AI agents in Alzheimer’s disease management: challenges and future directions
Gerasimos Grammenos, Aristidis G. Vrahatis, Konstantinos Lazaros, Themis P. Exarchos, Panagiotis Vlamos, Marios G. Krokidis

TL;DR
AI agents could improve Alzheimer’s disease management by integrating diverse data and supporting clinical decisions, but challenges remain in their development and deployment.
Contribution
The paper introduces agentic AI as a novel approach for Alzheimer’s management through multimodal, adaptive systems.
Findings
Current AI tools for Alzheimer’s are limited by being unimodal and lacking longitudinal reasoning.
Agentic AI can integrate imaging, genomics, and behavioral data to support clinical decision-making.
Future AI systems should prioritize interpretability, collaboration with clinicians, and ethical deployment.
Abstract
Neurodegenerative diseases such as Alzheimer’s and Parkinson’s disease pose a major global healthcare challenge, with cases projected to rise sharply as populations age and effective treatments remain limited. AI has shown promise in supporting diagnostics, predicting disease progression, and exploring biomarkers, yet most current tools are narrowly focused, unimodal, and lack longitudinal reasoning or interpretability. By enabling context-aware analysis across imaging, genomics, cognitive, and behavioral data, agentic AI can track disease progression, identify therapeutic targets, and support clinical decision-making. Over time, these systems may detect gaps in their own information and request targeted data, moving closer to real clinical reasoning while keeping clinicians in control. The next frontier in medical AI lies in developing autonomous, multimodal agents capable of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
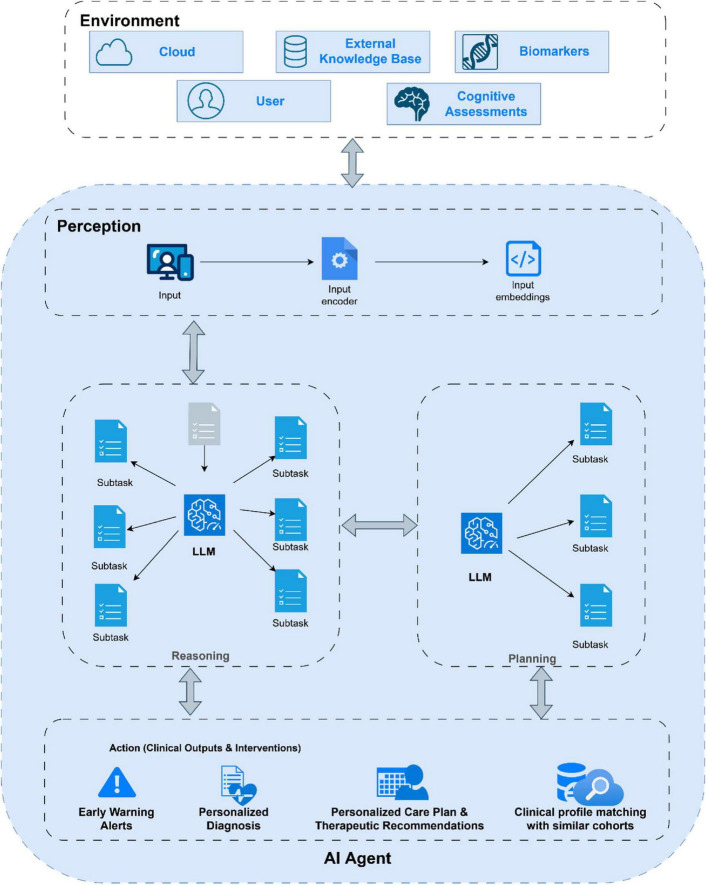 FIGURE 1
FIGURE 1| Research area | Methodology | Modality | Outcome | References |
|---|---|---|---|---|
| Diagnostic classification | Deep learning with latent space analysis | Structural MRI | Classifies sex-specific brain network changes with high precision (> 90%). |
|
| Multimodal data fusion | MRI + plasma biomarkers | Detects amyloid status with AUC 0.94 |
| |
| EEG/electrophysiological AI models | EEG recording | Identification of the EEG frequency bands decisive for AD diagnosis, balance metrics, real-time AD detection |
| |
| Disease prediction | Knowledge-graph learning | EHR | Predicts AD onset 7 years in advance (AUC 0.80). |
|
| Trajectory modeling | Longitudinal MRI + CSF (Aβ42) | Forecasts MCI-to-AD conversion within 3 years with 85% accuracy. |
| |
| Biomarker discovery | Feature selection and machine learning classifiers | Blood gene expression from ADNI, ANM1, ANM2 datasets | Classification of AD (AUC: 0.619–0.859); identification of AD-related pathways (inflammation, mitochondria, Wnt signaling) |
|
| Classical machine learning | Digital biomarkers: motor activity, neurocognitive tests, eye tracking, speech analysis | Prediction/classification of AD (AUC ∼0.887) and MCI (AUC ∼0.821); integration into clinical practice |
| |
| Mechanism exploration | GS correlation analysis; imaging-transcriptomics integration | fMRI; gene expression | Altered GS topography in AD; correlation with functional network properties and cognition |
|
| Deep transfer learning using pre-trained CNNs, ensemble modeling | MRI | Accurate AD diagnosis (up to 96% accuracy) with interpretable visual explanations highlighting key neural regions |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsArtificial Intelligence in Healthcare and Education · Machine Learning in Healthcare · Explainable Artificial Intelligence (XAI)
