Optimizing phenytoin therapy: a systematic review of clinically relevant food and herb interactions
Adriana Monserrath Orellana-Paucar, Erick Thomas Mosquera-Lopez, Nancy Michelle Bustamante-Alvarez, María Gabriela Machado-Orellana, Daniela Alejandra Vintimilla-Rojas, John Diego Atiencia-Palacios, Ana Cristina Espinoza-Fajardo

TL;DR
This paper reviews how foods and herbs interact with phenytoin, a seizure medication, to help doctors prescribe it more safely.
Contribution
The study systematically reviews and categorizes clinically relevant food and herb interactions with phenytoin, offering new insights for safer drug administration.
Findings
Folic acid can be co-administered with phenytoin without affecting drug levels or efficacy.
Piperine may increase phenytoin absorption and plasma levels, requiring monitoring.
Noni may reduce phenytoin levels to subtherapeutic concentrations and should be avoided.
Abstract
Phenytoin, a widely prescribed anticonvulsant, presents clinical challenges due to its narrow therapeutic index and potential interactions with various foods, herbs, and medications. These interactions can lead to adverse effects or subtherapeutic responses, necessitating a thorough understanding by healthcare professionals to optimize patient care. This systematic review investigates clinically significant interactions between phenytoin and dietary components. A comprehensive search across PubMed, Scopus, and the Health Virtual Library identified relevant studies published from January 1960 to December 2024. Data extraction utilized standardized forms, and evidence certainty was evaluated using the GRADE criteria. Twelve of the 826 initially identified articles met the inclusion criteria. Findings revealed diverse interactions: three articles reported no interaction, five indicated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
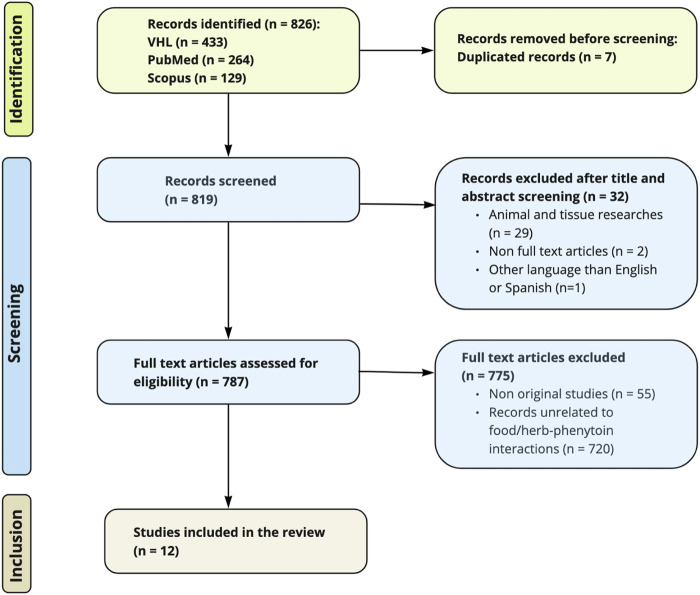 FIGURE 1
FIGURE 1| Article reference | Type of study | Aim(s) | Population | Results | Prescribed drugs | Pharmacological interaction and dosage | Study limitations |
|---|---|---|---|---|---|---|---|
|
| Randomized Controlled Trial | To describe the effect of folic acid depletion on cognition in patients with epilepsy treated with phenytoin and carbamazepine | Eighteen patients aged 18–50 years with a diagnosis of cryptogenic epilepsy | No changes were observed in serum antiepileptic drug concentration or seizure frequency following folic acid administration | Experimental group: phenytoin 340 mg/day (mean dose) | Food-Drug Interaction | The study did not involve dose-response gradient and did not control for potential confounding factors, including diet, herbal tea consumption, and the use of self-prescribed medications |
|
| Randomized Controlled Trial | To compare the bioavailability of phenytoin sodium solution and phenytoin acid suspension in healthy volunteers receiving continuously infused enteral feeding | Ten healthy volunteers aged 23–43 years | No significant difference in bioavailability is observed between phenytoin sodium solution and phenytoin acid suspension when administered with continuous enteral feeding | Phase A: Phenytoin sodium solution (435 mg) i.v.; Phase B: Phenytoin acid suspension (400 mg) through a nasogastric tube; Phase C: Phenytoin sodium solution (435 mg) via nasogastric tube | Food-drug Interaction | The study design limits generalizability due to differences in phenytoin administration route compared to long-term treatment in outpatients, single-dose and nonblinded assessment, and recruitment of healthy volunteers. Furthermore, the sample size is minor (n = 10). Adherence to treatment varies: two participants drop out the study |
|
| Randomized Controlled Trial | To investigate the possible influence of a high-fat meal on the bioavailability and pharmacokinetics of phenytoin (Dilantin Kapseals) in healthy volunteers | Twenty-four healthy volunteers (10 men and 14 women); aged 29–69 years | No significant differences in maximum concentration or extent of absorption were observed between fed and fasted states | Fed and fasted conditions: 100 mg phenytoin (Dilantin Kapseal) | Food-Drug Interaction | Study generalizability is limited by the use of healthy volunteers and a single-dose design, which may not reflect phenytoin bioavailability in patients with epilepsy receiving long-term treatment |
| Article reference | Type of study | Aim(s) | Population | Results | Prescribed drugs | Pharmacological interaction and dosage | Study limitations |
