The association between adverse practice experiences and residency trainee occupational burnout
Qiaoying Wei, Hewei Xiao, Shenglin Liang, Ruida Zhang, Liuyan Lan, Qian Qin, Hao Yang

TL;DR
This study finds that adverse experiences during residency training in China are strongly linked to higher levels of occupational burnout among trainees.
Contribution
The study identifies specific adverse practice experiences most strongly associated with burnout in Chinese residency trainees.
Findings
70.48% of residency trainees in China experience occupational burnout.
Verbal abuse, personal service demands, and gender discrimination are the most common adverse practice experiences.
Physical and emotional abuse exposure is most strongly linked to increased burnout scores.
Abstract
Occupational burnout among the residency trainees in the Standardized Resident Training Program is widely prevalent in China. This study investigated the current status of Adverse Practice Experiences (APEs) among residency trainees, examines their associations with occupational burnout, and ultimately proposes targeted strategies to alleviate occupational burnout and enhance training quality. The cross-sectional study used multi-stage stratified random sampling method was used to conduct an online survey of 1,328 residency trainees from 18 residency training bases in Guangxi, China. Analysis of variance was used to explore differences in occupational burnout by exposure of APEs, and multiple linear regression was conducted to examine the association of APEs and its exposure on trainees' occupational burnout. The prevalence of occupational burnout among residency trainees was 70.48%.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1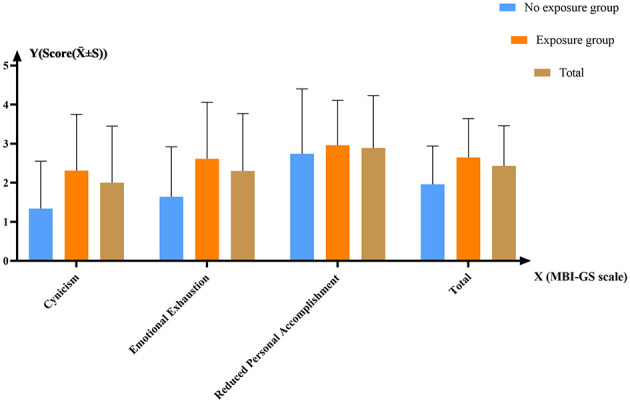 Figure 2
Figure 2|
|
|
|
|
|---|---|---|---|
|
| |||
| ≤ 25 age group | 247 (18.6) | 550 (41.42) | 797 (60.02) |
| >25 age group | 173 (13.03) | 358 (26.96) | 531 (39.98) |
|
| |||
| Female | 199 (14.98) | 573 (43.15) | 772 (58.13) |
| Male | 221 (16.64) | 335 (25.23) | 556 (41.87) |
|
| |||
| Urban | 141 (10.62) | 280 (21.08) | 421 (31.7) |
| Rural | 279 (21.01) | 628 (47.29) | 907 (68.3) |
|
| |||
| Single | 395 (29.74) | 866 (65.21) | 1,261 (94.95) |
| Married | 25 (1.88) | 42 (3.16) | 67 (5.05) |
|
| |||
| Bachelor's degree and below | 330 (24.85) | 651 (49.02) | 981 (73.87) |
| Pursuing a professional master's degree | 55 (4.14) | 174 (13.1) | 229 (17.24) |
| Master's degree and above | 35 (2.64) | 83 (6.25) | 118 (8.89) |
|
| |||
| The first year | 211 (15.89) | 368 (27.71) | 579 (43.6) |
| The second year | 120 (9.04) | 280 (21.08) | 400 (30.12) |
| The third year | 89 (6.7) | 260 (19.58) | 349 (26.28) |
|
| |||
| Yes | 104 (7.83) | 175 (13.18) | 279 (21.01) |
| No | 316 (23.8) | 733 (55.2) | 1,049 (78.99) |
|
| |||
| Never | 34 (2.56) | 19 (1.43) | 53 (3.99) |
| Once | 27 (2.03) | 31 (2.33) | 58 (4.37) |
| Occasionally | 227 (17.09) | 373 (28.09) | 600 (45.18) |
