the pragmatics), in contrast to all the technicians. This heterogeneity in perspective may be due to the emergent character of AI-supported systems in everyday clinical practice on the one hand, and to the insufficient educational support in this field on the other hand. Moreover, having AI-confident healthcare professionals is related to building AI-competent healthcare workforce able to participate in internal and external collaboration, therefore the medical education should include the objective of developing AI literacy in addition to data science literacy (3, 4, 26, 30, 44–48). Such AI-relevant learning in medical education should help healthcare professionals understand both the challenges and advantages of AI-driven solutions, understand what to expect from such systems, and bridge the “AI chasm” (2, 6), so fewer would answer “no idea” to questions regarding the AI tools or tasks in ED triage. For example, AI is paramount in natural language and free text processing, and in other related applications such as simulation-based training and testing, and metaverse in ED (1, 12, 15, 49–51), while very few respondents identified this potential in our survey.
The International Medical Informatics Association (IMIA) has updated its recommendations on education in biomedical and health informatics to include AI as a required competence (52). The European Society for Emergency Medicine (EUSEM) has a working group for digital emergency medicine (53), and an agreement with the European Federation for Medical Informatics (EFMI) to collaborate on both research and education (54). Disseminating success stories of significant improvements in triage equity through the effective implementation of AI-supported ED triage (17–20) and specialized training for AI-translators (namely, enthusiastic medical professionals from Cluster 1) would help to establish realistic expectations for interdisciplinary projects involving professionals from various backgrounds, i.e., both developers and consumers of AI-driven solutions in ED triage. Notably, interdisciplinary educational programmes on AI in healthcare already exist and aim to attract students from diverse backgrounds (55, 56). Integrating AI courses into general medical education would help develop AI-based critical thinking skills; establishing dedicated ethical frameworks and application guidelines is recognised as a crucial first step in advancing interdisciplinary approaches to deploying AI-assisted solutions in healthcare more broadly, and in ED triage in particular (26, 47, 48).
There was also heterogeneity and misalignments in the metrics for assessing effectiveness of an AI application in ED triage. As evidence-based medicine is now common practice, the integration of AI-derived evidence is also expected to intensify. Reporting protocols are already in place: TRIPOD-AI and PROBAST-AI (57).
Hedonic motivation seemed to be the optimism driving force among the enthusiasts in our survey, which confirms the investigations regarding healthcare and other fields, such as education (39, 40). It could be related to respondents' trust and familiarity with AI tools.
In summary, there is an on-going re-negotiation regarding the role AI could play in emergency triage (in relation to the means of implementation, challenges, and constraints) on the one hand, and the role of emergency physicians and their responsibilities on the other hand. While most professionals are rather moderate and balanced, there is great heterogeneity in the vision of developers and consumers, and across the levels of professional experience. AI-driven solutions in healthcare are emerging, subjective opinions are contradictory, and numerous confounding factors constitute additional obstacles to the development of a coherent vision. Multidisciplinary educational programmes on AI in healthcare are needed to develop the knowledge of bridging such existing gaps and mitigating the present contradictions. Trained enthusiasts from both medical and technical backgrounds can play an important role as AI-translators, advancing the field without compromising confidence in medical decision-making.
Limitations
4.1
The cross-sectional design and the number of respondents are the main limitations to the survey's validity, but there are underlying reasons for assuming these shortcomings. Firstly, this is a highly dynamic field; only an analysis over a limited period of time could provide a realistic picture of it, with its inherent limitations. Our investigation aims to put forward the subject to the attention of educators, policy makers, and leaders for future investigation. Secondly, the survey's distribution to the targeted English-speaking professionals was intentionally limited so we could ask domain-specific questions and contain the confounding factors.
The reliability and consistency of the GAAIS scale was low to moderate, particularly for factor GAAIS-negative; this would imply rather inconsistent negative perceptions and concerns regarding AI-related risks. They could be due to various factors, such as the heterogeneity in professional background or level of career, and individual psychological traits (which were not separately assessed in our exploratory investigation). This moderate inconsistency affected the clustering quality (i.e., the clusters were not disjoint), but the mean silhouette scores remained acceptable.
