Augmented Reality Visualization and Navigation Operationalized in Biopsy of Indeterminate Splenic Mass
Alexander S. Misono

TL;DR
Augmented reality helped guide a biopsy of a splenic mass with improved precision and safety compared to traditional imaging methods.
Contribution
Demonstrates the first successful use of AR for splenic biopsy in an outpatient setting.
Findings
AR guidance enabled accurate first-pass needle placement without complications.
AR reduced cognitive load and improved spatial awareness during the procedure.
Pathology confirmed high-grade B-cell lymphoma from the biopsy samples.
Abstract
This case report describes the successful use of an augmented reality (AR) guidance system (XR90, MediView XR Inc., Cleveland Ohio) to assist in the percutaneous biopsy of a splenic mass performed in a minor procedure room. Traditional two‐dimensional (2D) imaging modalities such as ultrasound and computed tomography (CT) present limitations in depth perception, spatial orientation, and procedural ergonomics, particularly in anatomically complex and mobile regions like the spleen. The AR system integrates real‐time ultrasound, electromagnetic (EM) tracking, and pre‐procedural CT data to generate a 3D holographic overlay within a heads‐up display (HUD), enhancing operator spatial awareness and needle control. A 69‐year‐old male with a 6 cm splenic mass underwent biopsy using the AR platform alongside ultrasound. The system enabled accurate needle placement, reduced cognitive load, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
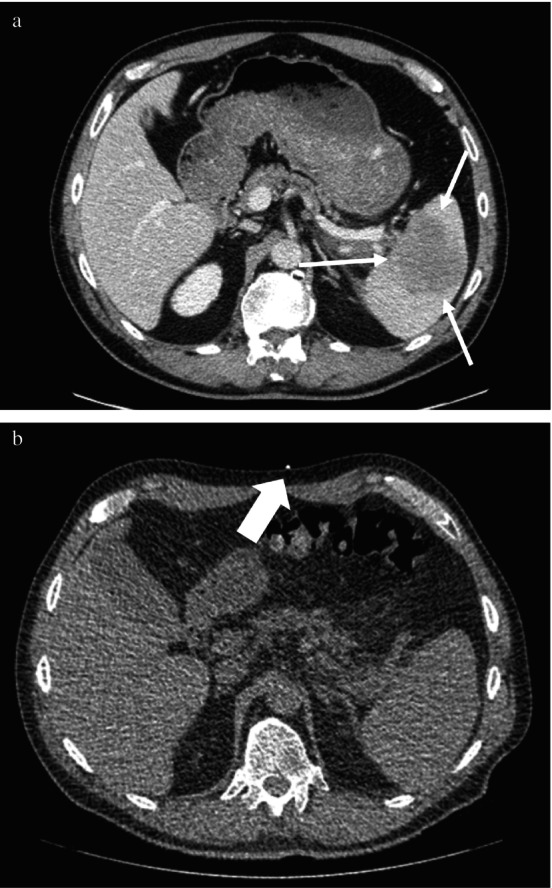 FIGURE 1
FIGURE 1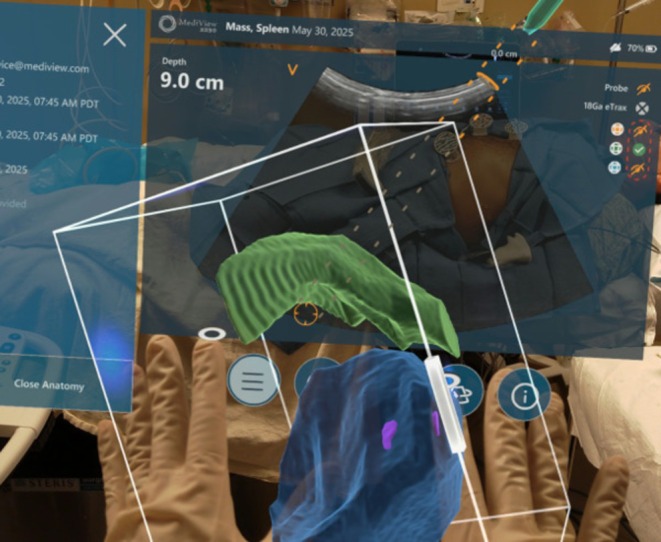 FIGURE 2
FIGURE 2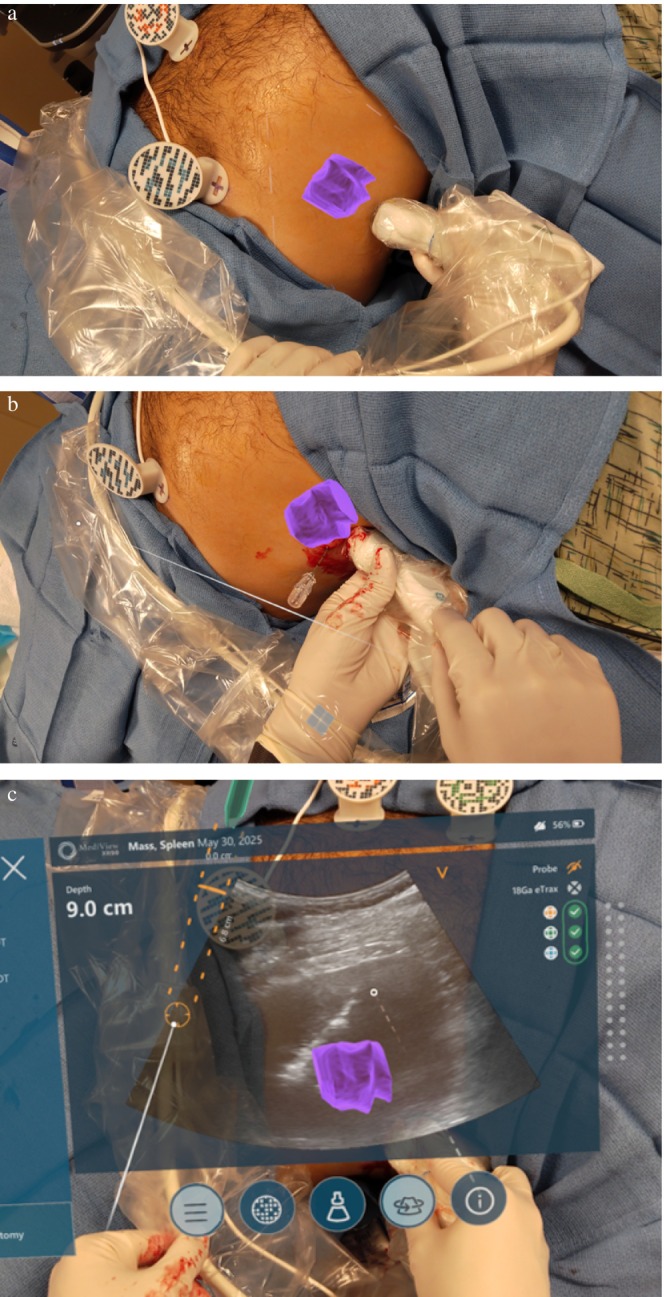 FIGURE 3
FIGURE 3| Clinical specialty | Clinical procedure | Augmented reality (AR) application | Key findings | Citation |
|---|---|---|---|---|
| Spine surgery | Percutaneous vertebroplasty | AR/AI guided trocar insertion with motion compensation | Procedure was found to be accurate, safe, and lower patient radiation exposure as compared to SOC | Auloge et al. [ |
| Spine surgery | Thoracolumbar pedicle screw instrumentation | Intraoperative 3D imaging and registration with AR‐Head Mounted Display (HMD) computer navigation for screw placement | Clinically accurate insertion of pedicle screws | Liu et al. [ |
| Neurosurgery | Neurosurgical navigation for brain tumors located on the brain surface | AR based neurosurgical navigation with 3D MRI images viewed through smart glasses | Clear visualization of the surgical field with a clinically acceptable target registration error | Maruyama et al. [ |
