Hyperferritinemia Drives Risk: Unravelling the Association Between Ferritin Levels and Multi-Organ Dysfunction in Acute Febrile Illness: An Emergency Medicine Perspective
Neeraj Singla, Neha Sharma, Nalin Sharma, Mandip Bhatia, Navneet Sharma

TL;DR
High ferritin levels are linked to severe illness and death in patients with fevers and organ failure, especially in older individuals.
Contribution
This study identifies serum ferritin as a novel prognostic marker for mortality and multi-organ dysfunction in acute febrile illness.
Findings
Elevated serum ferritin levels were significantly associated with increased mortality in patients with acute febrile illness.
Older patients and those with neurological symptoms or respiratory distress had higher mortality rates.
Serum ferritin levels correlated with prolonged hospital stays and multi-organ dysfunction.
Abstract
Background: Hyperferritinemia has been increasingly recognized as a marker of systemic inflammation, immune dysregulation, and multi-organ failure. This study examines the association between vital signs, laboratory parameters (including serum ferritin), and clinical outcomes (discharge and mortality) among patients presenting with acute febrile illness and multi-organ dysfunction in a tropical emergency department. Aim: To determine the association between serum ferritin levels and multi-organ failure in patients with acute febrile illness. Methods: The study was conducted in the emergency department of a tertiary-level institute. Patients with acute febrile illness and multi-organ dysfunction without a definitive diagnosis were enrolled. All participants underwent routine blood investigations (hemogram, liver, and renal function tests), tropical serology (dengue, leptospirosis,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
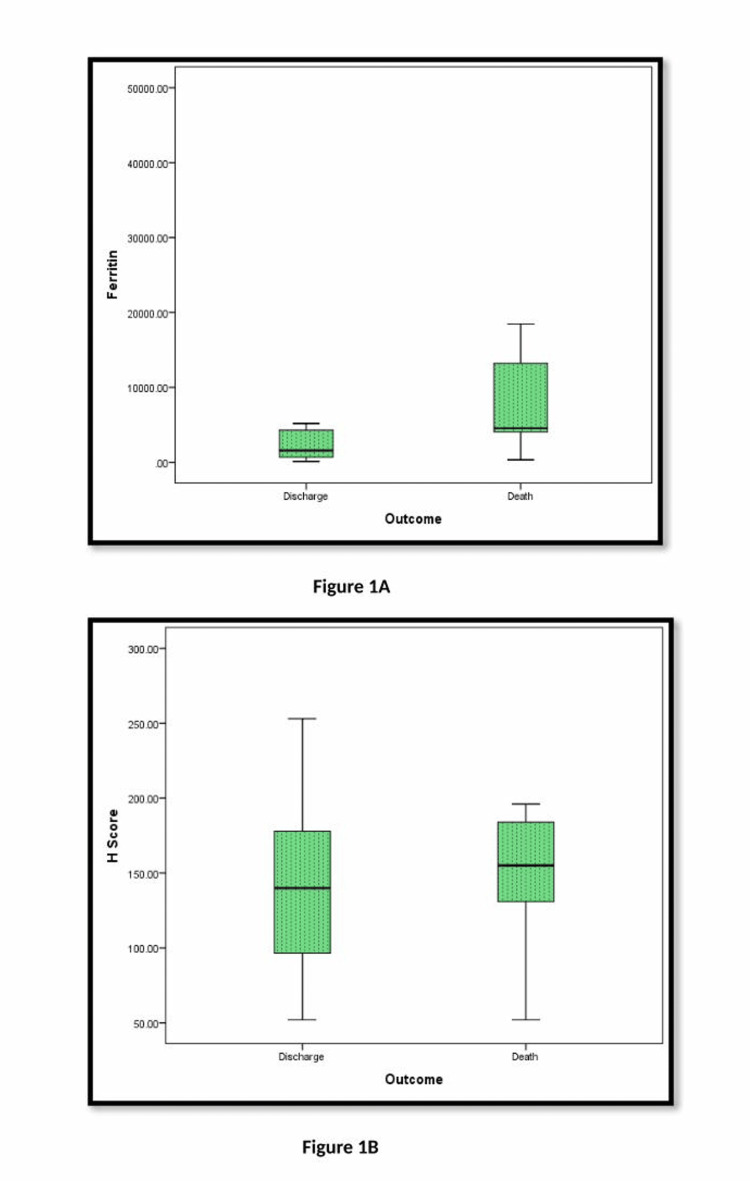 Figure 1
Figure 1| Survivors (61)84.72% | Non-survivors (11)15.27% | Chi-Square Test | p-value | |
| Fever | 58(95.1%) | 11(100%) | 0.565 | 0.452 |
| Arthralgias | 2(3.3%) | 1(9.1%) | 0.788 | 0.375 |
| Rash | 4(6.6%) | 2(18.2%) | 1.649 | 0.199 |
| Bleeding Manifestations | 14(23.0%) | 2(18.2%) | 0.123 | 0.726 |
| Petechiae | 4(6.6%) | 1(9.1%) | 0.093 | 0.761 |
| Mucosal Bleed | 6(9.8%) | 3(27.3%) | 2.591 | 0.108 |
| Major Organ Bleed | 13(21.3%) | 2(18.2%) | 0.055 | 0.814 |
| Joint Pains | 2(3.3%) | 1(9.1%) | 0.788 | 0.375 |
| Myalgias | 26(42.6%) | 4(36.4%) | 0.150 | 0.698 |
| GI Symptoms | 29(47.5%) | 5(45.5%) | 0.160 | 0.898 |
| Urinary Symptoms | 11(18.0%) | 2(18.2%) | 0.000 | 0.991 |