|---|---|---|---|---|---|---|---|
|
| Quasi-Experimental Study | To determine the possible influence of mealtime on the bioavailability of phenytoin | Eight healthy volunteers (1 woman and 7 men); aged 23–27 years | Phenytoin absorption is accelerated when administered with a 440 kcal meal (20% protein, 35% fat, 45% carbohydrates) | Phenytoin 300 mg | Food-Drug Interaction | The study was conducted on a minor sample (n = 8) of healthy volunteers, and the process of selecting participants was not specified |
|
| Quasi-Experimental Study | To analyze the effect of the consumption of food containing piperine ( | Six healthy volunteers (2 women and 4 men). No information regarding age was provided | Piperine from pepper may increase phenytoin absorption and delay its elimination, potentially by inhibiting drug metabolism | Phenytoin 300 mg, 30 min after breakfast | Food-Drug Interaction. Experimental group: 200 mL of soup containing tomato, tamarind, coriander, legumes, garlic, fennel, asafoetida, and pepper (1 g/200 mL soup) | The process for selecting study participants was not specified. The evaluation focused on a minor sample (n = 6) of healthy volunteers, which limits the generalizability of the findings. Results were not assessed based on a dose-response relationship |
|
| Randomized Controlled Trial | To examine the interdependence of phenytoin and folic acid in six healthy women | Six healthy female volunteers; aged 28–39 years | In comparing two treatment approaches, treatment 2, which was associated with increased serum folic acid levels, resulted in faster attainment of phenytoin steady state compared to treatment 1, which was associated with decreased serum folic acid levels | Treatment 1: 300 mg sodium phenytoin/day for 22 days | Food-Drug Interaction | Limitations of this study include the recruitment of only healthy volunteers, an imprecise selection method for study subjects, and deficient control over the participants’ daily diets |
|
| Quasi- Experimental Study | To investigate the influence of piperine on phenytoin kinetics in healthy volunteers | Five healthy male volunteers; aged 25–40 years | Co-administration of piperine enhanced phenytoin absorption | Phenytoin 300 mg | Food-Drug Interaction. Piperine: 20 mg | The study employed a single-dose design conducted exclusively on healthy volunteers. The selection method for participants was imprecise and the small sample size limits the generalizability of the findings. There was a lack of control for potential confounding factors, such as diet, herbal tea consumption, and the use of self-prescribed medications |
|
| Quasi- Experimental Study | To explore the effect of a single dose of piperine in patients with uncontrolled epilepsy on the steady-state pharmacokinetics of phenytoin | Twenty patients aged 20–45 years with a diagnosis of epilepsy | Piperine increased significantly the mean plasma concentration of phenytoin at most of the time points in both dose groups assessed | Phenytoin 150 mg or 200 mg twice daily | Food-Drug Interaction. Piperine: 20 mg | The selection process of participants was not described. There was insufficient control over potential confounding factors, including diet, consumption of herbal teas, and the use of self-prescribed medications |
| Article reference | Type of study | Aim(s) | Population | Results | Prescribed drugs | Pharmacological interaction and dosage | Study limitations |
|---|---|---|---|---|---|---|---|
| Martikainen et al. (2012) ( | Case Report | To describe the benefits of combining phenytoin, oxcarbazepine, and levetiracetam with a low glycemic index diet in treating epilepsy related to mutations in the mitochondrial polymerase gamma gene (POLG) | One woman with severe headaches, visual flashing, speech difficulty and generalised seizures; aged 26 years | A combination therapy of phenytoin, oxcarbazepine, levetiracetam, and a low-glycemic-index diet was both effective and well-tolerated in a patient with severe episodes of POLG-related mitochondrial epilepsy with nonconvulsive status epilepticus | No dose of phenytoin was reported | Food-Drug Interaction | Dosing information for phenytoin, oxcarbazepine, and levetiracetam was not provided. The specific composition of the low glycemic index diet was not detailed |
| Article reference | Type of study | Aim(s) | Population | Results | Prescribed drugs | Pharmacological interaction and dosage | Study limitations |