| Often | 115 (8.66) | 376 (28.31) | 491 (36.97) |
| Always | 17 (1.28) | 109 (8.21) | 126 (9.49) |
|
| |||
| Never | 137 (10.32) | 115 (8.66) | 252 (18.98) |
| Once | 32 (2.41) | 49 (3.69) | 81 (6.1) |
| Occasionally | 181 (13.63) | 423 (31.85) | 604 (45.48) |
| Often | 60 (4.52) | 249 (18.75) | 309 (23.27) |
| Always | 10 (0.75) | 72 (5.42) | 82 (6.17) |
|
| |||
| Never | 115 (8.66) | 74 (5.57) | 189 (14.23) |
| Once | 74 (5.57) | 94 (7.08) | 168 (12.65) |
| Occasionally | 224 (16.87) | 650 (48.95) | 874 (65.81) |
| Often | 6 (0.45) | 85 (6.4) | 91 (6.85) |
| Always | 1 (0.08) | 5 (0.38) | 6 (0.45) |
| Total | 420 (31.63) | 908 (68.37) | 1,328 (100) |
|
|
|
| |||
|---|---|---|---|---|---|
|
|
|
|
| ||
| Gender discrimination | 702 (52.86) | 626 (47.14) | 296 (22.29) | 224 (16.87) | 106 (7.98) |
| Racial/Ethnic discrimination | 1,013 (76.28) | 315 (23.72) | 219 (16.49) | 70 (5.27) | 26 (1.96) |
| Physical abuse | 953 (71.76) | 375 (28.24) | 269 (20.26) | 78 (5.87) | 28 (2.11) |
| Verbal abuse | 644 (48.49) | 684 (51.51) | 359 (27.03) | 237 (17.85) | 88 (6.63) |
| Emotional abuse | 786 (59.19) | 542 (40.81) | 336 (25.3) | 151 (11.37) | 55 (4.14) |
| Required to perform personal services | 674 (50.75) | 654 (49.25) | 401 (30.2) | 189 (14.23) | 64 (4.82) |
| Sexual harassment | 1,102 (82.98) | 226 (17.02) | 175 (13.18) | 33 (2.48) | 18 (1.36) |
| Pregnancy/Childcare-related discrimination | 1,134 (85.39) | 194 (14.61) | 140 (10.54) | 34 (2.56) | 20 (1.51) |
|
|
|
|
|
| |||
|---|---|---|---|---|---|---|---|
|
|
|
|
| ||||
| Gender discrimination | 2.13 ± 1.03 | 2.71 ± 1.42 | 2.57 ± 0.92 | 2.87 ± 0.92 | 3.08 ± 0.99 | 55.082 | < 0.001 |
| Racial/Ethnic discrimination | 2.29 ± 1.04 | 3.22 ± 1.11 | 2.78 ± 0.85 | 3.11 ± 0.85 | 3.25 ± 0.78 | 32.090 | < 0.001 |
| Physical abuse | 2.23 ± 1.02 | 3.22 ± 1.09 | 2.82 ± 0.87 | 3.16 ± 0.87 | 3.36 ± 0.99 | 49.377 | < 0.001 |
| Verbal abuse | 2.10 ± 1.01 | 3.04 ± 1.11 | 2.51 ± 0.93 | 2.85 ± 0.93 | 3.36 ± 0.97 | 67.96 | < 0.001 |
| Emotional abuse | 2.12 ± 1.00 | 3.12 ± 1.07 | 2.71 ± 0.87 | 3.07 ± 0.87 | 3.42 ± 0.98 | 79.809 | < 0.001 |
| Required to perform personal services | 2.09 ± 1.00 | 3.01 ± 1.12 | 2.57 ± 0.92 | 3.01 ± 0.92 | 3.37 ± 0.96 | 74.317 | < 0.001 |
| Sexual harassment | 2.33 ± 1.05 | 3.18 ± 1.12 | 2.84 ± 0.79 | 3.16 ± 0.79 | 3.03 ± 0.88 | 21.107 | < 0.001 |
| Pregnancy/Childcare-related discrimination | 2.36 ± 1.05 | 3.18 ± 1.20 | 2.73 ± 0.8 | 3.07 ± 0.8 | 3.31 ± 0.82 | 15.579 | < 0.001 |
|
|
|
|
|
|
| |
|---|---|---|---|---|---|---|
|
|
| |||||
|
| ||||||
| Once | 0.179 | 0.030 | 5.900 | < 0.001 | 0.119 | 0.238 |
| >25 | −0.050 | 0.033 | −1.500 | 0.134 | −0.116 | 0.015 |
|
| ||||||
| Male | −0.027 | 0.027 | −1.030 | 0.302 | −0.080 | 0.025 |
|
| ||||||
| Rural | 0.052 | 0.028 | 1.870 | 0.061 | −0.002 | 0.107 |
|
| ||||||
| Married | 0.029 | 0.061 | 0.480 | 0.631 | −0.091 | 0.150 |
|
| ||||||
| Pursuing a professional master's degree | 0.044 | 0.035 | 1.250 | 0.211 | −0.025 | 0.112 |