| AMS | 14(23.0%) | 8(72.7%) | 10.882 | 0.001 |
| Respiratory Symptoms | 25(41.0%) | 9(81.8%) | 6.235 | 0.013 |
| Co-morbidities | ||||
| Diabetes Mellitus | 10(16.4%) | 2(18.2%) | 0.021 | 0.884 |
| Hypertension | 11(18.0%) | 2(18.2%) | 0.000 | 0.991 |
| COPD | 1(1.6%) | 3(27.3%) | 11.671 | 0.001 |
| CAD | 1(1.6%) | 1(9.1%) | 1.872 | 0.171 |
| CLD | 0(0%) | 0(0%) | ||
| CKD | 4(6.6%) | 2(18.2%) | 1.649 | 0.199 |
| Lab investigations | Survivors | Non-Survivors | ||||
| Mean | Standard Deviation | Mean | Standard Deviation | T-value Mann-Whitney test | p-value | |
| HB | 12.24 | 2.83 | 11.66 | 1.84 | .653 | .516 |
| TLC | 12041.15 | 17650.38 | 12336.36 | 7702.89 | 1.127 | 0.26 |
| Platelets | 33391.72 | 40664.91 | 43818.18 | 26301.40 | 1.722 | 0.085 |
| Neutrophils | 62.24 | 13.94 | 68.36 | 16.66 | 1.301 | .198 |
| Lymphocytes | 23.54 | 12.62 | 18.59 | 15.95 | 1.150 | .254 |
| HCT | 37.87 | 8.14 | 36.42 | 8.33 | 0.541 | .590 |
| CRP | 70.70 | 68.80 | 93.71 | 66.26 | 0.839 | .405 |
| Ferritin | 7963.27 | 17821.86 | 12654.78 | 19376.25 | 2.115 | .034* |
| Triglycerides (TG) | 277.76 | 173.01 | 265.40 | 212.55 | 0.148 | .883 |
| Fibrinogen | 3.01 | 1.51 | 2.74 | 2.52 | 0.366 | .716 |
| H Score | 140.89 | 55.35 | 143.60 | 57.13 | 0.102 | .919 |
| Urea | 68.96 | 66.92 | 135.09 | 74.64 | 3.194 | .001** |
| Creatinine | 1.66 | 1.76 | 3.09 | 1.77 | 2.85 | .004** |
| Sodium (Na) | 135.33 | 7.62 | 138.55 | 6.31 | 1.319 | .192 |
| Potassium(K) | 4.37 | .66 | 4.58 | .75 | 0.935 | .353 |
| Bilrubin | 2.30 | 3.13 | 4.84 | 6.87 | 1.698 | 0.089 |
| SGOT | 991.74 | 2141.78 | 1425.55 | 1889.93 | 2.34 | .019* |
| SGPT | 566.43 | 1297.26 | 589.45 | 722.82 | 1.980 | .048* |
| ALP | 191.68 | 159.73 | 241.64 | 117.32 | 1.857 | 0.063 |
| Albumin | 2.96 | .71 | 2.68 | .66 | 1.236 | .221 |
| Tropical Serology | Chi-square test | |||||
| Dengue | 45(73.77%) | 8(72.7%) | 0.123 | 0.739 | ||
| Scrub Typhus | 11(18.03%) | 3(27.3%) | 0.395 | 0.53 | ||
| Leptospirosis | 6(9.8%) | 1(9.1%) | 0.016 | 0.96 | ||
| Chikungunya | 5(8.19%) | 1(9.1%) | 0.003 | 0.96 | ||
| Enteric Fever | 0 | 0 | ||||
| Malaria | 0 | 0 | ||||
| No Specific Diagnosis | 5(8.19%) | 0 | 1.224 | 0.269 | ||
| Survivors: 61(84.72%) | Non-Survivors :11(15.27%) | Chi-Square Test | p-value | |
| ARDS | 28(45.9%) | 8(72.72%) | 3.997 | 0.046 |
| Severe Bleeding | 15(24.59%) | 1(9.09%) | 1.048 | 0.306 |
| Renal Failure | 24(39.3%) | 7(63.63%) | 3.282 | 0.07 |
| Encephalitis | 11(18.03%) | 7(63.63%) | 12.26 | 0.0001 |
| Shock | 12(19.67%) | 6(54.5%) | 7.383 | 0.007 |
| Hepatitis | 46(75.4%) | 8(72.72%) | 0.099 | 0.753 |