|---|---|---|---|---|---|---|---|
|
| Case Report | To report an unsafe herb-drug interaction between noni juice and phenytoin | One man with a diagnosis of epilepsy; aged 49 years | Consumption of noni juice was associated with subtherapeutic phenytoin levels and subsequent loss of seizure control | Without noni juice: 600 mg/day of phenytoin was administered during the first 7 days. On day 11, the dose was readjusted to 500 mg/day | Herb-Drug Interaction | Limited generalizability due to single-patient approach |
|
| Case Report | To describe the case of an elderly patient hospitalized for pneumonia who experienced the loss of seizure control due to an interaction between an oral supplement (Ensure) and phenytoin | One man with a diagnosis of chronic obstructive pulmonary disease and multiple episodes of pneumonia; aged 62 years | Oral feeding with Ensure was associated with subtherapeutic plasma levels of phenytoin, leading to loss of seizure control | Pre-hospitalization: 300 mg of phenytoin and 120 mg of phenobarbital. Hospitalization | Food-Drug Interaction. Three daily doses of 240 mL of Ensure were administered for 7 days | Given that this was an elderly patient with several comorbidities, the findings may not be relevant to younger patients diagnosed with epilepsy. Additionally, there was no information provided about potential confounding factors, such as the nutritional alternative prescribed in place of Ensure |
|
| Case Report | To inform the case of an elderly patient who suffered a faltal breakrhrough seizure due to herb-drug interaction among the prescribed anticonvulsants (phenytoin and valproic acid) and | One man with a diagnosis of epilepsy; aged 55 years | Autopsy results revealed that the serum levels of both anticonvulsants were below therapeutic ranges | No doses of anticonvulsant drugs were specified | Herb-Drug Interaction. No dose of | Single-patient approach. Unspecified dietary information. The source of information regarding the administration of non-prescribed drugs (including |
| Reference | 1. Study design | 2. Risk of bias | 3. Inconsistency | 4. Indirectness | 5. Imprecision | 6. Publication bias | 7. Magnitude of effect | 8. Dose-response gradient | 9. Confounding factors | GRADE final rating |
|---|---|---|---|---|---|---|---|---|---|---|
|
| Strong | Moderate | Strong | Strong | Strong | Strong | Moderate | Weak | Weak | Moderate |
|
| Strong | Weak | Weak | Weak | Weak | Strong | Weak | Weak | Moderate | Very Low |
|
| Strong | Weak | Strong | Weak | Weak | Strong | Weak | Weak | Strong | Very Low |
|
| Moderate | Weak | Weak | Weak | Weak | Strong | Weak | Weak | Strong | Very Low |
|
| Moderate | Weak | Strong | Weak | Weak | Strong | Weak | Weak | Strong | Very Low |
|
| Strong | Weak | Strong | Weak | Weak | Strong | Weak | Weak | Strong | Very Low |
|
| Moderate | Weak | Strong | Weak | Weak | Strong | Weak | Weak | Weak | Very Low |
|
| Moderate | Weak | Strong | Strong | Strong | Strong | Moderate | Strong | Weak | Moderate |
|
| Weak | Weak | Strong | Strong | Weak | Strong | Weak | Weak | Moderate | Very Low |
|
| Weak | Moderate | Strong | Strong | Weak | Strong | Moderate | Strong | Strong | Moderate |
|
| Weak | Weak | Strong | Strong | Weak | Strong | Weak | Strong | Weak | Very Low |
|
| Weak | Weak | Strong | Strong | Weak | Strong | Weak | Weak | Weak | Very Low |
- —Universidad de Cuenca10.13039/501100018776
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedicinal Plants and Neuroprotection · Morinda citrifolia extract uses · Vitamin C and Antioxidants Research
Background
1
The intricate interplay among medications, food, and herbal remedies presents a significant challenge in clinical practice. Food and medicinal plants, rich in diverse nutrients and bioactive compounds, have the potential to interact with pharmaceutical drugs, leading to changes in their pharmacokinetic and pharmacodynamic properties (Vuong et al., 2023). These interactions can manifest as beneficial or adverse effects, influencing the therapeutic outcome (Wang et al., 2025; Babos et al., 2021). While drug-drug interactions are often well-documented, the interactions between drugs and food or medicinal plants are typically less recognized and understood (Amadi and Mgbahurike, 2018). This knowledge gap underscores the necessity of understanding the potential for such interactions to optimize patient care and reduce the risk of adverse events.
