Survival in stage IV non-small cell lung cancer patients based on radiation dose to immune cells: a retrospective analysis
Changxing Feng, Kang Wang, Tao Hu, Fuhao Xu, Li Li, Shuanghu Yuan

TL;DR
This study shows that radiation dose to immune cells (EDRIC) and other factors can predict survival in stage IV lung cancer patients receiving immunotherapy.
Contribution
The study introduces EDRIC as a novel prognostic factor and demonstrates its combined predictive power with lymphocyte nadir and ALI.
Findings
Higher EDRIC is linked to worse overall and progression-free survival in stage IV NSCLC patients.
A model combining EDRIC, lymphocyte nadir, and ALI outperforms single-factor models in predicting survival.
Findings were validated in an external cohort, confirming the model's reliability.
Abstract
Programmed death-1 (PD-1)/programmed death-ligand 1 (PD-L1) immune checkpoint inhibitors combined with chemotherapy represent the standard first-line treatment for stage IV non-small cell lung cancer (NSCLC) without driver mutations. Both concurrent and sequential thoracic radiotherapy (RT) have been shown to improve survival outcomes. This study aimed to evaluate the prognostic significance of the estimated dose of radiation to immune cells (EDRIC) in stage IV NSCLC patients receiving first-line immunotherapy (IT), as well as the predictive performance of EDRIC in combination with inflammatory parameters for overall survival (OS). This multicenter retrospective study included 167 stage IV NSCLC patients who received concurrent or sequential RT in addition to IT. Spearman’s rank correlation was applied to assess associations between variables. Kaplan-Meier and Cox regression analyses…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
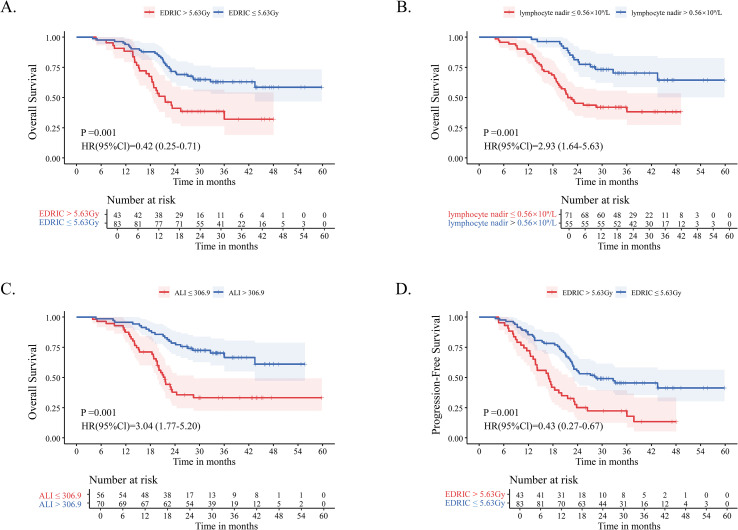 Figure 1
Figure 1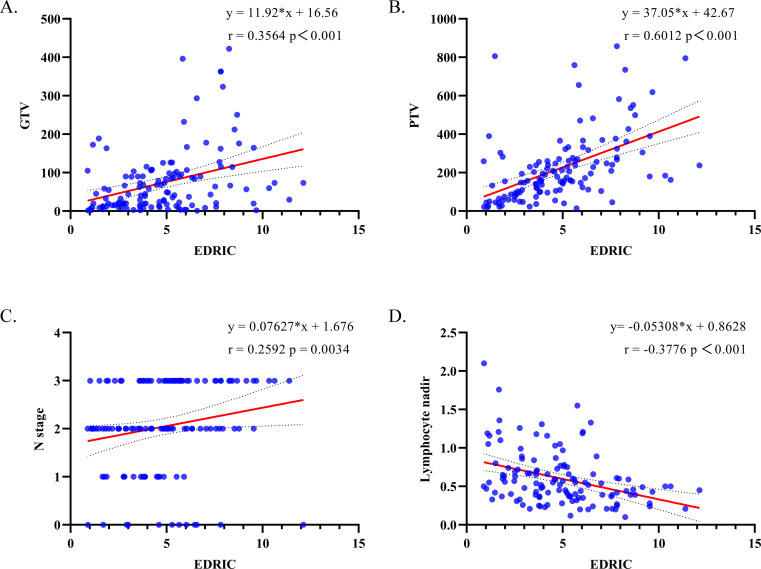 Figure 2
Figure 2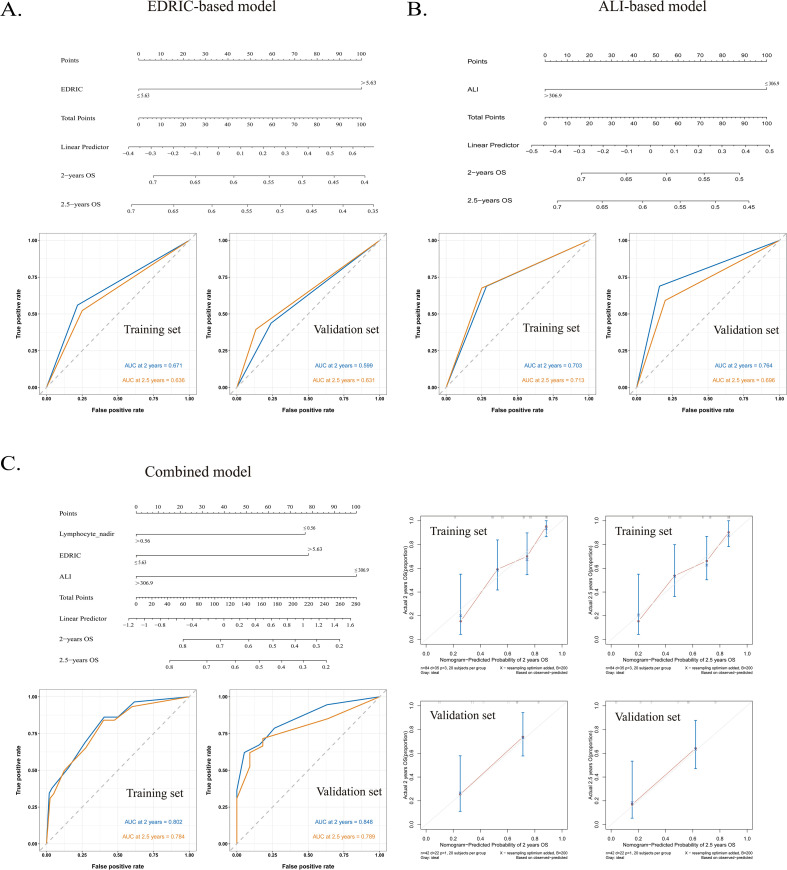 Figure 3
Figure 3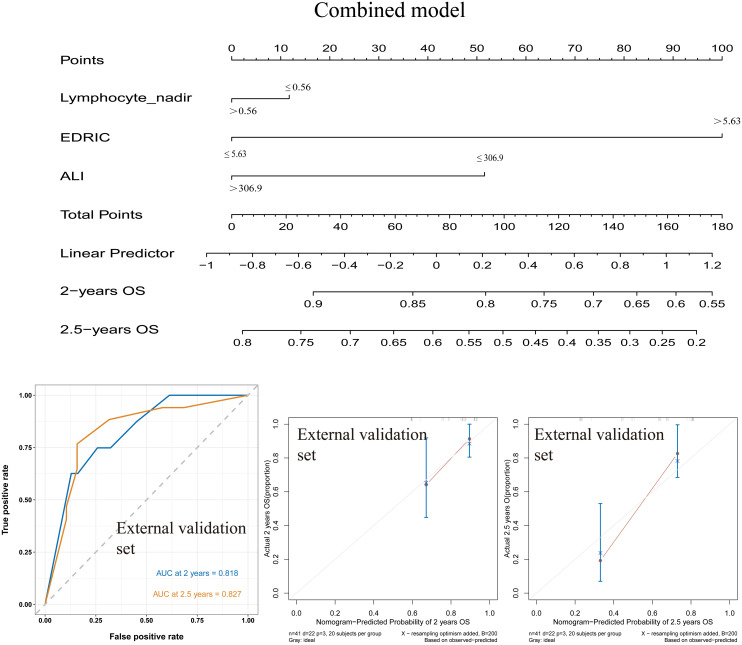 Figure 4
Figure 4| Characteristics | Total (%) (n=126) |
|---|---|
| Gender | |
| Male | 96 (76.2) |
| Female | 30 (23.8) |
| Age (y) | |
| (Median, range) | 64 (36-79) |
| <65 | 56 (44.4) |
| ≥65 | 70 (55.6) |
| ECOG | |
| 0-1 | 118 (93.7) |
| ≥2 | 8 (6.3) |
| Smoking history | |
| Yes | 72 (57.1) |
| No | 54 (42.9) |
| Alcohol consumption | |
| Yes | 51 (40.5) |
| No | 75 (59.5) |
| Comorbidities | |
| Yes | 50 (39.7) |
| No | 76 (60.3) |
| History | |