Introduction
Neurodegenerative diseases such as Alzheimer’s related dementias and Parkinson’s disease represent one of the greatest challenges in global healthcare. According to World Alzheimer’s Report over 55 million people live with dementia, mostly due to Alzheimer’s worldwide while this number is projected to reach 150 million people worldwide by 2050 (Alzheimer’s Disease International, 2024). As human lifespan increases, more individuals suffer cognitive decline or motor dysfunction while effective treatments and reliable early diagnostics remain limited. This growing gap between disease burden and therapeutic progress highlights the need for new ways to understand and manage these complex clinical. Artificial intelligence (AI) has shown progress in this area as a supportive tool in diagnostic classification, disease prediction, biomarker discover and disease mechanism exploration (van Oostveen and de Lange, 2021). For example, AI analysis of neuroimaging biomarkers can assist in early prediction of Alzheimer’s disease (AD) pathology (Kale et al., 2024). Table 1 presents an overview of recent AI applications in the context of AD management. This illustrates AI’s supportive role in neurodegenerative disease research, from diagnosing early symptoms to predicting which patients with mild cognitive impairment will progress to dementia (Ai et al., 2025). However, most current artificial intelligence tools in medicine remain narrowly focused, with strong performance in isolated tasks such as MRI classification or speech analysis but limited capacity to generalize well using multimodal data. Recent evidence confirms that clinical AI systems largely remain unimodal and lack mechanisms for integrating heterogeneous data or supporting longitudinal reasoning (Winchester et al., 2023; Judge et al., 2024). They operate as passive algorithms rather than active collaborators and frequently function as black boxes with limited interpretability (Rudin, 2019; Xu and Shuttleworth, 2024). Herein, we argue that the frontier in medical AI is to move beyond narrow, task-specific models toward autonomous agents that can reason across varied data sources, use multiple existing state-of-the-art tools for decision support and calculation, adapt through experience and collaborate effectively with clinicians. We specifically examine the current role of AI in AD’s care, outline key obstacles related to integration, interpretability and regulation, considering future directions for introducing these agents into clinical practice.
Clinical landscape of Alzheimer’s disease
AD is a progressive neurodegenerative disorder clinically characterized by the cognitive impairment and decline in various functional abilities. Several processes are involved into the pathophysiology of AD, i.e., abnormal extracellular deposition of amyloid-beta (Aβ) plaques, intracellular tau tangles, and volumetric loss of cortical gray matter (DeTure and Dickson, 2019). This pathophysiology is already present long before the clinical AD onset symptoms, which is known as “preclinical” AD and it can last for up to 20 years. The commonest clinical manifestation of the AD is the short-term memory deficits, while modest impairments in other cognitive domains can also be present, known as “prodromal AD” or Mild Cognitive Impairment (MCI) stage. During the disease course cognitive decline is worsening leading to dementia, a syndromic term for a decline in cognitive abilities of sufficient severity to interfere with function during daily activities.