| Neurosurgery | Craniotomy for intracranial tumors and vascular lesions | AR neuro navigation with 3D MRI/CT reconstructions overlaying the surgical field via microscope‐ or HMD‐based visualization | AR facilitated visualization of cortex and critical structures. Preserved neurological function with no AR related complications in gross and near total resection | Gómez et al. [ |
| Orthopedics | Minimally invasive Scapula fracture surgery | Pre‐operative virtual simulation combined with intra‐operative navigation assisted fixation | Decreased procedure times and less blood loss as compared to SOC | Guo et al. [ |
| Orthopedics | Acetabular cup placement during total hip arthorplasty | AR system produced superimposed image in the surgical field via smarthphone | The AR system provided more accurate information as compared to the conventional method | Ogawa et al. [ |
| Interventional Radiology | Percutaneous tumor ablation of soft tissue tumors | AR‐HMD intraprocedural holographic guidance and navigation | Intraprocedural 3D guidance agreed with the standard imaging guidance | Gadodia et al. [ |
| Interventional Radiology | Percutaneous Ct‐guided bone biopsy | AR‐HMD intraprocedural lesion targeting and needle trajectory planning | CT passes and radiation does were significantly lower for the AR‐HMD group as compared to SOC | Albano et al. [ |
- —MediView
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAugmented Reality Applications · Surgical Simulation and Training · Soft Robotics and Applications
Introduction
1
Background
1.1
Clinicians performing percutaneous soft tissue biopsies rely on traditional medical imaging tools, predominantly 2D displays from ultrasound (US) and computed tomography (CT) to navigate through complex three‐dimensional (3D) anatomical spaces. This reliance on two‐dimensional views during three‐dimensional procedures often leads to increased cognitive and physical loads on proceduralists, potentially impacting precision and workflow efficiency [1]. Augmented reality (AR) technologies have emerged as promising tools to address these challenges by enhancing spatial orientation and visualization during minimally invasive needle‐based procedures [2, 3]. Recent cadaver and porcine preclinical studies using an AR system in percutaneous needle‐based procedures have shown that AR systems are as accurate and safe as procedures with traditional 2D image guidance, while significantly reducing needle repositions [2, 3, 4]. AR systems have also shown comparable accuracy, increased visualization, decreased radiation dose, and decreased procedure times in the neuro and orthopedic space [5, 6, 7, 8, 9]. Additional demonstrated benefits of AR system utilization are improved ergonomics, reduced operative time, and decreased blood loss [5]. Nearly all existing AR