Phenytoin, a commonly prescribed anticonvulsant, exhibits complex pharmacokinetic properties that various factors, including interactions with food and herbs, can influence. Phenytoin exerts its anticonvulsant effects primarily by stabilizing neuronal membranes and reducing neuronal excitability (Hakami, 2021). It accomplishes this by blocking voltage-gated sodium channels, which inhibits the repetitive firing of action potentials (Patocka et al., 2020) Maintaining phenytoin plasma concentrations within a narrow therapeutic range is crucial for achieving optimal seizure control while minimizing the risk of toxicity. Phenytoin is highly protein-bound, primarily to albumin. Hypoalbuminemia, a condition where albumin levels are low, can significantly increase the free fraction of phenytoin in the bloodstream. This can lead to elevated levels of pharmacologically active drugs and potentially raise the risk of toxicity, even with seemingly normal total phenytoin levels (Wilfred et al., 2022; Hong et al., 2009; Chang et al., 2020). The narrow therapeutic index of phenytoin and its susceptibility to various interactions necessitate careful monitoring and individualized dosage adjustments to ensure optimal clinical outcomes.
Phenytoin’s metabolism is crucial to its safety and efficacy profile. Understanding its metabolic pathway and potential adverse effects is essential for its safe and effective use. The CYP2C9 enzyme system primarily metabolizes phenytoin in the liver (Chang et al., 2020; Crane and Wiegand, 2023; Kan et al., 2021). Importantly, this metabolic pathway is saturable, meaning the enzyme system can be overwhelmed at higher concentrations. This saturation kinetics results in a non-linear relationship between dose and serum concentration. Even small increases in dose, when serum concentrations are already high, can cause disproportionately large increases in serum levels, significantly elevating the risk of toxicity (Wu et al., 2013).
Due to its saturable metabolism, phenytoin shows dose-dependent toxicity, with the risk of adverse effects significantly increasing as serum concentrations surpass the therapeutic range (Iorga and Horowitz, 2023). Phenytoin can lead to a wide array of adverse effects, which can be generally classified as acute or long-term. Acute adverse effects typically arise shortly after administration or with dose escalations. These may include central nervous system effects such as dizziness, ataxia, nystagmus, sedation, confusion, slurred speech, headache, and gastrointestinal disturbances like nausea and vomiting. Long-term adverse effects can develop gradually with extended use and include gingival hyperplasia, hirsutism, osteoporosis, cognitive impairment, hepatotoxicity, and severe dermatological reactions, such as Stevens-Johnson syndrome and toxic epidermal necrolysis (Patocka et al., 2020; Waterhouse and Hale, 2013; Puri et al., 2023).
Careful monitoring of adverse effects, appropriate dose adjustments, and patient education are essential to minimize the risk of complications associated with phenytoin therapy.