Available pharmacological treatments provide only temporary symptomatic relief and do not alter disease course. Non-pharmacological interventions, such as cognitive training, physical activity, nutrition, and social engagement show proven benefits, but remain fragmented, non-standardized, and rarely integrated with biological or digital monitoring (Luo et al., 2023). Current care models therefore fail to deliver adaptive and personalized interventions capable of addressing the heterogeneity of AD. Traditional biomarkers (CSF assays, PET, plasma NfL) enable early diagnosis and stratification while digital biomarkers derived from wearables and smartphones offer scalable, real-time measures of cognition and behavior. Evidence from meta-analyses supports combined cognitive-behavioral strategies, which also have transdiagnostic relevance (e.g., depression, psychosis) ( Ó hAnrachtaigh et al., 2024). However, integration of digital signals into clinical workflows is minimal and combined biological–digital biomarker frameworks for guiding interventions are lacking. Recent advances in AI provide new opportunities to link multimodal biomarkers with clinical outcomes, but these remain at early research stages and are not embedded in routine dementia care (Jasodanand et al., 2025).
The growing importance of agentic AI
Agentic AI (artificial intelligence), refers to intelligent systems capable of acting autonomously, perceiving their surroundings, reasoning about what they observe, and making decisions to achieve specific objectives. Unlike conventional software that follows fixed instructions, agentic systems are designed to learn from experience, plan their actions, and adapt dynamically as conditions change. They combine perception, reasoning, memory and action into a coherent whole, allowing them to operate with a level of independence that brings machines closer to genuine collaboration with humans. This development marks a significant step in artificial intelligence, as systems evolve from static automation to entities capable of purposeful and context-aware behavior (Huang, 2025).
The growing importance of agentic AI stems from its capacity to address environments that are complex, uncertain, and data-intensive. This makes it particularly relevant in scientific and medical domains where dynamic systems must be understood and interpreted across multiple layers of biological, clinical, and behavioral information. In the study of neurodegenerative diseases such as Alzheimer’s disease, where disease mechanisms unfold gradually and vary across individuals, agentic systems hold the potential to synthesize vast datasets and extract patterns that evolve over time (Cheng et al., 2024). Their ability to integrate molecular findings, imaging data and cognitive assessments could eventually support the construction of adaptive models capable of anticipating disease progression or identifying subtle early indicators of decline, as Figure 1 depicts. Through this adaptive reasoning, agentic AI offers a conceptual pathway toward a more comprehensive understanding of complex neurobiological processes (Breithaupt et al., 2025).
Conceptual framework of an AI agent in Alzheimer’s disease. The agent interacts with environmental data including biomarkers and cognitive assessments through a continuous perception, reasoning, planning, and action cycle. Inputs are encoded into embeddings and processed by large language models to decompose complex tasks. The action layer executes clinical outputs such as early warning alerts, personalized diagnoses, therapeutic recommendations, and clinical profile matching.
AI agents can be organized into several main categories depending on their internal architecture and level of autonomy. Reactive agents represent the simplest form, responding directly to stimuli from their environment without storing or reasoning about past experiences. Their lack of memory makes them well-suited for tasks that require immediate reaction or repetitive evaluation of changing conditions (Sapkota et al., 2025). Deliberative agents operate at a higher level, maintaining internal representations of their environment and planning future actions based on predicted outcomes. They reason about alternative possibilities before deciding on a course of action, a feature that makes them potentially useful for modeling long-term biological processes such as disease progression. In neurodegenerative research, such agents can be used to simulate how cellular, molecular, and behavioral factors interact over time, supporting hypothesis generation in studies of brain aging or dementia. Hybrid agents combine both reactive and deliberative mechanisms, enabling immediate responsiveness while retaining strategic, long-term reasoning capabilities (Lanham, 2025). Their architecture allows them to balance real-time data interpretation with broader analytical goals. This flexibility can be valuable in longitudinal biomedical studies, where systems must adapt to new data while maintaining continuity with prior analyses.