systems are designed to work within traditional operating rooms, interventional angiography suites, and/or hybrid operating room environments. The inherent complexity of intervention in these settings is an excellent match for the technological advances provided by AR systems. Furthermore, operating rooms and angiography suites typically feature tables built without metal components, a feature that is required for radiofrequency energy emission and interpretation that drives AR registration.
While AR systems have been proven to work in such settings for the purposes of supporting complex procedures, there is also a desire to perform AR procedures in minor procedure room settings, defined as designated spaces for performing outpatient procedures. Procedures in these settings are typically performed in short duration and may only require local anesthesia or moderate sedation. These rooms allow for faster procedural and patient turnover as compared with operating room or angiography suites. In interventional radiology, common procedures include paracentesis, thoracentesis, and biopsy procedures. In these settings, many ultrasound‐guided procedures are performed including those with complex or less familiar anatomy. The ability to bring AR into minor procedure room settings will allow for further democratization of this technology.
We present a case in which we performed a splenic biopsy utilizing an AR System as an adjunct to ultrasound (US)‐guided needle biopsy. Splenic biopsies are uncommon and present risks to the patient and challenges to the physician [3]. The spleen's vascularity introduces an increased risk for life‐threatening bleeding and hemorrhage following the procedure. Additionally, pneumothorax, pleural effusion, and colonic injury are known complications [10, 11]. The anatomical position of the spleen, situated in the upper abdominal cavity and partially obscured by the rib cage, complicates access and visualization, making the procedure technically demanding for the physician. The AR system supported precision‐guided needle biopsy along with 3D visualization to overcome the restrictive nature of the organ's location.
Technology Overview
1.2
Recent technological advances such as lightweight head‐mounted displays, along with tracked instruments (optical or EM) have led to an increased application of AR devices for clinical interventions across multiple specialties within the surgical and interventional space. AR devices have been successfully used for orthopedic, neurologic, surgical, urologic, and interventional radiology. Table 1 demonstrates a brief overview of recent literature published demonstrating the diverse implications for AR for intraprocedural guidance.