Despite the widespread use of phenytoin and the well-documented effects of food and herbs on drug pharmacokinetics and pharmacodynamics, there remains a lack of readily accessible, comprehensive, and evidence-based information regarding phenytoin interactions with these agents. This knowledge gap can lead to suboptimal therapeutic management, increasing the risk of adverse events and therapeutic failures in patients receiving phenytoin. To address this critical issue, the present systematic review aims to conduct a thorough and systematic analysis of the existing literature on phenytoin interactions with food and herbs. The goal is to provide healthcare professionals with a comprehensive and evidence-based resource to guide clinical decision-making, promote preventive measures, and ultimately optimize therapeutic outcomes for patients prescribed phenytoin.
Methods
2
Guidelines and protocol
2.1
This systematic review followed the Preferred Reporting Items for Systematic Reviews statement (PRISMA) (Page et al., 2021). It adhered to the protocol titled “Interactions of clinical relevance associated with the concurrent administration of prescription drugs and food or medicinal plants: a systematic review protocol” (PROSPERO registration number CRD42018117308) (Orellana et al., 2020).
Search strategy
2.2
The search strategy was developed using the Patient/Problem, Intervention, Comparison group, and Outcome (PICO) framework, focusing on patients with epilepsy or individuals receiving phenytoin therapy (Population), examining phenytoin co-administration with food or herbal products (Intervention/Exposure), compared with phenytoin administration without such co-exposures (Comparator), to determine clinical outcomes related to pharmacokinetic and pharmacodynamic interactions (Outcomes), using human studies including clinical trials, observational studies, and case reports (Study designs). A comprehensive literature search was conducted from January 1960 to December 2024 across three databases: PubMed, Scopus, and the Virtual Health Library (VHL). The search employed a combination of Medical Subject Headings (MeSH) and keywords, such as “food-drug interaction,” “plant-drug interaction,” “herbal-drug interaction,” “phenytoin,” and “epilepsy.” Duplicate articles were identified and removed. Additionally, a lateral search of the reference lists from selected studies in PubMed was performed to minimize the potential for omitting relevant articles.
Selection and exclusion criteria
2.3
Three independent reviewers conducted the article selection process for this systematic review. Studies were deemed eligible for inclusion if they met the following criteria: (a) published in English or Spanish; (b) original, full-text articles; (c) conducted in human subjects across all age groups (from birth to ≥65 years); (d) explored the pharmacological interactions between phenytoin and concurrently administered food or herbal products; and (e) used a case report, clinical trial, comparative, or observational study design. Articles were excluded if they: (a) were published in a language other than English or Spanish; (b) were review articles; (c) involved cell culture, tissue-based, or animal research; or (d) were duplicates.
Data extraction
2.4
Data extraction from the selected studies was performed independently by three reviewers using a standardized spreadsheet. Any discrepancies in data entry were resolved through consensus following a re-review of the original article. The following data elements were extracted:
- Publication details: authors, year of publication, language, title, journal, country where the study was conducted, and funding sources;
- Study design: type of study (e.g., clinical trial, quasi-experimental, case report, case-control, cohort, observational), methods of participant recruitment, and data collection methods;
- Study objectives, outcomes, and outcome measures;
- Participant characteristics: sample size, demographic and socioeconomic characteristics, age group stratification (children <18 years, adults 19–65 years, older adults >65 years), and specific physiological conditions (e.g., pregnancy, lactation);
- Phenytoin: daily dose administered;
- Pharmacological interaction: type of interaction (food-drug or herb-drug);
- Food: type of food (e.g., fruits, vegetables, dairy), specific food item (e.g., cow’s milk, beef), scientific name (for fruits and vegetables), and reported amount consumed;
- Herbs: scientific name of the plant, type of herbal preparation (e.g., infusion, herbal product), and reported amount consumed or dose of active constituents administered;
- Safety issues: reported adverse reactions; and
- Study limitations: potential biases (e.g., response bias, selection bias) and other limitations.
Evaluation of the certainty of evidence
2.5
The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system was used to thoroughly assess the certainty of evidence across the studies included in this review (Schünemann et al., 2013). The GRADE framework emphasizes five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Based on these domains, the quality of evidence was classified as high, moderate, low, or very low.
Data synthesis
2.6
Data synthesis was performed using a narrative approach, providing a comprehensive summary of the findings from the selected studies. This narrative synthesis emphasized a critical analysis of the reliability of the evidence from the twelve chosen articles to clarify the clinical characteristics and safety concerns related to pharmacological interactions between phenytoin and food or herbal products.