| Master's degree and above | −0.018 | 0.049 | −0.360 | 0.719 | −0.115 | 0.079 |
|
| ||||||
| The second year | 0.067 | 0.032 | 2.100 | 0.036 | 0.004 | 0.130 |
| The third year | 0.087 | 0.038 | 2.290 | 0.022 | 0.013 | 0.162 |
|
| ||||||
| Yes | 0.037 | 0.034 | 1.100 | 0.274 | −0.030 | 0.105 |
|
| ||||||
| Once | 0.218 | 0.093 | 2.350 | 0.019 | 0.036 | 0.400 |
| Occasionally | 0.252 | 0.071 | 3.570 | < 0.001 | 0.114 | 0.391 |
| Often | 0.464 | 0.074 | 6.310 | < 0.001 | 0.320 | 0.609 |
| Always | 0.632 | 0.088 | 7.190 | < 0.001 | 0.459 | 0.804 |
|
| ||||||
| Once | 0.084 | 0.063 | 1.330 | 0.183 | −0.040 | 0.207 |
| Occasionally | 0.115 | 0.038 | 3.050 | 0.002 | 0.041 | 0.189 |
| Often | 0.226 | 0.046 | 4.910 | < 0.001 | 0.135 | 0.316 |
| Always | 0.344 | 0.074 | 4.650 | < 0.001 | 0.199 | 0.489 |
|
| ||||||
| Once | 0.115 | 0.052 | 2.220 | 0.026 | 0.014 | 0.217 |
| Occasionally | 0.159 | 0.041 | 3.900 | < 0.001 | 0.079 | 0.239 |
| Often | 0.310 | 0.065 | 4.780 | < 0.001 | 0.182 | 0.437 |
| Always | 0.258 | 0.203 | 1.270 | 0.204 | −0.141 | 0.657 |
| Cons | −0.060 | 0.080 | −0.760 | 0.450 | −0.216 | 0.096 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare professionals’ stress and burnout · Diversity and Career in Medicine · Counseling Practices and Supervision
Introduction
1
The Standardized Resident Training Program (SRTP) in China has been formally established since 2014 as a kind of postgraduate education (1). This program aims to augment the professional competence and overall quality of resident physicians, aligning them with the demands of contemporary medical services (2). These professionals are required to demonstrate comprehensive mastery of medical theory and clinical practice, thereby enabling independent diagnosis and management of common diseases, prevalent conditions, and complex critical illnesses in their respective subspecialties (3). Medical students enrolled in SRTP are officially designated as residency trainees. Eligibility for residency trainee status is contingent upon fulfilling stringent admission criteria at accredited training bases, including successful completion of written examinations and structured interviews.
Trainees are required not only to fulfill rigorous clinical responsibilities but also navigate adverse events inherent to clinical environments on a daily basis. Among these challenges, Adverse Practice Experiences (APEs) are the most common negative events, including but not limited to discrimination, bullying, and harassment. Although these events have been reported internationally, research focusing on residency trainees in China has received limited attention (4–6). Empirical evidence demonstrates that APEs exert detrimental effects on trainees' career trajectory decisions (including specialty selection and residency continuation), professional identity formation, and occupational satisfaction (7–9); furthermore, these experiences may induce enduring psychological sequela.