Functional distinctions can be identified between goal-based and utility-based agents (Matsumoto et al., 2006). Goal-based agents operate based on predefined objectives, continuously adjusting their decisions to achieve those targets. They are particularly useful in data-driven research pipelines aimed at optimizing model performance or enhancing predictive accuracy. Utility-based agents build upon this principle by evaluating the relative worth of possible outcomes and selecting actions that maximize overall benefit according to specified evaluation criteria. These agents are especially valuable in research settings that demand trade-offs among sensitivity, specificity and interpretability, for example, distinguishing between early and late stages of Alzheimer’s pathology. Learning agents constitute another important category, characterized by their ability to improve through feedback (Axelsson et al., 2022). They refine their decision-making processes as they accumulate experience, which makes them especially relevant in settings where the underlying system evolves or where the available data grow over time. Reinforcement learning, a key approach within this category, enables agents to learn optimal behaviors through iterative exploration and evaluation (Wang F. et al., 2025). Although its full application to neurodegenerative disease research is still emerging, such adaptive learning methods could one day contribute to refining diagnostic models or identifying new therapeutic targets by continuously updating their reasoning as new evidence appears. Finally, multi-agent systems bring together several autonomous entities that cooperate or coordinate to achieve shared objectives (Rother et al., 2025). They can divide complex analytical problems into smaller, specialized tasks and communicate to form a collective intelligence greater than the sum of its parts. While their integration into neuroscience and biomedical research remains largely conceptual, such systems hold promise for managing large-scale datasets that span molecular, imaging, and clinical dimensions, potentially enabling collaborative reasoning across interconnected models.
The expanding development of these various forms of agents illustrates the flexibility and depth of the agentic AI paradigm. While their current use in neurodegenerative research is still in exploratory stages, their theoretical capabilities align closely with the needs of the field (Perry et al., 2024). They offer frameworks for continuous learning, adaptive reasoning, and distributed analysis; qualities that mirror the progressive and multifactorial nature of disorders such as Alzheimer’s disease. As these technologies evolve, the main challenge will be to translate their conceptual promise into practical, transparent, and interpretable tools that can operate responsibly within scientific and clinical research.
From classical AI tools to AI agents in neurogenerative care
Current AI applications in neurodegenerative disease diagnosis remain narrow, single-task, unimodal systems that function as sophisticated classifiers rather than reasoning applications. These systems showcase narrow intelligence with the application of high-level processing to single, constrained clinical tasks without capacity for generalization or multi-step reasoning (Adler-Milstein et al., 2022). Most models operate on unimodal data performing analysis on neuroimaging biomarkers or conducting clinical assessments in isolation (Shokrpour et al., 2025). While deep learning achieves accuracy greater than 80% on specific classification tasks (Venugopalan et al., 2021), these systems exhibit performance degradation when encountering incomplete data or context-based scenarios that was not part of the training set. Furthermore, no current AI system continually receives feedback about diagnostic performance, limiting capacity for clinical learning and adaption (Ahmed et al., 2023).
AI agents can change this entirely. Unlike traditional machine and deep learning methodologies that map input to output, AI agents execute goal-directed behavior that break high-level complex objectives into smaller subtasks while maintaining probabilistic decision-making. Recent works demonstrate this shift. Google presented the AIME system that uses state-aware reasoning through diagnostic phases that outperforms clinicians in 29 out of 32 evaluations (Saab et al., 2025). MedAgent-Pro introduced hierarchical workflows with disease-level planning and patient-level reasoning (Wang Z. et al., 2025). For neurodegenerative disease, agents can provide guidance that’s impossible to achieve with narrow tools. Instead of producing a simple classification label, an agent can follow a multi-step reasoning process. It may analyze atrophy patterns on MRI, interpret cerebrospinal fluid biomarker ratios, retrieve information from electronic health records about genetic risk factors, and assess the patient’s cognitive trajectory over time. It can also review current diagnostic criteria, generate a probabilistic differential diagnosis, and suggest confirmatory assessments when uncertainty remains high. A 2024 Nature Medicine study involving more than fifty-one thousand participants showed that a multimodal model reached an AUROC of 0.96 in distinguishing ten dementia types, outperforming neurologist-only assessment by more than twenty-six percent (Xue et al., 2024). Yet, even this remains a static classifier. Agentic systems build upon such models with introducing dynamic reasoning which allows them to request additional context for the data provided when confidence drops and track longitudinal disease trajectories to improve understanding over time. Foundation models such as ChatGPT, Claude and even more clinical focused like Med-PaLM2 now provide the intelligence needed for these systems to achieve expert-level performance across a wide range of medical tasks (Singhal et al., 2023, 2025). Evidence from a review of more than four hundred studies shows that multimodal approaches consistently outperform single-modality models by about six percentage points in AUC (Schouten et al., 2025). Agentic architectures could convert those performance gains into real clinical value through the integration of reasoning, memory, and adaptive decision processes that reflect human diagnostic thought.