Results
3
Search results
3.1
The initial database searches yielded 826 articles (VHL: 433, PubMed: 264, Scopus: 129). After removing seven duplicates, 819 articles underwent title and abstract screening. Of these, 32 records were excluded for not meeting the eligibility criteria. A full-text review was conducted on the remaining 787 articles, excluding 775 articles that were either not original research articles or did not focus on interactions between phenytoin and food or herbs. Twelve studies fulfilled the predefined selection criteria and were included in this systematic review. The selected studies comprised four randomized controlled trials, four quasi-experimental studies, and four case reports. Figure 1 provides a visual representation of the study selection process.
Flow chart based on the PRISMA statement.
Identified interactions
3.2
Of the twelve included studies, three reported no pharmacological interactions between phenytoin and the investigated nutrients/foods or herbs (Hernández et al., 2005; Doak et al., 1998; Cook et al., 2001). Five studies described nutrient/food-phenytoin interactions that enhanced drug absorption (Melander et al., 1979; Velpandian et al., 2001; Berg et al., 1995; Bano et al., 1987; Pattanaik et al., 2006), while one reported improved drug effectiveness (Martikainen et al., 2012). Conversely, three studies documented decreased phenytoin’s anticonvulsant effect due to food/herb-phenytoin interactions (Kang et al., 2015; Longe and Smith, 1988; Kupiec and Raj, 2005). Tables 1–4 provide detailed information regarding these studies’ findings.
Certainty of evidence evaluation
3.3
One clinical trial was rated as having moderate-quality evidence (Hernández et al., 2005), while the other three randomized clinical trials (RCTs) were assessed as having very low-quality evidence (Doak et al., 1998; Cook et al., 2001; Berg et al., 1995). Similarly, three quasi-experimental studies were classified as very low-quality evidence (Melander et al., 1979; Velpandian et al., 2001; Bano et al., 1987), and only one was rated as moderate quality (Pattanaik et al., 2006). Among the case reports, one was assessed as moderate quality (Kang et al., 2015), and three were considered very low quality (Martikainen et al., 2012; Longe and Smith, 1988; Kupiec and Raj, 2005). Table 5 provides a detailed rationale for the GRADE rating of each included study based on nine components: study design, risk of bias, inconsistency, indirectness, imprecision, publication bias, magnitude of effect, dose-response gradient, and confounding factors.
Discussion
4
Phenytoin, a widely prescribed antiepileptic drug since 1938, remains a first-line treatment option for epilepsy due to its established efficacy. Its effectiveness derives from its ability to block both voltage-gated and frequency-gated sodium channels for longer durations than other antiepileptic drugs (AEDs), effectively suppressing high-frequency neuronal firing. Additionally, phenytoin is thought to increase brain levels of inhibitory neurotransmitters such as serotonin and gamma-aminobutyric acid, promoting functional equilibrium at the neuronal membrane level (Besag and Vasey, 2021).
Despite its therapeutic benefits, phenytoin’s narrow therapeutic index and potential adverse effects, especially with long-term use, require careful consideration. Cognitive impairment affects about 70% of individuals with epilepsy, and phenytoin has been linked to worsening this issue (Novak et al., 2022). In addition to its direct neurocognitive effects, phenytoin has been shown to lower serum folate concentrations, which may contribute to cognitive decline. Phenytoin affects folate absorption and metabolism, decreasing plasma folate levels (Kathiravan et al., 2021). Importantly, folate administration does not seem to influence phenytoin plasma concentrations, as highlighted in a moderate-quality RCT (Hernández et al., 2005) Including patients with epilepsy in the study enhances the clinical relevance of these findings. However, confounding factors like herb or food consumption were not controlled, and there was no assessment of a dose-response gradient. Conversely, a very low-quality RCT examining the co-administration of phenytoin and folic acid found that folate supplementation helped achieve steady-state phenytoin levels faster, indicating improved AED absorption (Berg et al., 1995). The study’s drawbacks included recruiting only healthy volunteers, an imprecise participant selection method, and insufficient control over daily diets. Considering both pieces of evidence, particularly the moderate-quality one, folate administration seems beneficial for patients on chronic phenytoin therapy to reduce the risk of folate deficiency without impacting AED plasma concentrations.