| Squamous cell carcinoma | 44 (34.9) |
| Adenocarcinoma | 78 (61.9) |
| Others | 4 (3.2) |
| PDL1 Expression | |
| <1% | 20 (15.9) |
| ≥1% | 42 (33.3) |
| Unknown | 64 (50.8) |
| T stage | |
| T1 | 24 (19.0) |
| T2 | 35 (27.8) |
| T3 | 21 (16.7) |
| T4 | 46 (36.5) |
| N stage | |
| N0 | 12 (9.5) |
| N1 | 18 (14.3) |
| N2 | 48 (38.1) |
| N3 | 48 (38.1) |
| Stage | |
| IVA | 61 (48.4) |
| IVB | 65 (51.6) |
| Chemotherapy regimen | |
| PC | 63 (50.0) |
| PP | 18 (14.3) |
| TP | 16 (12.7) |
| TC | 29 (23.0) |
| Presence of brain metastasis | |
| Yes | 83 (65.9) |
| No | 43 (34.1) |
| Presence of liver metastasis | |
| Yes | 68 (54.0) |
| No | 58 (46.0) |
| Presence of bone metastasis | |
| Yes | 54 (42.9) |
| No | 72 (57.1) |
| PET staging | |
| Yes | 54 (42.9) |
| No | 72 (57.1) |
| Tumor location | |
| Lower | 43 (34.1) |
| Middle | 12 (9.6) |
| Upper | 71 (56.3) |
| Location | |
| Left lung | 57 (45.2) |
| Right lung | 69 (54.8) |
| GTV (cm3) | |
| (Median, range) | 48.8 (1.2-422.2) |
| PTV (cm3) | |
| (Median, range) | 179.9 (14.8-857.5) |
| Lymphocyte nadir (109/L) | |
| (Median, range) | 0.52 (0.1-2.1) |
| EDRIC (Gy) | |
| (Median, range) | 4.76 (0.89-12.12) |
| Variable | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
|
|
|
|
| |
| Age | ||||
| <60 |
| |||
| ≥60 |
|
| ||
| Gender | ||||
| Male |
| |||
| Female |
|
| ||
| ECOG PS | ||||
| 0-1 |
| |||
| ≥2 |
|
| ||
| Smoking history | ||||
| Yes |
| |||
| No |
|
| ||
| Comorbidities | ||||
| Yes |
| |||
| No |
|
| ||
| History | ||||
| Squamous cell carcinoma |
| |||
| Adenocarcinoma |
|
| ||
| Others |
|
| ||
| PDL1 Expression | ||||
| <1% |
| |||
| ≥1% |
|
| ||
| Unknown |
|
| ||
| Location | ||||
| Left lung |
| |||
| Right lung |
|
| ||
| T stage | ||||
| T1 |
| |||
| T2 |
| 0.411 | ||
| T3 |
| 0.880 | ||
| T4 |
| 0.855 | ||
| N stage | ||||
| N+ |
| |||
| N0 |
| 0.501 | ||
| Stage | ||||
| IVA |
| |||
| IVB |
|
| ||
| Chemotherapy regimen | ||||
| |
| |||
| |
|
| ||
| |
|
| ||
| |
|
| ||
| Brain metastasis | ||||
| No |
| |||
| Yes |
| 0.661 | ||
| Liver metastasis | ||||
| No |
| |||
| Yes |
| 0.943 | ||
| Bone metastasis | ||||
| No |
| |||
| Yes |
| 0.670 | ||
| Brain radiotherapy | ||||
| No |
| |||
| Yes |
| 0.336 | ||
| Liver radiotherapy | ||||
| No |
| |||
| Yes |
| 0.114 | ||
| Bone radiotherapy | ||||
| No |
| |||
| Yes |
| 0.982 | ||
| Tumor location | ||||
| Lower |
| |||
| Middle |
|
| ||
| Upper |
|
| ||
| NLR | ||||