| Myocarditis | 11(18.03%) | 6(54.5%) | 8.309 | 0.004 |
| Coagulopathy | 8(13.11%) | 4(36.3%) | 4.422 | 0.035 |
| Musculoskeletal Manifestations | 5(8.19%) | 0 | 0.882 | 0.348 |
| >1 Complication | 40(65.6%) | 7(63.6%) | 0.675 | 0.784 |
| Duration of Hospital Stay | 6.189 | 0.045 | ||
| ≤ 5 days | 24(39.3%) | 5(45.45%) | ||
| 6-10 days | 28(45.9%) | 3(27.27%) | ||
| >10 days | 9(14.7%) | 3(27.27%) | ||
| Random Donor Platelet Transfusion | 26(42.6%) | 3(27.3%) | 0.913 | 0.339 |
| Single Donor Platelet Transfusion | 22(36.1%) | 2(18.2%) | 1.341 | 0.247 |
| Ferritin | ||
| Pearson Correlation | p-value | |
| GCS | -.005 | .972 |
| SBP | -.027 | .839 |
| DBP | -.006 | .966 |
| Pulse | .066 | .614 |
| Spo2 | .130 | .318 |
| HB | .223 | .084 |
| TLC | .140 | .281 |
| PLATELETS | -.106 | .416 |
| NEUTROPHILS | -.015 | .906 |
| LYMPHOCYTES | -.149 | .253 |
| HCT | .167 | .197 |
| CRP | -.029 | .830 |
| TG | .053 | .731 |
| Fibrinogen | -.237 | .113 |
| H Score | .273 | .089 |
| UREA | .023 | .859 |
| Creat | .153 | .240 |
| Na | -.259* | .044 |
| K | .321* | .012 |
| BILRUBIN | -.026 | .840 |
| SGOT | .435** | .000 |
| SGPT | .296* | .021 |
| ALP | .016 | .906 |
| Albumin | -.007 | .956 |
| Duration of Hospital Stay | .085 | .536 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIron Metabolism and Disorders · Hemoglobinopathies and Related Disorders · Malaria Research and Control
Introduction
Acute febrile illness (AFI) is one of the leading causes of hospital admissions in tropical countries, particularly during the monsoon and post-monsoon seasons. These illnesses are attributed to a diverse array of pathogens, including Plasmodium species (malaria), Leptospira (leptospirosis), Rickettsia (scrub typhus), Salmonella typhi/paratyphi (enteric fever), and arboviruses such as Dengue and Chikungunya [1,2]. In many cases, these infections can progress to systemic inflammatory response syndrome (SIRS) and multi-organ dysfunction syndrome (MODS), resulting in significant morbidity and mortality in adult patients.
Early identification of biomarkers that reflect disease severity is crucial for guiding triage and management decisions. Serum ferritin, traditionally recognized for its role in iron metabolism, has recently garnered interest as a potential prognostic biomarker in systemic inflammation and sepsis [3]. Marked elevations in ferritin are observed in hyperinflammatory conditions, including hemophagocytic lymphohistiocytosis (HLH), adult-onset Still’s disease, septic shock, and severe viral infections [4].