Meanwhile, sustained exposure to clinical demands, excessive workloads, and effort-reward imbalance have been identified as key determinants of occupational burnout in residency trainees (10). Occupational burnout is defined as a state of physical and mental exhaustion, reduced enthusiasm, and disengagement resulting from prolonged exposure to high work stress and heavy workloads (11). Reports from around the world suggest that approximately one-third to one-half of physicians experience burnout (12). A cross-sectional observational study by Caesar et al. (13) found that general surgeons had the highest total burnout mean score, followed by those in emergency medicine, acute medicine, and orthopedics. In China, the prevalence of occupational burnout among residency trainees have been reported as 71.4% in Beijing, 62.2% in Shanghai, and 47.7% in Yan'an, Shaanxi Province, while the overall physicians' occupational burnout rate ranges from 66.5 to 87.8% (14–17). Additionally, one study indicated that the prevalence of occupational burnout among residents who completed the Standardized Resident Training Program was significantly lower than that of pediatric residents who had not completed the program (18).
It is worth noting that the occupational burnout experienced by residency trainees not only reflects the high-pressure clinical work environment but may also be closely related to the APEs they encounter. APEs can exacerbate occupational burnout through direct emotional distress, cumulative psychological burden, and weakened professional identity. Given that residency trainees are in a critical transitional phase from medical students to independent clinical practitioners, and considering China's unique cultural and healthcare environment, they may be more susceptible to APEs. Therefore, exploring the current situation of APEs and their impact on occupational burnout is of significant practical importance.
This study aims to reveal the current status of APEs experienced among residency trainees in Guangxi, China, and further examine how the frequency of APEs affects the level of occupational burnout among these trainees. The findings will not only provide empirical evidence to improve the quality of residency training and alleviate occupational burnout but also provide information and reference for developing targeted interventions aimed at enhancing trainees' mental health.
Methods
2
Study design and objectives
2.1
This cross-sectional study aimed to investigate the association between APEs and occupational burnout among residency trainees in Guangxi, China. The primary objectives were: (1) to describe the prevalence and types of APEs; (2) to assess the current status of occupational burnout; and (3) to quantify the association between exposure to different types and frequencies of APEs and the level of occupational burnout.
Data source and study sample
2.2
A multi-stage stratified random sampling method was employed in this study. Nine prefecture-level cities of Guangxi Zhuang Autonomous Region, including Baise, Nanning, Qinzhou, Beihai, Yulin, Liuzhou, Wuzhou, Guilin, and Guigang, were selected as primary sampling units based on a comprehensive assessment of the number of residency trainees, the economic development level, and geographical location (Figure 1). In the second stage, at least one hospital with residency training qualifications was selected from each city, totaling 18 hospitals. In the third stage, adhering to the principle of voluntariness and after obtaining informed consent, residency trainees within the sampled hospitals were randomly selected by the training grade (The first year/second/third year) and specialty (e.g., Internal Medicine, Surgery, etc.) using a stratified approach, resulting in a total sample of 1,328 trainees for the survey. After obtaining informed consent, each trainee was guided to anonymously complete the questionnaire through the “Wenjuanxing” platform (a Chinese online survey platform). Data collection occurred between January 2–15, 2025. The study was approved by the People's Hospital of Guangxi Zhuang Autonomous Region and Guangxi Academy of Medical Sciences (No: KY-KJT-2023-206).
Geographical distribution of nine sample cities and prefecture in Guangxi Zhuang Autonomous Region.