| > 2.79 |
|
| ||
| ≤ 2.79 |
|
|
| 0.754 |
| PLR | ||||
| > 143.8 |
|
| ||
| ≤ 143.8 |
|
|
| 0.934 |
| LMR | ||||
| > 2.07 |
|
| ||
| ≤ 2.07 |
|
|
| 0.597 |
| SII | ||||
| > 844 |
|
| ||
| ≤ 844 |
| 0.001 |
| 0.574 |
| PNI | ||||
| > 49.7 |
| |||
| ≤ 49.7 |
| 0.092 | ||
| ALI | ||||
| > 306.9 |
|
| ||
| ≤ 306.9 |
| 0.001 |
|
|
| Lymphocyte nadir | ||||
| > 0.56×109/L |
|
| ||
| ≤ 0.56×109/L |
|
|
|
|
| EDRIC | ||||
| > 5.63Gy |
|
| ||
| ≤ 5.63Gy |
|
|
|
|
| Variable | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
|
|
|
|
| |
| Age | ||||
| <60 |
| |||
| ≥60 |
|
| ||
| Gender | ||||
| Male |
| |||
| Female |
|
| ||
| ECOG PS | ||||
| 0-1 |
| |||
| ≥2 |
|
| ||
| Smoking history | ||||
| Yes |
| |||
| No |
|
| ||
| Comorbidities | ||||
| Yes |
| |||
| No |
|
| ||
| History | ||||
| Squamous cell carcinoma |
| |||
| Adenocarcinoma |
|
| ||
| Others |
|
| ||
| PDL1 Expression | ||||
| <1% |
| |||
| ≥1% |
|
| ||
| Unknown |
|
| ||
| Location | ||||
| Left lung |
| |||
| Right lung |
|
| ||
| T stage | ||||
| T1 |
| |||
| T2 |
| 0.484 | ||
| T3 |
| 0.666 | ||
| T4 |
| 0.409 | ||
| N stage | ||||
| N+ |
| |||
| N0 |
| 0.897 | ||
| stage | ||||
| IVA |
| |||
| IVB |
|
| ||
| Chemotherapy regimen | ||||
| PC |
| |||
| PP |
|
| ||
| TP |
|
| ||
| TC |
|
| ||
| Brain metastasis | ||||
| No |
| |||
| Yes |
| 0.973 | ||
| Liver metastasis | ||||
| No |
| |||
| Yes |
| 0.854 | ||
| Bone metastasis | ||||
| No |
| |||
| Yes |
| 0.923 | ||
| Brain radiotherapy | ||||
| No |
| |||
| Yes |
| 0.119 | ||
| Liver radiotherapy | ||||
| No |
| |||
| Yes |
| 0.261 | ||
| Bone radiotherapy | ||||
| No |
| |||
| Yes |
| 0.330 | ||
| Tumor location | ||||
| Lower |
| |||
| Middle |
| 0.464 | ||
| Upper |
| 0.656 | ||
| NLR | ||||
| > 2.79 |
|
| ||
| ≤ 2.79 |
|
|
| 0.928 |
| PLR | ||||
| > 143.8 |
|
| ||
| ≤ 143.8 |
|
|
| 0.120 |
| LMR | ||||
| > 2.07 |
| |||
| ≤ 2.07 |
|
| ||
| SII | ||||
| > 844 |
|
| ||
| ≤ 844 |
| 0.001 |
| 0.330 |
| PNI | ||||
| > 49.7 |
| |||
| ≤ 49.7 |
| 0.329 | ||
| ALI | ||||
| > 306.9 |
|
| ||
| ≤ 306.9 |
| 0.001 |
| 0.450 |
| lymphocyte nadir | ||||
| > 0.56×109/L |
|
| ||
| ≤ 0.56×109/L |
|
|
| 0.099 |
| EDRIC | ||||
| > 5.63Gy |
|
| ||
| ≤ 5.63Gy |
|
|
|
|
| End point | Models | AUC | |
|---|---|---|---|
| Training cohort | Validation cohort | ||
| 2-year OS | Combined model | 0.802 | 0.848 |
| EDRIC-based model | 0.671 | 0.599 | |
| ALI-based model | 0.703 | 0.764 | |