Hyperferritinemia may reflect macrophage activation and cytokine storm, which are commonly observed in severe tropical infections. Notably, significantly elevated ferritin levels have been documented in severe dengue and scrub typhus, both of which are frequent causes of MODS in tropical regions [5,6]. Similarly, in leptospirosis and malaria, increased ferritin is associated with greater disease severity and poorer outcomes [7]. These findings highlight the potential of ferritin as a surrogate marker for disease burden and immune dysregulation in tropical febrile illnesses.
Despite this, there remains a paucity of data evaluating the relationship between serum ferritin levels and clinical outcomes in adult patients presenting with AFI and MODS in emergency departments during tropical seasons. Given the nonspecific nature of early symptoms in many tropical infections, ferritin could serve as a valuable adjunct in early risk stratification.
This study aims to explore the association of serum ferritin levels and disease severity in adult participants with acute febrile illness presenting with multi-organ dysfunction syndrome in a tropical medical emergency setting. The findings could enhance our understanding of the prognostic role of ferritin and potentially inform early intervention strategies.
Materials and methods
This prospective observational study was conducted in the Medicine Emergency Department of a premier tertiary care institute, following approval from the Institutional Ethics Committee. The study focused on patients presenting with acute febrile illness (AFI) and multi-organ dysfunction syndrome (MODS).
Patient population
Patients aged over 12 years with acute febrile illness, defined as fever >38.3°C persisting for more than 48 hours and with onset within the preceding 14 days, were eligible for inclusion. Enrollment required the presence of at least two of the following clinical features: a) Cytopenias (platelet count <100,000/cu.mm or total leucocyte count <4,000/cu.mm), b) hepatomegaly and/or splenomegaly, c) lymphadenopathy, d) systemic signs (rash, edema), e) respiratory distress, f) encephalopathy.
All patients underwent a comprehensive diagnostic workup, including tropical serologies (dengue, malaria, scrub typhus, Leptospira, typhoid), serum ferritin levels, lipid profile, and bone marrow examination in patients who were alert or regained consciousness, indicated for the diagnosis of hemophagocytes, and the H score was calculated.
Hyperferritinemia was defined as ferritin levels greater than 500 ng/mL and measured by standard automated chemiluminescence immunoassays. The H score is a weighted scoring system based on nine variables, including fever greater than 38.3°C, cytopenias, splenomegaly, hypofibrinogenemia, hypertriglyceridemia, hyperferritinemia (greater than 500 ng/mL), hemophagocytosis in the bone marrow, hepatomegaly, and elevated transaminases. A detailed bilingual patient information sheet was provided, and written informed consent was obtained from all participants.
Outcomes
The primary outcome was the correlation of serum ferritin levels measured at admission with mortality in patients with undifferentiated acute febrile illness. Secondary outcomes included the incidence of unfavorable complications in patients with MODS due to tropical infections associated with hyperferritinemia.
Statistical analysis
All data were entered into Microsoft Excel (Redmond, USA) and analyzed using IBM Corp. Released 2018. IBM SPSS Statistics for Windows, Version 24. Armonk, NY: IBM Corp. Quantitative variables were summarized as mean ± standard deviation (SD), and normality was assessed using the Kolmogorov-Smirnov test (n>50). Categorical variables were compared between survivors and non-survivors using the chi-square test or Fisher’s exact test, as appropriate. For intergroup comparisons of laboratory parameters, either the independent two-sample t-test or the Mann-Whitney U test was employed, depending on data distribution. A p-value < 0.05 was considered statistically significant.
Results
This study examined demographic distribution, clinical symptoms, comorbidities, laboratory parameters, and clinical outcomes among 72 patients with hyperferritinemia in sepsis patients with multi-organ dysfunction syndrome.
The mean age of patients was 42.75 years (range: 13-95 years). Most patients (27.4%) were in the 31-40 age group. Males constituted 44 (61.11%) of cases, while females were 28 (38.9999%). Among the clinical presentations, fever was present in 69 (95.8%), followed by respiratory distress and gastrointestinal symptoms in 35 (47.9%), myalgias in 31 (42.5%), bleeding manifestations in 16 (22.2%), urinary symptoms in 13 (17.8%), altered mental sensorium in 22 (30.1%), and joint pain and arthralgias in less than 5% of patients. In bleeding manifestations, major organ bleed was present in 15 (20.8%), mucosal bleed was present in 9 (12.5%), and petechiae was present in 5 (6.9%), which is highlighted in Table 1.