Challenges in development and clinical deployment
Recent works in explainable AI in medicine found that the principal barrier to clinical adoption is the black box nature of deep learning models. The authors emphasized that when the reasoning process of a model is not transparent, clinicians are less to rely on its output, particularly in contexts where decisions carry important medical and legal consequences (Muhammad and Bendechache, 2024; Houssein et al., 2025). Clinicians do not need to follow each computational step, but they do require clear and well-grounded explanations that align with accepted medical reasoning and professional accountability. An effective AI agent would present its diagnostic recommendations with narrative justifications that reference key clinical features, supporting evidence, and plausible alternative interpretations. Advances in foundation models now make this possible with enabling the generation of detailed clinical rationales, probabilistic differential diagnoses, and evidence-based references. A systematic review on explainability in clinical AI found that the ethical requirement for transparency depends strongly on context, with low risk screening able to tolerate opaque accuracy, while high risk interventions demand comprehensive and interpretable justification (Blackman and Veerapen, 2025). Holding AI systems to the same standard of explainability expected from human reasoning, rather than to an unattainable level of mathematical clarity, would create a more practical balance between transparency and clinical utility.
Another major challenge in the clinical deployment of AI agents lies in understanding how humans collaborate with these systems and how trust in their outputs is calibrated to effectively support clinical judgment. Experimental evidence in disease diagnostics shows that the introduction of AI support can create a false conflict error, a situation in which clinicians replace correct judgments with incorrect algorithmic outputs (Rosenbacke et al., 2024). Under controlled experimental conditions, physicians demonstrating high baseline diagnostic accuracy exhibited significant performance degradation following the introduction of AI assistance. Specifically, diagnostic accuracy declined from approximately 87% to 77% upon exposure to model-generated recommendations. This decline occurred because clinicians deferred to the system’s suggestions even when their original assessment had been correct. In contrast, clinicians with lower baseline accuracy improved, suggesting that algorithmic guidance can compensate for limited expertise while potentially undermining expert clinical reasoning when over trusted. These findings suggest that the interaction between human expertise and AI recommendations depends not only on model performance but also on the clinician’s perception of the system’s trustworthiness. Overconfidence in algorithmic predictions can lead to errors that would otherwise not occur, whereas excessive skepticism can neutralize potential benefits. This phenomenon, known as trust miscalibration, underscores the importance of designing AI systems that communicate uncertainty, reliability, and contextual limitations. In AD research, similar issues have been observed during the integration of AI models trained on MRI, PET, and multimodal biomarker data, where clinicians may either overestimate model reliability or dismiss valid insights due to insufficient interpretability and lack of transparent reasoning (Mirkin and Albensi, 2023).
Transition toward agentic tools in clinical practice and future insights
The most practical way to introduce agentic AI systems into healthcare is through targeted augmentation of existing clinical bottlenecks rather than attempting a full-scale transformation of clinical workflows. Applications such as cognitive assessment agents, neuroimaging triage systems, and medication optimization tools represent feasible near-term implementations, it remains unclear whether these narrowly focused deployments will demonstrate sufficient clinical and operational value to justify widespread adoption. Automated screening, for instance, could in theory help reduce clinic wait times, which often exceed six months (Mattke and Hanson, 2024) and even stretch to twelve months (Lam and Mattke, 2021), but its true impact depends on whether such an application genuinely improves patient outcomes or merely redistributes diagnostic delays. In many cases, the limiting factor is not algorithmic performance but the healthcare system’s capacity to respond to an increased number of patients identified for expedited assessment. The main advantage of these domain-specific systems lies in their inherently safe failure modes. Errors in cognitive scoring can be detected through clinician review, prioritization mistakes in imaging typically cause diagnostic delays rather than missed diagnoses, and medication optimization recommendations still require human approval before clinical implementation (Connor et al., 2018). Systems designed primarily for safety and oversight may remain confined to supportive roles and never achieve the degree of autonomy required for substantial improvements in clinical efficiency or systemic scalability.