| 2.5-year OS | Combined model | 0.784 | 0.789 |
| EDRIC-based model | 0.636 | 0.631 | |
| ALI-based model | 0.713 | 0.696 | |
- —National Institutes of Natural Sciences10.13039/501100006321
- —Natural Science Foundation of Shandong Province10.13039/501100007129
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Lung Cancer Diagnosis and Treatment · Inflammatory Biomarkers in Disease Prognosis
Introduction
1
Lung cancer is the most common malignancy worldwide, with non-small cell lung cancer (NSCLC) representing the predominant histological subtype (1). Because early-stage NSCLC is often asymptomatic, most patients are diagnosed at an advanced stage with poor prognosis. With the advent of immunotherapy (IT), immune checkpoint inhibitors combined with chemotherapy have become a standard first-line treatment for advanced NSCLC (2, 3). Based on findings from the PEMBRO-RT and MDACC trials, administering concurrent or sequential thoracic radiotherapy (RT) may provide potential therapeutic benefit for patients with metastatic NSCLC (4–6).
RT can potentiate the effects of IT by inducing tumor cell apoptosis and releasing tumor-associated antigens, thereby activating antitumor immune responses. However, RT also exerts immunosuppressive effects, particularly through lymphocyte depletion (7, 8). Radiation-induced lymphocytopenia (RIL) is a recognized adverse prognostic factor in multiple solid tumors (9). Thus, quantifying the immune effects of RT is of critical importance.
Jin et al. (10) and Ladbury et al. (11) proposed and refined the estimated dose of radiation to immune cells (EDRIC), defined as the sum of equivalent uniform doses (EUD) to several organs, accounting for factors such as heart, lung, and whole-body mean dose, as well as the number of RT fractions. A retrospective study by Yu et al. (12) demonstrated that EDRIC was significantly correlated with lymphocyte depletion and served as an independent predictor of overall survival (OS) and progression-free survival (PFS) in patients with limited-stage SCLC. However, in this population, the standalone EDRIC model yielded only modest predictive performance, with a C-index of 0.617 for OS. In locally advanced NSCLC, the predictive ability of EDRIC for RIL was similarly limited, with an AUC of 0.596 (13). To improve prognostic accuracy, efforts have been made to integrate EDRIC with additional clinical indicators to develop multiparametric models.