Adverse practice experiences measurements
2.3
Adverse Practice Experiences (APEs) refer to the non-medical negative events experienced by residency trainees during the SRTP. APEs include eight items: gender discrimination, racial/ethnic discrimination, physical abuse, verbal abuse, emotional abuse, required to perform personal services (e.g., being asked to do extra work-related matters of another person in a more senior position within a hierarchical medical system), sexual harassment, and pregnancy/childcare-related discrimination. These items were developed based on previous research and practical work experience (19–22). Responses are rated on a 7-point scale: “Never,” “Rarely,” “Occasionally,” “Often,” “Frequently,” “Very Frequently,” and “Every Day.” These responses indicate the frequency rather than the severity of these experiences. “Rarely” refers to a few times per year or less; “Occasionally” refers to once per month or less; “Often” refers to several times per month; “Frequently” refers to once per week; and “Very Frequently” refers to several times per week. We defined “Never” as the no exposure group, “Rarely” as the low exposure group, “Occasionally” as the moderate exposure group, and “Often,” “Frequently,” “Very Frequently,” and “Every Day” as the high exposure group.
To ensure the validity of APEs measurement, a pre-survey was conducted at Liuzhou Workers' Hospital in Guangxi Province (n = 73) prior to the formal investigation. The aim was to assess the applicability, clarity, and psychometric properties of the APEs scale among residency trainees. Exploratory Factor Analysis was performed to examine structural validity, yielding a KMO value of 0.836 and a significant Bartlett's test of sphericity (χ^2^ = 779.362, df = 28, P < 0.001), indicating good sampling adequacy. A single factor with an eigenvalue greater than 1 was extracted, accounting for 57.46% of the total variance, with factor loadings ranging from 0.576 to 0.840, suggesting a robust unidimensional structure. In terms of reliability, the scale showed excellent internal consistency (Cronbach's α = 0.866). These findings confirm that the APEs scale possesses satisfactory structural validity and reliability, supporting its use for assessing adverse practice experiences among residency trainees in this study.
Occupational burnout measurement
2.4
This study used the Maslach Burnout Inventory-General Survey (MBI-GS) scale developed by Maslach et al. (35) to assess the occupational burnout of residency trainees. The MBI-GS scale consists of 16 items and includes three dimensions: emotional exhaustion (five items), cynicism (five items), and reduced personal accomplishment (six items) (23). Chinese scholars Li Chaoping, Shi Kan, and others have adapted and revised the scale, showing that the revised version has good construct validity and internal consistency in the Chinese context (16). The MBI-GS scale is assessed using a 7-point Likert scale, with scores ranging from 0 to 6, representing the frequency of feelings (from “Never” to “Every day”). Participants self-assess based on their own experiences during the SRTP period. The Emotional Exhaustion and Cynicism dimensions are scored positively, while Reduced Personal Accomplishment is scored negatively. Based on the study by Zhang et al., occupational burnout is considered if the average score of any dimension is ≥ 3 (16). The Cronbach's α coefficient for this scale in this study was 0.863.
Statistical analysis
2.5
Data cleaning and analysis were conducted using STATA 18.0 statistical software. For quantitative data, descriptive statistics were presented using mean and standard deviation. For qualitative data, frequency (n) and proportion (%) were used for statistical description. One-way (ANOVA) and multiple linear regression analysis were used for univariate and multivariate analysis, respectively. The significance level was α = 0.05.
Results
3
Demographic characteristics
3.1
A total of 1,328 residency trainees were included in this study, with 908 in exposure group (68.37%) and 420 in no exposure group (31.63%). Of these trainees, 797 were 25 years old or younger (60.02%), 772 were female (58.13%), 907 were from rural area (68.30%). Over 70% of the trainees had a bachelor's degree or lower (Table 1).
Supplementary Table S1 presents the occupational burnout scores among trainees with different demographic characteristics. Trainees pursuing a professional master's degree exhibited the highest burnout scores. Burnout scores increased with longer duration of training. Furthermore, higher frequencies of experiencing physical fatigue due to workload, missing or delaying personal activities due to workload, and experiencing medical disputes were associated with higher burnout scores.
The exposure of APEs
3.2
The majority of residents in the study (n = 908, 68.37%) reported experiencing APEs at least once since attending SRTP. The most common APEs reported were verbal abuse (such as slander and intimidation), which accounted for 51.51%. This was followed by being required to perform personal services and gender discrimination, with proportions of 49.25 and 47.14%, respectively. 40.81% of residency trainees who experienced emotional abuse (Table 2).