Coordinated multi agent diagnostic systems that divide the diagnostic process into specialized components such as clinical intake, biomarker integration, literature synthesis, differential diagnosis and treatment recommendation are a promising direction for clinical artificial intelligence (Borkowski and Ben-Ari, 2025). The modularity principle is appealing, as it allows individual components to be updated with advances in medical knowledge and computational methods without rebuilding the entire system. Yet the same flexibility introduces coordination challenges and raises conceptual doubts about whether clinical reasoning can truly be divided into discrete computational stages. In reality, diagnostic reasoning is iterative: clinicians continuously adjust hypotheses as new information and context interact (Olson et al., 2024). Rigidly partitioning subtasks in multi-agent architectures may therefore distort the natural flow of diagnostic thought.
A future step between current diagnostic agents and more autonomous systems may involve integrating aspects that mimic the concept of active inference. Current clinical AI models still operate as passive classifiers that rely on static, pre collected inputs, which limits their ability to emulate the nature of clinical decision making. Future agentic systems should be able to estimate their own uncertainty and determine which additional data would reduce diagnostic uncertainty (Gao et al., 2024). This could involve suggesting a targeted cognitive task, prompting the patient for a specific examination or requesting more data regarding their clinical history. Such targeted information gathering is similar to how clinicians ask specific questions to clarify uncertainty during diagnosis. These systems will still require a human in the loop framework to ensure that any AI initiated data request remains clinically appropriate, feasible and ethically acceptable (Moreno-Sánchez et al., 2026). However, to achieve this level of agentic decision making requires a change in how foundational language models which function as the “brain” of these agents are trained. Current models optimize next token prediction rather than truthfulness or calibration, limiting their ability to identify when their own knowledge is insufficient. Incorporating active inference aspects will likely require training objectives that explicitly model uncertainty to allow the agent to distinguish between medical ambiguity and uncertainty arising from missing information. Without such reasoning, the system cannot reliably decide when it should stop, request additional data, or escalate to clinician oversight.
The emerging paradigm of longitudinal care agents, which continuously synthesize data from wearable sensors, cognitive evaluations, patient-reported outcomes, and administrative health records, marks a transformative yet uncertain frontier in clinical artificial intelligence. These agents could, in theory, detect minimal signs of cognitive or functional decline months before conventional diagnostic thresholds are reached (AlHarkan et al., 2024). They could anticipate clinical inflection points, warn for early interventions, identify candidates for clinical trials, and potentially slow disease progression. However, this faces non-technical challenges that can potentially be more restrictive than the limitations of current algorithms. Continuous AI-driven monitoring depends on infrastructure that in most cases does not yet exist. It requires standardized data exchange protocols across health networks and regulatory frameworks that can guarantee patient autonomy while at the same time allow for algorithmic observation and development and deployment of models that prioritize preventive over reactive care. The assumption that earlier detection will result in better outcomes also warrants careful examination. In neurodegenerative diseases, where disease-modifying therapies remain limited (Yiannopoulou and Papageorgiou, 2020), identifying decline months earlier may contribute primarily prognostic information without offering a meaningful therapeutic benefit. Early detection without effective interventions may cause emotional distress and diminish quality of life, factors not captured by quantitative metrics but crucial for assessing the true value of continuous AI monitoring (Lee et al., 2014; Felekoğlu et al., 2021). Such systems also pose unique risks: longitudinal agents must remain calibrated as patients age and conditions change. Unlike episodic diagnostic tools, continuously running agents can gradually drift from accuracy, with errors accumulating unnoticed. Ensuring long-term oversight and recalibration is therefore essential, yet remains an unresolved challenge for safe deployment.
As the field advances, several foundational questions warrant continued deliberation. Should AI agents aim for superhuman performance based on non-human reasoning, or should validation prioritize interpretable models aligned with human cognition? Current evaluation standards assume equivalence with expert performance, yet human experts exhibit systematic biases, anchoring on initial impressions (Ly et al., 2023), overemphasizing recent salient cases, and neglecting base rates (Saposnik et al., 2016). Agents free from these cognitive constraints might achieve superior outcomes through reasoning patterns that diverge from human approaches. The question becomes whether we accept agents outperforming humans through non-human reasoning and recognize that the goal is improved patient outcomes rather than replicating human thought processes. What performance threshold justifies transitioning agents from advisory to autonomous roles? Human physicians maintain autonomous authority despite diagnostic error rates of 10%–15% (Graber, 2013). Applying higher standards to AI than humans could result in status quo biases while delaying patient access to superior diagnostic tools. Risk-stratified governance distinguishing advisory recommendations with mandatory human confirmation from default-accept recommendations with override capability to autonomous actions with retrospective review enables proportionate oversight matching autonomy levels to clinical risk.