Inflammation is a hallmark of cancer, contributing to tumor initiation, progression, and metastasis (14, 15), and is also influenced by RT and chemotherapy (16, 17). Circulating neutrophil, lymphocyte, and platelet counts reflect systemic immune-inflammatory status (18). Peripheral blood markers such as neutrophil-to-lymphocyte ratio (NLR) (19) and platelet-to-lymphocyte ratio (PLR) (20) are well-established prognostic factors in lung cancer. The Advanced Lung Cancer Inflammation Index (ALI), a composite index integrating inflammation and nutritional status, is calculated as BMI × (albumin/NLR). Several studies have demonstrated its prognostic value, with lower ALI levels associated with poor outcomes in lung cancer patients (21–24). Other biomarkers, including the systemic immune-inflammation index (SII) (25), lymphocyte-to-monocyte ratio (LMR) (26), and nutrition-based indicators such as the prognostic nutritional index (PNI) (27), have also been reported as predictors of adverse outcomes.
This study investigated the prognostic value of EDRIC and a range of inflammation- and nutrition-based indices (NLR, LMR, PLR, SII, ALI, and PNI) for OS and PFS in stage IV NSCLC patients treated with IT and RT. Furthermore, we evaluated their performance individually and in combination, aiming to develop a more accurate prognostic model for this patient population.
Materials and methods
2
Patients
2.1
This retrospective study included patients who received at least four cycles of first-line IT and thoracic RT at three centers between 2020 and 2023. Owing to the retrospective design, the requirement for informed consent was waived. A total of 167 patients with available dose measurement data were identified. Among them, 126 patients from Shandong Cancer Hospital were used as the training cohort and validation cohort, in which the prognostic model was developed and internally validated. The remaining 41 patients from Anhui Provincial Cancer Hospital and Anhui Provincial Hospital comprised an independent external validation cohort. The inclusion criteria were as follows: (1) age ≥18 years; (2) histologically confirmed NSCLC (including adenocarcinoma, squamous cell carcinoma, and large cell carcinoma); (3) clinical stage IV disease according to the AJCC TNM staging system, 8th edition; and (4) at least three complete blood counts (CBCs) obtained during thoracic RT. The exclusion criteria were: (1) prior targeted therapy for specific gene mutations (e.g., EGFR, ALK); (2) absence of detailed RT and dose measurement data; (3) active infection or ongoing corticosteroid therapy at the time of CBC assessment; and (4) concurrent or prior malignancies. This study was approved by the Ethics Committee of Shandong Cancer Hospital and Institute (ethics approval number: SDTHEC2022009020) and was conducted in accordance with the Declaration of Helsinki.
Data collection and EDRIC calculation
2.2
Patient data were collected by reviewing electronic medical records, including sex, age, height, weight, comorbidities (e.g., hypertension, diabetes), initial tumor pathology and stage, prior treatment history, and dates of diagnosis and disease progression. Baseline laboratory data obtained within two weeks prior to IT included serum albumin, neutrophil, platelet, lymphocyte, and monocyte counts. These values were used to calculate NLR, PLR, LMR, SII, ALI, and PNI. The EDRIC was calculated according to the methods developed by Jin et al. (10) and further refined by Ladbury et al. (11). Relevant parameters, including mean lung dose (MLD), mean heart dose (MHD), mean body dose (MBD), number of fractions, gross tumor volume (GTV), and planning target volume (PTV), were extracted from each patient’s RT treatment plan. The calculation was performed using the following formula:
Statistical analysis
2.3
The primary endpoint of this study was OS, and PFS was defined as a secondary endpoint. OS was calculated from the date of diagnosis to death from any cause or the last follow-up. PFS was defined as the interval from diagnosis to local progression or death from any cause. Optimal cutoff values for each parameter were determined using ROC curve analysis. Spearman’s rank correlation was applied to evaluate associations between EDRIC and other variables. Kaplan-Meier methods were used to estimate OS and PFS, with comparisons made using log-rank tests. Cox proportional hazards models were employed for univariate and multivariate analyses to identify factors associated with OS and PFS and to determine independent prognostic indicators. Patients were randomly assigned into a training and validation cohort at a 2:1 ratio based on independent predictors. Nomogram models predicting OS using EDRIC, ALI, and combined EDRIC-lymphocyte nadir-ALI were constructed in R software (version 4.4.2). Model performance was compared using ROC curve analysis. All statistical analyses were performed using SPSS software (version 27.0), and a p-value<0.05 was considered statistically significant.