Survey results of occupational burnout
3.3
Figure 2 display the average scores of occupational burnout. The score was ≥3 points in at least one dimension for 936 trainees (70.48%), indicating that there was a high prevalence of occupational burnout. The score of emotional exhaustion was 2.30 ± 1.47, the score of cynicism was 2.00 ± 1.45, and the reverse score of reduced personal accomplishment was 2.89 ± 1.34. There were 374 residents whose average scores of two dimensions were ≥3 points and 194 residents had obvious occupational burnout in all three dimensions.
The average score for occupational burnout.
One-way ANOVA results indicated that the exposure group exhibited significantly higher occupational burnout scores than the no exposure group (P < 0.001). Overall, occupational burnout scores increase with higher exposure frequency. However, for sexual harassment, the high exposure group demonstrated lower occupational burnout scores than the moderate exposure group (Table 3).
The association between APEs and occupational burnout
3.4
Table 4 display the results of the multiple linear regression model indicated that, after controlling for confounding factors (gender, hometown, marital status, etc.), residency trainees who had encountered at least one adverse practice experiences were associated with higher occupational burnout scores (β = 0.179, 95% CI [0.119, 0.238], P < 0.001). Higher frequency of experiencing physical fatigue due to workload was associated with higher occupational burnout score (from “Occasionally” to “Always,” β = 0.218–0.632, 95% CI [0.036–0.459, 0.400–0.804] P < 0.05). Similarly, frequency of missing or delaying personal activities due to workload was positively associations with occupational burnout across the “Occasionally” to “Always” range (β = 0.115–0.344, 95% CI [0.041–0.199, 0.189–0.489], P < 0.05). In contrast, frequency of experiencing medical disputes at the “Always” level showed no significant association with occupational burnout (β = 0.258, P = 0.204).
Supplementary Table S2 presents the associations between different types of APEs and occupational burnout. Overall, higher APEs exposure levels were associated with higher occupational burnout scores (P < 0.05). Results from the multiple linear regression analysis revealed that physical abuse (from “low exposure group” to “high exposure group,” β = 0.172–0.339, P < 0.001), emotional abuse (from “low exposure group” to “high exposure group,” β = 0.215–0.332, P < 0.001) and pregnancy/childcare-related discrimination (from “low exposure group” to “high exposure group,” β = 0.141–0.304, P < 0.001) were the most strongly associated with occupational burnout scores.
Discussion
4
To our knowledge, this is the first study to examine the association between varying levels of exposure to adverse practice experiences and occupational burnout among Chinese residency trainees. The findings' main clinical implications may help residency trainees avoid adverse clinical/medical events or errors, patient mortality, and medicolegal complaints/disputes.
The results of this study indicate that the prevalence of occupational burnout among residency trainees is 70.48%, which is higher than the prevalence reported in Shanghai (62.2%) and in Yan'an, Shaanxi (47.7%), but lower than that in Beijing (71.4%) (13–15). Compared to international findings, only 19.0% of resident physicians in France were found to experience occupational burnout (24). The possible reasons for this discrepancy may be that trainees in the study region bear a heavier workload, higher on-call frequency, or are exposed to more complex cases, leading to a higher prevalence of occupational burnout. On the other hand, cultural differences across countries may also play a role. In Western countries, a more open communication culture and work environment that emphasizes personal rights may help alleviate occupational burnout. Even though the same burnout measurement scale was used, there is still no consensus on the standard approach, which could explain the variations across studies. It is important to note that a high rate of occupational burnout not only affects the physical and mental health of trainees but also negatively impacts the development of their professional skills and the sustainability of their careers.