Table 1: Comparison of symptoms and co-morbidities between survivors and non-survivors in patients with acute febrile illness and ferritin elevation (n=72) (p<0.05 is considered significant)AMS: Acute Mountain Sickness, COPD: Chronic Obstructive Pulmonary Disease, CAD: Coronary Artery Disease, CLD: Chronic Liver Disease, CKD: Chronic Kidney Disease
On clinical examination, the mean Glasgow Coma Scale (GCS) score was found to be 13.36. Systolic blood pressure (SBP) averaged 114.50 mmHg, while diastolic blood pressure (DBP) was 72.14 mmHg.
Mean hemoglobin (HB) was 12.15 g/dL, and total leukocyte count (TLC) averaged 12,086.25. Platelet count was highly variable, ranging from 1.19 to 226,000. Ferritin levels had a wide distribution, with a mean of 8,655.46, which has been illustrated in Table 2.
Table 2: Comparison of laboratory investigations and tropical serologies between survivors and non-survivors in patients with acute febrile illness and ferritin elevation (p<0.05 is considered significant)HB: Hemoglobin, TLC: Total Leukocyte Count, HCT: Hematocrit, CRP: C-Reactive Protein, SGOT: Serum Glutamic Oxaloacetic Transaminase (AST), SGPT: Serum Glutamic Pyruvic Transaminase (ALT), ALP: Alkaline Phosphatase
Dengue fever was the most common infectious cause (76.8%), followed by scrub typhus (20.3%) and leptospirosis (10.1%). Malaria and enteric fever were not reported. Blood, urine, or pus cultures were positive in 13.9% of cases, with a significantly higher prevalence among non-survivors (p=0.019).
Amongst radio-imaging abnormalities, pleural effusion was observed in 38.4% of cases, ascites in 45.2%, and hepatomegaly in 30.1%. Splenomegaly was noted in 13.7% of cases. Imaging abnormalities, such as bilateral infiltrates, were found in 4.1% of patients. Dengue encephalitis was diagnosed in 1.4% of cases. Chest infiltrates, pleural effusion, and splenomegaly were more frequent in non-survivors.
Amongst the complications, serositis, bleeding manifestations, renal failure, encephalitis, shock, hepatitis, and myocarditis were seen in both survivors and non-survivors, showing a strong correlation with mortality, which is charted in Table 3.
Table 3: Comparison of complications between survivors and non-survivors in patients with acute febrile illness and ferritin elevation (p<0.05 is considered significant)ARDS: Acute Respiratory Distress Syndrome
In outcomes, 61 (84.7%) patients recovered, whereas 11 (15.3%) patients expired. During the hospital stay, <=5 days was seen in 29 (46.8%), with the highest mortality (p=0.045).
A total of 6-10 days in 28 (45.2%), and more than 10 days' stay was seen in 5 (8.1%) patients, with no recorded deaths, suggesting longer treatment duration may have improved survival.
Transfusion therapies, including random donor platelets (RDP) and single donor platelets (SDP), were administered to 29 (40.3%) and 24 (33.3%) of patients, respectively, but RDP and SDP showed no significant impact on survival, p=0.339 and p=0.247, respectively. Steroid and intravenous immunoglobulin (IVIG) use was minimal, each administered to only 1.4% of patients.
Patients who were discharged had a higher mean Glasgow Coma Scale (GCS) score (13.87) compared to those who died (10.55, p=0.002). Systolic blood pressure (SBP) was lower in deceased patients (103.64 mmHg) than in discharged ones (116.46 mmHg). Similarly, diastolic blood pressure (DBP) was reduced in non-survivors (66.36 mmHg vs. 73.18 mmHg). Non-survivors had a higher mean pulse rate (102.09 bpm) than discharged patients (97.20 bpm), while oxygen saturation (SpO2) levels were slightly higher in non-survivors (95.82%) compared to survivors (92.84%).
Renal and hepatic function
Non-survivors exhibited significantly higher blood urea levels (135.09 vs. 68.96, p=0.001) and creatinine levels (3.09 vs. 1.66, p=0.004), indicating worsening kidney function. Serum sodium (Na) was slightly higher in non-survivors (138.55 vs. 135.33), while potassium (K) levels were comparable. Bilirubin was elevated in deceased patients (4.84 vs. 2.30, p=0.019), and liver enzyme levels (SGOT: 1425.55 vs. 991.74, p=0.048; SGPT: 589.45 vs. 566.43) were higher in non-survivors, indicating hepatic dysfunction.