Results
3
Baseline patient characteristics
3.1
This study included 126 patients with advanced NSCLC. The median age was 64 years (range, 36–79 years), and the cohort comprised 96 males (76.2%) and 30 females (23.8%). A history of smoking was reported in 72 patients (57.1%), and 51 patients (40.5%) had a history of alcohol consumption. Clinical staging showed that 61 patients (48.4%) were at stage IVA and 65 patients (51.6%) at stage IVB. The median follow-up was 35.5 months (range, 11.6-62.1 months). During follow-up, 57 patients (45.2%) died, and 79 patients (62.7%) experienced disease progression. The median EDRIC was 4.76 Gy (range, 0.89-12.12 Gy), and the median lymphocyte nadir during radiotherapy was 0.52 × 10^9^/L (range, 0.1-2.1 × 10^9^/L) (Table 1). We compared the baseline characteristics across the training, validation, and external validation cohorts, as shown in Supplementary Table S1. Details of the patients’ radiotherapy, including treatment intent, thoracic dose, fractionation, and doses to critical organs, are provided in Supplementary Table S2.
Factors affecting prognosis
3.2
ROC curves were plotted using patient survival as the state variable, and optimal cutoff values for each parameter were determined by the maximum Youden index: EDRIC = 5.63 Gy; lymphocyte nadir = 0.56 × 10^9^/L; NLR = 2.79; PLR = 143.8; LMR = 2.07; SII = 844; ALI = 306.9; PNI = 49.7. In univariate Cox regression for NSCLC, NLR, PLR, SII, LMR, ALI, lymphocyte nadir, and EDRIC were associated with OS. In multivariate analysis, ALI ≤306.9 (HR 2.64, 95% CI 1.01-6.92, P = 0.048), lymphocyte nadir ≤0.56 × 10^9^/L (HR 2.20, 95% CI 1.19-4.06, P = 0.012), and EDRIC ≤5.63 Gy (HR 0.52, 95% CI 0.29-0.91, P = 0.022) were independent prognostic factors for OS (Table 2). Univariate analysis also showed significant associations of NLR, PLR, SII, ALI, lymphocyte nadir, and EDRIC with PFS. Multivariate analysis identified EDRIC ≤ 5.63 Gy as an independent predictor of PFS (HR 0.50, 95% CI 0.31-0.81, P = 0.005) in NSCLC patients receiving neoadjuvant chemo-immunotherapy (Table 3).
Impact of EDRIC, lymphocyte nadir, and ALI on patient prognosis
3.3
Among 126 patients, 83 (65.9%) had EDRIC ≤5.63 Gy, whereas 43 (34.1%) had EDRIC >5.63 Gy. Kaplan-Meier analysis revealed significantly improved OS in patients with EDRIC ≤5.63 Gy compared with those with EDRIC >5.63 Gy. The 12-, 24-, and 36-month OS rates were 92.8%, 66.3%, and 26.5% for patients with EDRIC ≤5.63 Gy, versus 88.4%, 37.2%, and 14.0% for those with EDRIC >5.63 Gy, respectively (Figure 1A).
Kaplan-Meier survival curves in patients with stage IV NSCLC who received consolidative thoracic RT following first-line chemoimmunotherapy: (A) OS comparing the EDRIC >5.63 Gy and EDRIC ≤ 5.63 Gy groups; (B) OS comparing the lymphocyte nadir ≤ 0.56×109/L and lymphocyte nadir >0.56×109/L groups; (C) OS comparing the ALI ≤ 306.9 and ALI >306.9 groups; (D) PFS comparing the EDRIC >5.63 Gy and EDRIC ≤ 5.63 Gy groups. NSCLC, non-small cell lung cancer; RT, radiotherapy; OS, overall survival; EDRIC, estimated dose of radiation to immune cells; Gy, Gray; ALI, advanced lung cancer inflammation index; PFS, progression-free survival; HR, hazard ratio; CI, confidence interval.
Patients with a lymphocyte nadir >0.56 × 10^9^/L exhibited significantly prolonged OS compared with those with ≤ 0.56 × 10^9^/L. The 12-, 24-, and 36-month OS rates were 100%, 76.4%, and 30.9% versus 84.5%, 40.8%, and 15.5%, respectively (Figure 1B). Similarly, patients with ALI >306.9 demonstrated significantly better OS compared with those with ALI ≤306.9. The 12-, 24-, and 36-month OS rates were 95.7%, 77.1%, and 27.1% versus 85.7%, 30.4%, and 16.1%, respectively (Figure 1C). Consistent with the OS findings, patients with EDRIC ≤5.63 Gy had significantly improved PFS compared with those with EDRIC >5.63 Gy. The 12-, 24-, and 36-month PFS rates were 84.3%, 53.0%, and 19.3% versus 70.1%, 23.3%, and 11.6%, respectively (Figure 1D). We also generated Kaplan–Meier curves for PFS based on lymphocyte nadir (Supplementary Figure S1A) and ALI (Supplementary Figure S1B).