A case report documented a reduction in phenytoin plasma concentration to subtherapeutic levels, leading to a loss of seizure control attributed to the consumption of noni juice (Morinda citrifolia) (Kang et al., 2015). Although it is a single case study, it presents moderate evidence certainty due to the observed dose-response relationship supporting this interaction.
Unlike the previous case with noni, the low-rated certainty of the evidence in the case report regarding a possible interaction between phenytoin and Ginkgo biloba is mainly based on the single-patient approach, the absence of dietary information, and the fact that the source of information regarding the administration of Ginkgo biloba was not specified (Kupiec and Raj, 2005). Furthermore, the dosages of phenytoin and Ginkgo biloba given to the patient were not mentioned. Thus, solid data is insufficient to discourage this co-administration.
The findings on the co-administration of phenytoin with food show inconsistencies among the selected studies. A very low-quality RCT reported no significant influence of continuous enteral feeding on phenytoin plasma concentrations (Doak et al., 1998). This observation aligns with the results of another low-rated RCT, suggesting that a high-fat meal does not impact the pharmacokinetics or bioavailability of phenytoin (Cook et al., 2001). However, both studies have significant limitations, primarily due to the inclusion of a small sample of healthy volunteers and a single-dose approach. These findings contrast with the accelerated drug absorption noted in a very low-quality quasi-experimental study when phenytoin was administered with a meal comprising 20% protein, 35% fat, and 45% carbohydrates (Melander et al., 1979). However, this study also faces critical limitations, including sample size and focus on healthy subjects. The participant selection process was not detailed, and the single-dose method is inadequate for predicting phenytoin’s bioavailability. Further discrepancies arise when considering case reports with lower evidence (Martikainen et al., 2012; Longe and Smith, 1988). One study indicated that a low-glycemic index diet enhanced the effectiveness of phenytoin in managing POLG-related mitochondrial epilepsy, demonstrating improved control of status epilepticus (Martikainen et al., 2012). Conversely, another article reported an interaction between Ensure and phenytoin, which reduced AED plasma concentration to subtherapeutic levels (Longe and Smith, 1988). In summary, the available scientific evidence regarding potential interactions between phenytoin and food remains inconclusive, lacking the robustness to recommend or discourage co-administration.
Furthermore, two very low-quality quasi-experimental studies suggested that piperine may enhance phenytoin absorption and delay its elimination (Velpandian et al., 2001; Bano et al., 1987). The main limitations of both studies include a single-dose design with a small sample size of healthy volunteers and a lack of control over confounding factors. A third study, considered moderate quality, supports piperine’s role in improving phenytoin absorption (Pattanaik et al., 2006). This potential interaction is backed by evidence that piperine has similar effects on the absorption of other compounds, including curcumin (Pawar et al., 2021). Therefore, co-administering phenytoin and piperine appears beneficial for enhancing drug absorption, based on the moderate quality of evidence from this third study, primarily supported by the dose-response evaluation.
Conclusions and future directions
5
While drug-drug interactions associated with phenytoin are well-established, interactions between this anticonvulsant and herbs or food are less known. Given phenytoin’s narrow therapeutic index (10–20 mg/mL), it is crucial to disseminate scientific information to prevent any interactions that could alter its plasma concentration.
Given the moderate scientific quality from the available RCTs, co-administration of folic acid with phenytoin may be beneficial in preventing folate deficiency in patients receiving long-term treatment (Hernández et al., 2005). Although phenytoin has been associated with reduced folate levels, current evidence indicates that folic acid supplementarion does not significantly alter phenytoin pharmacokinetics. Accordingly, correction of folate deficiency may help mitigate potential cognitive decline in individuals with epilepsy treated with phenytoin; however, this relationship remains insufficiently demonstrated and should be interpreted with caution due to study limitations, including the lack of dose-response evaluation and inadequate control for dietary intake, herbal tea consumption, and self-prescribed medications. Future clinical studies examining phenytoin-folate interactions should employ rigorous methodological designs, including control of key confounding factors and standardized outcome measures, to strengthen the evidence base and better inform clinical recommendations.