Association of serum ferritin was assessed by Spearman-Pearson correlation with various clinical signs and laboratory parameters depicted in Table 4, and was found significant with H score (0.089), sodium levels (0.044), hemoglobin levels (0.084), potassium levels (0.012), ALT (0.021), and AST (0.000). Box plot analysis, as shown in Figure 1, highlighted the association between the final outcomes and both Serum ferritin and H-score.
**Table 4: Association between various clinical parameters and laboratory investigations with serum ferritin (p<0.05 is considered significant) *. Correlation is significant at the 0.05 level (2-tailed); . Correlation is significant at the 0.01 level (2-tailed)GCS: Glasgow Coma Scale, SBP: Systolic Blood Pressure, DBP: Diastolic Blood Pressure, SpO₂: Peripheral Capillary Oxygen Saturation, HB: Hemoglobin, TLC: Total Leukocyte Count, HCT: Hematocrit, CRP: C-Reactive Protein, TG: Triglycerides, Na: Sodium, K: Potassium, SGOT: Serum Glutamic Oxaloacetic Transaminase (AST), SGPT: Serum Glutamic Pyruvic Transaminase (ALT), ALP: Alkaline Phosphatase
Box plot representation of the association of ferritin and HLH score with the patient’s outcome (discharge vs. death)1 A. Ferritin vs. Outcome: the median ferritin level is higher in the "Death" group compared to the "Discharge" group, which suggests that elevated ferritin is associated with a worse outcome or disease severity. (p=0.0001*)1 B. H Score vs. Outcome: A higher H score in the "Death" group suggests that patients with higher H scores are at greater risk of mortality, as the H score, often used to assess hyperinflammation, could be a prognostic marker. (p=0.819), highlighted the association between the final outcomes and both Serum ferritin, H-score.*
Discussion
This study evaluates the prognostic significance of serum ferritin in predicting the severity and outcomes of patients with acute febrile illness and MODS. The findings align with previous research that highlights ferritin as an essential biomarker in critical illnesses such as sepsis, dengue, hemophagocytic lymphohistiocytosis (HLH), and macrophage activation syndrome (MAS) [4,8]. The study establishes that higher ferritin levels are correlated with increased mortality, multi-organ dysfunction, and prolonged hospital stays, thereby reinforcing their prognostic value.
Demographic comparisons
The cohort comprised 72 patients, with a mean age of 42.75 years, and predominantly in the 31-40 age group. Males constituted 61.1% of cases. These demographic trends have been observed in tropical illness-related MODS studies, where middle-aged adults, particularly males, have a higher risk of complications [9]. The predominance of dengue fever as the underlying etiology mirrors patterns observed in endemic regions, where dengue-associated MODS frequently affects younger adults [10].
Clinical profile and comparison
Fever was the most common symptom, reported in 95.8% of patients, consistent with tropical illness-related MODS studies where fever is a primary presenting feature [11]. Other common symptoms included myalgias (42.5%), gastrointestinal symptoms (47.9%), and respiratory symptoms (47.9%). Altered mental status (30.1%) was also significantly associated with mortality (p=0.001).
A noteworthy variance from bacterial sepsis studies was the lower prevalence of hypotension at presentation, as reflected in the mean systolic (114.5 mmHg) and diastolic (72.14 mmHg) blood pressures in this cohort. In contrast, sepsis-associated MODS often presents with profound hypotension and higher shock incidence [12]. However, shock remained a strong predictor of mortality in this cohort (p = 0.007), consistent with the global critical care literature.
Laboratory investigations and pathophysiology
Hyperferritinemia was strongly associated with disease severity. The mean ferritin level was 8,655.46 ng/mL, with significantly higher levels in non-survivors (12,654.78 ng/mL) compared to survivors (7,963.27 ng/mL, p=0.034). This trend is comparable to HLH-associated MODS, where ferritin levels exceeding 10,000 ng/mL are linked to increased mortality [13]. Elevated ferritin levels in this study suggest excessive inflammation, macrophage activation, and iron-mediated oxidative stress, similar to findings in cytokine storm syndromes [14].