Spearman’s rank correlation analysis demonstrated positive correlations between EDRIC and GTV (r = 0.3564, P< 0.001; Figure 2A), PTV (r = 0.6012, P< 0.001; Figure 2B), and N stage (r = 0.2592, P = 0.0034; Figure 2C). In contrast, EDRIC was negatively correlated with lymphocyte nadir (r = -0.3776, P< 0.001; Figure 2D).
Spearman’s correlation coefficients for (A) GTV and EDRIC; (B) PTV and EDRIC; (C) N-stage and EDRIC; (D) Lymphocyte nadir and EDRIC. GTV, gross tumor volume; PTV, planning target volume; EDRIC, estimated dose of radiation to immune cells; HR, hazard ratio; CI, confidence interval; Gy, Gray;.
Comparison of nomogram prognostic models
3.4
The training cohort comprised 84 patients, while the validation cohort included 42 patients. No significant differences were observed across clinical variables between groups. The predictive performance of three nomogram models, namely EDRIC (Figure 3A), ALI (Figure 3B), and the combined EDRIC, lymphocyte nadir, and ALI model (Figure 3C), was evaluated, with the results summarized in Table 4. The calibration curve of the combined model closely aligned with the ideal reference line (Figure 3C).
(A) EDRIC-based model and ROC curves for predicting OS in NSCLC patients receiving neoadjuvant chemoimmunotherapy. (B) ALI-based model and ROC curves for predicting OS. (C) Combined model and ROC curves for predicting OS, along with the calibration curve of the combined model. EDRIC, estimated dose of radiation to immune cells; ROC, receiver operating characteristic; OS, overall survival; NSCLC, non-small cell lung cancer; ALI, advanced lung cancer inflammation index.
Comparison of the area under the ROC curve (AUC) demonstrated that the combined model significantly outperformed the single-parameter EDRIC- and ALI-based models in predicting 2-year OS. Similar results were observed for 2.5-year OS prediction (Table 4).
The combined model was further validated in an independent external cohort of 41 patients, including 26 (63.4%) with squamous cell carcinoma and 15 (36.6%) with adenocarcinoma. Within this cohort, 24 (58.5%) patients had EDRIC ≤5.63 Gy, and 19 (46.3%) had ALI >306.9. The combined model again demonstrated superior predictive ability for both 2-year and 2.5-year OS compared with the single-factor models (Figure 4).
Combined model and ROC curves for predicting OS, along with the calibration curve of the combined model in the external validation cohort. ROC, receiver operating characteristic; OS, overall survival.
Taken together, the nomogram based on EDRIC and ALI provided excellent discrimination and calibration, supporting its clinical utility in predicting survival outcomes in stage IV NSCLC patients receiving IT combined with RT.
Discussion
4
Based on findings from the PEMBRO-RT (4) and MDACC (5) trials, combining RT with IT has shown potential efficacy for patients with metastatic NSCLC. To our knowledge, this study is the first to investigate the prognostic value of integrating EDRIC with nutritional and inflammatory parameters in this population. Our results demonstrate that lower EDRIC scores are associated with significantly improved survival outcomes, both in terms of PFS and OS. Moreover, low baseline ALI and reduced lymphocyte nadir levels emerged as independent prognostic factors for inferior OS. While prognostic models constructed from single indicators displayed limited accuracy, the integration of EDRIC, baseline ALI, and lymphocyte nadir into a multidimensional model markedly enhanced predictive performance. This approach provides clinicians with more robust decision-making support and may facilitate the optimization of individualized treatment strategies.
In a secondary analysis of RTOG 0617, Jin et al. first proposed a model estimating the radiation dose delivered to the immune system. Following the establishment of the EDRIC model, subsequent studies confirmed that elevated EDRIC values were associated with poorer OS and PFS in stage III NSCLC (27). These findings suggest that optimizing treatment planning to minimize EDRIC could improve prognosis. Similarly, a retrospective study by Yin et al. (28) identified EDRIC as an independent prognostic factor for locally advanced NSCLC, with its impact closely correlated with GTV and N staging—results consistent with the present study. Likewise, Yang et al. (13) reported that higher EDRIC levels predicted worse OS and PFS in stage III NSCLC patients, underscoring its potential role as a biomarker for consolidation immunotherapy. These findings align closely with our results.
We also extended the analysis to the prognostic significance of ALI. A high baseline ALI was associated with longer OS, consistent with prior reports by Jafri and Mandaliya et al. (21, 29). Taken together, these findings suggest that the combined model of EDRIC, ALI, and lymphocyte nadir provides a biologically plausible and clinically useful tool for survival prediction in stage IV NSCLC.