The mix of medical professionals who answered the questionnaire−ED and non-ED physicians−could also be regarded as a limitation. In addition, it was an anonymous and voluntary questionnaire, which did not allow for verification of factual information (e.g., background and level of career) or assessment of the level of professional knowledge or understanding of AI concepts. However, our investigation aimed to explore subjective opinions and attitudes, rather than synthesizing a professional report. Moreover, very often, medical practitioners need assistance of AI-based tools to work or practice beyond their strict expertise, for example when they face difficulties and need support; to use these AI-driven systems, they should both trust them and have the necessary know-how. Furthermore, the actual clusters did not show distinguishable differences in terms of professional background or career level; even with regard to attitude towards AI, although silhouette scores indicated acceptable clustering, the actual clusters were not disjoint, with a notably lower silhouette score for Cluster 2, i.e., the thoughtful, moderate half of respondents. On the one hand, the anonymous character of the questionnaire constitutes a limitation or shortcoming; on the other hand, it offers the advantage of avoiding the drawbacks associated with interviews and identifiable responses, such as selection bias, social desirability bias, and acquiescence bias.
This was an exploratory investigation and no hypotheses were tested. Our analysis provides no definite answers, but they are not actually needed in this highly dynamic developing field. UTAUT2 mapping is also merely exploratory and was not validated; therefore, no normalization was applied to compare the contribution of the UTAUT2 constructs to different opinions regarding ED triage; in addition, some GAAIS items are not related to the UTAUT2 theory, but rather to psychological components of the attitude towards AI.
Conclusions
5
AI-based solutions for optimizing ED triage should be analyzed beyond the performance of the algorithms. There is substantial misalignment in perspective of various stakeholders. This depends only to a certain extent on background and potential roles as developers or consumers. Even among professionals with similar background and expertise, hedonic motivation plays an important role in driving the interest in AI applications. Two educational directions should be followed: (a) AI courses and comprehensive programs should target the enthusiastic developers from diverse backgrounds; (b) all healthcare professionals should acquire AI literacy and become competent consumers.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maslej N Fattorini L Perrault R Gil Y Parli V Kariuki N The AI Index 2025 Annual Report. Stanford, CA: Institute for Human-Centered AI, Stanford University (2025). 10.48550/ar Xiv.2504.07139 · doi ↗
- 2Tikhomirov L Semmler C Mc Cradden M Searston R Ghassemi M Oakden-Rayner L. Medical artificial intelligence for clinicians: the lost cognitive perspective. Lancet Digit Health. (2024) 6:e 589–94. 10.1016/S 2589-7500(24)00095-539059890 · doi ↗ · pubmed ↗
- 3Liu F Zhou H Wang K Yu Y Gao Y Sun Z Meta GP: a generative foundation model integrating electronic health records and multimodal imaging for addressing unmet clinical needs. Cell Rep Med. (2025) 6:102056. 10.1016/j.xcrm.2025.10205640187356 PMC 12047458 · doi ↗ · pubmed ↗
- 4Patil R Heston TF Bhuse V. Prompt engineering in healthcare. Electronics (Basel). (2024) 13:2961. 10.3390/electronics 13152961 · doi ↗
- 5Ranjbar A Mork E Ravn J Brøgger H Myrseth P Østrem HP Managing risk and quality of AI in healthcare: are hospitals ready for implementation? Risk Manag Healthc Policy. (2024) 17:877–882. 10.2147/RMHP.S 45233738617593 PMC 11016246 · doi ↗ · pubmed ↗
- 6Seneviratne MG Shah NH Chu L. Bridging the implementation gap of machine learning in healthcare. BMJ Innov. (2020) 6:45–47. 10.1136/bmjinnov-2019-000359 · doi ↗
- 7Zachariasse JM van der Hagen V Seiger N Mackway-Jones K van Veen M Moll HA. Performance of triage systems in emergency care: a systematic review and meta-analysis. BMJ Open. (2019) 9:e 026471. 10.1136/bmjopen-2018-02647131142524 PMC 6549628 · doi ↗ · pubmed ↗
- 8Tam HL Chung SF Lou CK. A review of triage accuracy and future direction. BMC Emerg Med. (2018) 18:58. 10.1186/s 12873-018-0215-030572841 PMC 6302512 · doi ↗ · pubmed ↗