Complications and multi-organ failure
MODS was associated with several complications, including respiratory failure (ARDS), neurological dysfunction, and shock. Encephalitis (p=0.0001) and ARDS (p=0.046) were significantly linked to mortality, consistent with existing research on systemic inflammation-driven organ failure [15].
Coagulopathy was pointedly more in non-survivors (40% vs. 13.1%, p=0.035), mirroring trends in disseminated intravascular coagulation (DIC) studies where hyper-ferritinemia contributes to coagulopathy and thrombocytopenia [16].
An Indian study guided by Suresh SC et al. [17] found that serum ferritin levels were significantly higher in patients with severe dengue, with a cutoff value of 714 ng/ml, compared to those with mild dengue, with a sensitivity of 100% and a specificity of 43.75%. which was in concordance with this study. Similarly, in a study guided by Kurian SJ et al. [18], median ferritin levels were significantly higher in moderate to severe COVID-19 infection compared to mild (p = 0.001). Both these studies were in concordance with the present study, which re-emphasized the higher serum ferritin values with more severity of illness.
Limitations
It was a single-center study, which limited its generalizability. There was a lack of serial ferritin measurements to assess temporal trends. No adjustment was made for the effects of iron supplements or blood transfusions on ferritin. The non-survivor group (n=11) was very small in this study.
Conclusions
This study reinforces the role of ferritin as a biomarker for assessing the severity of multi-organ dysfunction syndrome in patients with acute febrile illness. Given its strong association with systemic inflammation and organ failure, early ferritin measurement could help stratify patients based on risk, allowing for timely interventions such as immunomodulatory therapy. The findings indicate that neurological deterioration, renal impairment, elevated inflammatory markers, and hepatic dysfunction are significant contributors to mortality in ferritin-related conditions. Higher ferritin and C-reactive protein (CRP) levels were indicative of a more severe inflammatory state, and patients with pronounced metabolic and organ dysfunction exhibited poorer prognoses. Notably, dengue fever emerged as the most prevalent infectious etiology associated with hyperferritinemia in this cohort.
Effective management strategies should prioritize early detection, rigorous infection control, and comprehensive organ support to improve survival outcomes in patients with ferritin-related multi-organ dysfunction. We recommend measuring serum ferritin within 24 hours of admission in all acute febrile illness patients presenting with ≥2 organ dysfunctions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The etiology of febrile illness in adults presenting to Patan hospital in Kathmandu, Nepal Am J Trop Med Hyg Murdoch R Woods W Zimmerman D 670675702004 https://pubmed.ncbi.nlm.nih.gov/15211012/15211012 · pubmed ↗
- 2Scrub typhus: an unrecognized threat in South India - clinical profile and predictors of mortality Trop Doct Chrispal A Boorugu H Gopinath KG 1291334020102036042610.1258/td.2010.090452 · doi ↗ · pubmed ↗
- 3Hyperferritinemia and inflammation Int Immunol Kernan KF Carcillo JA 4014092920172854143710.1093/intimm/dxx 031PMC 5890889 · doi ↗ · pubmed ↗
- 4The hyperferritinemic syndrome: macrophage activation syndrome, Still's disease, septic shock and catastrophic antiphospholipid syndrome BMC Med Rosário C Zandman-Goddard G Meyron-Holtz EG 1851120132396828210.1186/1741-7015-11-185PMC 3751883 · doi ↗ · pubmed ↗
- 5Ferritin levels predict severe dengue Infection Soundravally R Agieshkumar B Daisy M 13194320152535473310.1007/s 15010-014-0683-4 · doi ↗ · pubmed ↗
- 6Clinical profile and improving mortality trend of scrub typhus in South India Int J Infect Dis Varghese GM Trowbridge P Janardhanan J 39432320142466193110.1016/j.ijid.2014.02.009 · doi ↗ · pubmed ↗
- 7Haemophagocytic lymphohistiocytosis with leptospirosis: a rare but devastating complication Case Rep Infect Dis Munasinghe BM Arambepola AG Pathirage N 3451155202120213433631510.1155/2021/3451155 PMC 8295509 · doi ↗ · pubmed ↗
- 8Macrophage activation-like syndrome: a distinct entity leading to early death in sepsis Front Immunol Karakike E Giamarellos-Bourboulis EJ 551020193076653310.3389/fimmu.2019.00055 PMC 6365431 · doi ↗ · pubmed ↗