The study found that 68.37% of residency trainees (908 individuals) had experienced at least one APE. Specifically, the most common APE was verbal abuse (such as slander and intimidation), affecting 51.51% of trainees. This finding aligns with Crutche et al.'s (25) study in Canada; however, in Oman, the proportion increased to 88% (26). This highlights the widespread occurrence of verbal abuse during the SRTP period, with significant variation across different countries and regions. Prolonged exposure to verbal abuse was associated with higher levels of anxiety, depression, and occupational burnout, which may relate to changes in trainees' professional identity and future career choices, even suicidal thoughts (27). Additionally, verbal abuse was associated with lower self-confidence, diminish their motivation to learn, and hinder their clinical skills, ultimately compromising the quality of training.
49.25% of trainees reported being required to perform personal services, reflecting the presence of implicit power abuse during the SRTP period. Although being required to perform personal services does not involve direct verbal or physical abuse, it essentially constitutes a misuse of authority. This behavior is rooted in the long-standing hierarchical culture within the medical field, where superiors leverage their authority to demand tasks beyond the trainees' scope of learning. Trainees, being in a subordinate position, are often inclined to comply with such instructions (28). Tasks unrelated to training objectives were associated with less learning time, potentially diminish the quality of training, and are correlated with increased feelings of frustration or being undervalued among trainees. Furthermore, such practices could perpetuate a cycle of power abuse, as today's trainees may emulate these behaviors when they become superiors in the future.
A total of 47.14% of the trainees had experienced gender discrimination. Gender discrimination among medical students during their academic career was experienced significantly more often by women than men (21). In particular, males were long considered more suitable than females for surgical careers, due to traditionally accepted gender norms and stereotypes (29). Moreover, gender discrimination was associated with patterns that may contribute to persistent underrepresentation of women in certain specialties. When fewer women enter certain specialties due to discrimination, the representation of women in these fields further diminishes, reinforcing existing gender stereotypes (30).
The results of this study indicate that residency trainees who have encountered at least one APE have higher occupational burnout score. Looking at the different exposure levels of APEs, higher APEs exposure levels were associated with higher occupational burnout scores (P < 0.001). These findings underscore the association of APEs on the negative psychological wellbeing of residency trainees. The observed positive correlation between APEs exposure and occupational burnout aligns with prior research, which has established hostile learning environments and emotional harm as significant contributors to burnout among healthcare workers (31, 32). Chen et al. (33) find that healthcare workers with workplace violence exposure, particularly to emotional abuse, threats, and verbal sexual harassment, demonstrate higher susceptibility to burnout. This study further suggests that even limited or occasional exposure to APEs may not be benign and could have lasting psychological repercussions for residency trainees.
Due to the cross-sectional design of this study, these findings indicate associations rather than causal relationships; longitudinal studies are needed to examine potential causal mechanisms.
Burnout can lead to many challenges, including a physician's mental health issues such as suicidal tendencies and physical symptoms such as fatigue and headaches, as well as health system troubles such as poor doctor-patient relationships and clinical malpractice (15). The findings of this study have several important clinic implications for clinical education, hospital management, and resident wellbeing. Firstly, based on our findings that verbal, emotional, and physical abuse, as well as pregnancy/childcare-related discrimination, are prevalent among residency trainees, clear anti-verbal abuse policies should be formulated and enforced, establishing accessible, anonymous complaint and reporting mechanisms to enable trainees to seek help safely. Secondly, SRTP should incorporate targeted courses and workshops aimed at reducing burnout, including stress management and resilience training, mindfulness-based interventions, time management courses, and communication skills workshops for both trainees and supervisors. These initiatives are designed to foster respectful mentor-trainee relationships, improve coping strategies, and reduce conflicts and abusive behaviors. Thirdly, considering that residents reported being required to perform personal tasks unrelated to training objectives, systems must be established to clearly define the scope of responsibilities for residents, explicitly prohibiting the assignment of personal tasks unrelated to training objectives; this is crucial to combat power abuse and protect trainees' time and energy for learning. Furthermore, within the medical field, especially in traditionally male-dominated specialties such as surgery, active promotion of gender equality is essential to ensure equal opportunities in education, training, and career advancement for both women and men; increasing the visibility of female role models also helps to break down the constraints of gender stereotypes (34). Additionally, management should implement reasonable distribution of workload and on-call frequency for residents to prevent physical and mental exhaustion from overwork. Finally, it is vital to strengthen and improve accessible psychological support services for residents, ensuring they can obtain timely and effective professional help when facing stress or injustice.