Given the moderate level of scientific evidence presented in the case report, it is advisable to avoid co-administering noni and phenytoin whenever possible (Kang et al., 2015). As this clinical observation is only backed by preclinical studies (Chandra and Veeresham, 2011) conducting randomized, double-blind clinical trials is crucial to ascertain the effect of noni on phenytoin pharmacokinetics with a higher degree of scientific certainty.
Currently, there is no scientifically robust evidence to support or discourage the co-administration of phenytoin with food. Rigorous RCTs are needed to effectively control key variables and better understand this type of interaction. For instance, future studies should be designed to identify specific macro- or micronutrients responsible for any observed interactions.
The studies analyzed in this review regarding the potential of piperine to enhance the absorption and bioavailability of phenytoin are contradictory (Velpandian et al., 2001; Bano et al., 1987; Pattanaik et al., 2006). Based on the moderate-quality research (Pattanaik et al., 2006) this review recommends monitoring the plasma concentrations of the anticonvulsant when co-administered with piperine due to the potential inhibition of microsomal enzymatic metabolism of phenytoin triggered by piperine (Gohil and Mehta, 2009). Therefore, despite the proposed interaction, additional clinical studies are needed to determine the clinical significance of this potential interaction.
This review highlights the intricate nature of phenytoin interactions and emphasizes the need for further research to establish clear clinical guidelines. While supplementing with folic acid seems to be a reasonable strategy to counter phenytoin-induced folate deficiency, it is also advisable to avoid using noni alongside phenytoin. Furthermore, the combination of phenytoin and piperine appears to increase drug plasma concentration, which must be monitored closely due to phenytoin’s narrow therapeutic index. Future research should utilize rigorous methodologies, including randomized controlled trials with adequate sample sizes, standardized protocols, and comprehensive efficacy and safety outcomes assessments. By addressing these knowledge gaps, healthcare providers can improve phenytoin treatment and positively affect the lives of those living with epilepsy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Amadi C. N. Mgbahurike A. A. (2018). Selected Food/herb-drug interactions: mechanisms and clinical relevance. Am. J. Ther. 25, E 423–E 433. 10.1097/MJT.0000000000000705 29232282 · doi ↗ · pubmed ↗
- 2Babos M. Heinan M. Redmond L. Moiz F. Souza-Peres J. Samuels V. (2021). Herb-drug interactions: Worlds intersect with the patient at the center. Med. (Basel) 8, 44. 10.3390/MEDICINES 8080044 34436223 PMC 8401017 · doi ↗ · pubmed ↗
- 3Bano G. Amla V. Raina R. K. Zutshi U. Chopra C. L. (1987). The effect of piperine on pharmacokinetics of phenytoin in healthy volunteers. Planta Med. 53, 568–569. 10.1055/S-2006-962814 3444866 · doi ↗ · pubmed ↗
- 4Berg M. J. Stumbo P. J. Chenard C. A. Fincham R. W. Schneider P. J. Schottelius D. D. (1995). Folic acid improves phenytoin pharmacokinetics. J. Am. Diet. Assoc. 95, 352–356. 10.1016/S 0002-8223(95)00090-9 7860949 · doi ↗ · pubmed ↗
- 5Besag F. M. C. Vasey M. J. (2021). Neurocognitive effects of antiseizure medications in children and adolescents with epilepsy. Paediatr. Drugs 23, 253–286. 10.1007/S 40272-021-00448-0 33956338 · doi ↗ · pubmed ↗
- 6Chandra R. H. Veeresham C. (2011). Herb — drug interaction of noni juice and Ginkgo Biloba with phenytoin. Pharmacogn. J. 2, 33–41. 10.1016/S 0975-3575(11)80023-4 · doi ↗
- 7Chang W. C. Hung S. I. Carleton B. C. Chung W. H. (2020). An update on CYP 2C 9 polymorphisms and phenytoin metabolism: implications for adverse effects. Expert Opin. Drug Metab. Toxicol. 16, 723–734. 10.1080/17425255.2020.1780209 32510242 · doi ↗ · pubmed ↗
- 8Cook J. Randinitis E. Wilder B. J. (2001). Effect of food on the bioavailability of 100-Mg dilantin kapseals. Neurology 57, 698–700. 10.1212/WNL.57.4.698 11524482 · doi ↗ · pubmed ↗