Agentic AI systems hold genuine potential to address critical limitations in neurodegenerative disease diagnosis through integrating multimodal data, maintaining longitudinal surveillance, and reducing clinician cognitive burden. However, the transition from current narrow AI tools to clinically deployable autonomous systems is far from straightforward. It involves navigating unresolved technical limitations, regulatory uncertainty, difficulties in workflow integration, and fundamental questions concerning the appropriate scope of algorithmic participation in medical decision-making (Hosseini and Seilani, 2025). A balanced approach grounded in cautious optimism is therefore warranted. Rather than assuming inevitable transformation, progress should emphasize implementation that produces real-world evidence, systematic monitoring of failure modes, and adaptive regulatory frameworks that both enable innovation and protect patient safety.
Conclusion
Agentic AI represents a new phase of intelligent systems, characterized by reasoning, adaptability, and purposeful action. Although its application in neurodegenerative research is still early, its theoretical capabilities align closely with the needs of Alzheimer’s disease research. By enabling dynamic, context-aware analysis across imaging, genomics, cognitive, and behavioral data, agentic AI offers unprecedented potential to track disease progression and identify therapeutic targets. As a future perspective, these agents may gradually move beyond passive analysis toward models that can detect when their own information is incomplete and initiate targeted data requests to reduce uncertainty. This shift would push agentic systems closer to real clinical reasoning while still keeping clinicians in control. Ensuring ethical and patient centered deployment through close collaboration between technical and clinical teams remains essential, shifting the focus from whether AI will reshape care to how it can meaningfully support clinical expertise and patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adler-Milstein J. Aggarwal N. Ahmed M. Castner J. Evans B. J. Gonzalez A. A. (2022). Meeting the moment: addressing barriers and facilitating clinical adoption of artificial intelligence in medical diagnosis. NAM Perspect 2022:10.31478/202209 c. 10.31478/202209 c. 36713769 PMC 9875857 · doi ↗ · pubmed ↗
- 2Agostinho D. Simões M. Castelo-Branco M. (2024). Predicting conversion from mild cognitive impairment to Alzheimer’s disease: a multimodal approach. Brain Commun. 6:fcae 208. 10.1093/braincomms/fcae 208 38961871 PMC 11220508 · doi ↗ · pubmed ↗
- 3Ahmed M. I. Spooner B. Isherwood J. Lane M. Orrock E. Dennison A. (2023). A systematic review of the barriers to the implementation of artificial intelligence in healthcare. Cureus 15:e 46454. 10.7759/cureus.46454 37927664 PMC 10623210 · doi ↗ · pubmed ↗
- 4Ai M. Liu Y. Liu D. Yan C. Wang X. Chen X. (2025). Research progress in predicting the conversion from mild cognitive impairment to Alzheimer’s disease via multimodal MRI and artificial intelligence. Front. Neurol. 16:1596632. 10.3389/fneur.2025.1596632 40529431 PMC 12171368 · doi ↗ · pubmed ↗
- 5Al Harkan K. Sultana N. Al Mulhim N. Al Abdul Kader A. M. Alsafwani N. Barnawi M. (2024). Artificial intelligence approaches for early detection of neurocognitive disorders among older adults. Front. Comput. Neurosci. 18:1307305. 10.3389/fncom.2024.1307305 38444404 PMC 10913197 · doi ↗ · pubmed ↗
- 6Alzheimer’s Disease International. (2024). World-Alzheimer-Report-2024. Available: https://www.alzint.org/u/World-Alzheimer-Report-2024.pdf [Accessed October 21, 2025].
- 7Arikan F. B. Cetintas D. Aksoy A. Yildirim M. (2025). A deep learning approach to Alzheimer’s Diagnosis Using EEG Data: dual-attention and Optuna-Optimized SVM. Biomedicines 13:2017. 10.3390/biomedicines 13082017 40868268 PMC 12383294 · doi ↗ · pubmed ↗
- 8Axelsson A. Buschmeier H. Skantze G. (2022). Modeling feedback in interaction with conversational agents—a review. Front. Comput. Sci. 4:744574. 10.3389/fcomp.2022.744574 · doi ↗