Limitations
5
This study has several limitations. First, a retrospective approach was used to assess APEs, relying on self-reports from residency trainees, which may be subject to recall bias. Second, the generalizability of our findings may be limited. While the sampling strategy ensured good representativeness within the western coastal region of China where the study was conducted, the results may not be fully applicable to other Chinese regions with vastly different socioeconomic profiles or to distinct international medical training systems. Lastly, workload-related variables (e.g., working hours, night shifts, and training pressure) were not included as potential confounders, which may have influenced the observed associations between APEs and occupational burnout.
Conclusions
6
This study revealed a high prevalence of occupational burnout among residency trainees in Guangxi Province, China. A strong positive association was observed between APEs and burnout: trainees experiencing at least one APE reported significantly higher burnout levels, and increasing exposure to APEs was consistently linked to higher burnout scores. The most prevalent APEs contributing to this burden were verbal abuse, demands for personal services, and gender discrimination. It is recommended that training management departments improve relevant regulations and policies to safeguard the legal rights of residency trainees at the institutional level. Training centers should also allocate work intensity more reasonably, reduce excessive workload, and enhance attention to trainees' mental health and provide necessary interventions. At the individual level, trainees should strengthen their psychological adjustment skills, seek support and help, manage expectations appropriately, and maintain both physical and mental wellbeing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yang X Zheng D Wan P Luo X Zhang M Zhang L . Standard ophthalmology residency training in China: an evaluation of resident satisfaction on training program in Guangdong Province. BMC Med Educ. (2023) 23:550. doi: 10.1186/s 12909-023-04527-337537562 PMC 10401789 · doi ↗ · pubmed ↗
- 2Ye GC Liu CP Li W Zhu HC Lv L Zhu ZH . Effectiveness of multiple teaching methods in standardized training of internal medicine residents in China: a network meta-analysis. BMC Med Educ. (2025) 25:535. doi: 10.1186/s 12909-025-07020-140234869 PMC 11998199 · doi ↗ · pubmed ↗
- 3Zhu J Li W Chen L. Doctors in China: improving quality through modernisation of residency education. Lancet. (2016) 388:1922–9. doi: 10.1016/S 0140-6736(16)00582-127339756 · doi ↗ · pubmed ↗
- 4Cormack D Gooder C Jones R Lacey C Stanley J Paine SJ . Māori medical student and physician exposure to racism, discrimination, harassment, and bullying. JAMA Network Open. (2024) 7:e 2419373. doi: 10.1001/jamanetworkopen.2024.1937338949810 PMC 11217868 · doi ↗ · pubmed ↗
- 5Averbuch T Eliya Y Van Spall HGC. Systematic review of academic bullying in medical settings: dynamics and consequences. BMJ Open. (2021) 11:e 043256. doi: 10.1136/bmjopen-2020-04325634253657 PMC 8311313 · doi ↗ · pubmed ↗
- 6Fnais N Soobiah C Chen MH Lillie E Perrier L Tashkhandi M . Harassment and discrimination in medical training: a systematic review and meta-analysis. Acad Med. (2014) 89:817–27. doi: 10.1097/ACM.000000000000020024667512 · doi ↗ · pubmed ↗
- 7Stratton TD Mc Laughlin MA Witte FM Fosson SE Nora LM. Does students' exposure to gender discrimination and sexual harassment in medical school affect specialty choice and residency program selection? Acad Med. (2005) 80:400–8. doi: 10.1097/00001888-200504000-0002015793027 · doi ↗ · pubmed ↗
- 8Venkataraman S Nguyen M Chaudhry SI Desai MM Hajduk AM Mason HRC . Racial and ethnic discrimination and medical students' identity formation. JAMA Network Open. (2024) 7:e 2439727. doi: 10.1001/jamanetworkopen.2024.3972739412803 PMC 11581615 · doi ↗ · pubmed ↗