The superior performance of the combined model may be explained by the synergistic biological effects of its components. First, lymphocytes are highly radiosensitive, with doses as low as 1 Gy substantially reducing cell survival (30, 31). Previous studies have confirmed correlations between EDRIC and peripheral lymphocyte depletion (12, 32). Since CD4+ and CD8+ T lymphocytes are critical for cytotoxic antitumor immune responses, their depletion may compromise immune surveillance and promote tumor proliferation, invasion, and metastasis (33). Second, ALI captures the interplay between systemic inflammation and nutritional status, where reduced neutrophil levels may diminish secretion of pro-angiogenic, growth, and anti-apoptotic factors, thereby limiting tumor progression (34).
Importantly, all three parameters—EDRIC, ALI, and lymphocyte nadir—are clinically simple, cost-effective, and readily available in routine practice. Once their prognostic significance is further validated, these markers could be widely implemented by oncologists worldwide, supporting clinical translation.
Nevertheless, this study has limitations. First, as a retrospective analysis, it is subject to potential selection bias and uncontrolled confounding factors. Second, EDRIC, while a promising prognostic marker, has several limitations that should be considered. It may be influenced by variations in radiotherapy planning, including target volume delineation, radiation field configuration, and dose constraints, which can differ across institutions and lead to variability in the estimated immune cell dose exposure. The EDRIC model is based on simplified assumptions and does not incorporate specific dose distributions to immune substructures such as lymph nodes or major vessels. Furthermore, although EDRIC quantifies radiation exposure to circulating immune cells, it does not capture a patient’s intrinsic immune resilience or capacity to recover from lymphocyte depletion, which may explain why combining EDRIC with host-related immune parameters (e.g., ALI or lymphocyte nadir) enhances prognostic performance. Finally, the relatively small sample size underscores the need for large-scale, multicenter, prospective trials to validate the prognostic value of EDRIC and ALI in stage IV NSCLC patients undergoing first-line immunotherapy.
Conclusions
5
In the era of immunotherapy, EDRIC, lymphocyte nadir, and ALI serve as independent predictors of OS in patients with stage IV NSCLC, while EDRIC alone is an independent predictor of PFS. Notably, combining EDRIC with ALI further enhances prognostic accuracy, providing a more reliable tool for outcome prediction.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A . Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660, PMID: 33538338 · doi ↗ · pubmed ↗
- 2Gandhi L Rodríguez-Abreu D Gadgeel S Esteban E Felip E De Angelis F . Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. (2018) 378:2078–92. doi: 10.1056/NEJ Moa 1801005, PMID: 29658856 · doi ↗ · pubmed ↗
- 3Paz-Ares L Luft A Vicente D Tafreshi A GümüşM Mazières J . Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N Engl J Med. (2018) 379:2040–51. doi: 10.1056/NEJ Moa 1810865, PMID: 30280635 · doi ↗ · pubmed ↗
- 4Theelen WSME Peulen HMU Lalezari F van der Noort V de Vries JF Aerts JGJV . Effect of pembrolizumab after stereotactic body radiotherapy vs pembrolizumab alone on tumor response in patients with advanced non-small cell lung cancer: results of the PEMBRO-RT phase 2 randomized clinical trial. JAMA Oncol. (2019) 5:1276–82. doi: 10.1001/jamaoncol.2019.1478, PMID: 31294749 PMC 6624814 · doi ↗ · pubmed ↗
- 5Welsh J Menon H Chen D Verma V Tang C Altan M . Pembrolizumab with or without radiation therapy for metastatic non-small cell lung cancer: a randomized phase I/II trial. J Immunother Cancer. (2020) 8:e 001001. doi: 10.1136/jitc-2020-001001, PMID: 33051340 PMC 7555111 · doi ↗ · pubmed ↗
- 6Theelen WSME Chen D Verma V Hobbs BP Peulen HMU Aerts JGJV . Pembrolizumab with or without radiotherapy for metastatic non-small-cell lung cancer: a pooled analysis of two randomised trials. Lancet Respir Med. (2021) 9:467–75. doi: 10.1016/S 2213-2600(20)30391-X Erratum in: Lancet Respir Med. (2021) 9(3):e 29. doi: 10.1016/S 2213-2600(21)00012-6, PMID: 33096027 · doi ↗ · pubmed ↗
- 7Shang S Liu J Verma V Wu M Welsh J Yu J . Combined treatment of non-small cell lung cancer using radiotherapy and immunotherapy: challenges and updates. Cancer Commun (Lond). (2021) 41:1086–99. doi: 10.1002/cac 2.12226, PMID: 34658186 PMC 8626591 · doi ↗ · pubmed ↗
- 8Zhai D An D Wan C Yang K . Radiotherapy: Brightness and darkness in the era of immunotherapy. Transl Oncol. (2022) 19:101366. doi: 10.1016/j.tranon.2022.101366, PMID: 35219093 PMC 8881489 · doi ↗ · pubmed ↗