The benefits for AR have been well charactered for specialties with fixed locations such as neurologic or orthopedic applications. However utilizing AR for percutaneous soft tissue with which are often affected by soft tissue deformation and respiratory motion require complex solutions. One such solution is the XR90 (MediView, Cleveland, OH) system which integrates live ultrasound imaging with multimodal image fusion into a head mounted display along with tracked tools for soft tisse applications.
This platform integrates several cutting‐edge technologies to deliver its unique capabilities. The system utilizes HoloLens 2 (Microsoft, Redmond, WA) as its foundational AR Head‐Mounted Display (HMD), providing an immersive visual interface for clinicians. For real‐time tracking and precise navigation, the AR system incorporates the Aurora Electromagnetic Tracking system (Northern Digital Inc., Waterloo, Canada), which works in conjunction with electromagnetically (EM) sensor‐equipped instruments, including eTRAX (CIVCO Medical Solutions, Coralville, IA) needles and ultrasound probe bracket. Integration with commercially available ultrasound systems, such as the Vivid IQ (GE Healthcare, Chicago, IL), allows for the streaming of live ultrasound imaging to a HUD that is displayed in space. Through a registration process, 3D CT‐based models of segmented patients' anatomy are projected and registered in the procedural space.
Case Presentation
2
Patient Profile
2.1
A 69‐year‐old male presented with left‐sided abdominal pain and was found to have a 6 cm heterogeneous mass within the spleen. The patient had no significant past medical history and no history of malignancy. Other than the splenic mass, the only other finding on physical examination and imaging was nonspecific, unenlarged retroperitoneal lymph nodes. Medical oncology consulted and a splenic mass biopsy was requested to be performed in interventional radiology.
Interventional radiology review of the case revealed a normal sized spleen tucked posteriorly within the upper abdominal cavity. There was a 6 cm hypoattenuating, hypoenhancing mass within the splenic parenchyma (Figure 1a). On non‐contrast imaging, however, the splenic mass was poorly defined (Figure 1b).
(a) Hypovascular, hypoattenuating splenic mass (white arrows) is seen within the splenic parenchyma. The spleen is not enlarged and is located posteriorly within the upper abdominal cavity. (b) Noncontrast CT imaging reveals that the splenic mass is isoattenuating with splenic parenchyma and cannot easily be visualized. Large white arrow indicates one of three MediView XR90 skin markers required for registration.
While a CT‐guided biopsy could be performed using landmarks, given the splenic location, vascularity, and depth, precise needle trajectory planning and real‐time visualization were deemed important to minimize procedural risks and maximize technical success. The patient provided informed consent for the procedure and the use of the AR system.
Procedure Overview
2.2
This procedure was completed by an Interventional Radiologist with less than 1 year of AR experience. AR system specific benchtop training was completed prior to clinical procedures. The proceduralist participated in only 2 clinical cases utilizing the AR system prior to this highlighted case, highlighting ease of use. Training was performed rapidly using a phantom model provided by the vendor and consisted of an approximately 20‐min walk‐through of a pre‐existing example case.
Pre‐procedural imaging for the procedure was conducted using a conventional CT scanner. Three radio‐opaque markers were placed on the patient in the left upper quadrant (Figure 1b). Axial CT images with 1.25 mm thick reconstructions were obtained and transferred to the Picture Archiving and Communications System. Following the scan, the radio‐opaque markers were replaced with permanent surgical skin markings, after which the patient was transported to the minor procedure room.
On a separate workstation, the axial CT images were downloaded and imported into a 3D medical imaging post‐processing software (Tera Recon, Concert AI, Durham, NC). Within this workflow, the three radio‐opaque markers, the lung parenchyma of the left lower lobe, the spleen, and the splenic mass were individually contoured. Each of these segmented 3D datasets was then exported in an OBJ file format and subsequently uploaded to the AR system. With the pre‐procedural data prepared, the intervention began.
In the minor procedure room, the patient was placed onto a SurgiGraphic 6000 image‐guided surgical table (Steris, Mentor, OH), followed by sterile prep and draping of the left upper quadrant. Sterile registration markers were then placed on the skin markings. The operator donned the headset and AR registration was initiated and completed using verbal registration commands to the system.
Prior to biopsy initiation, a 3D rendering of the spleen, splenic mass, and lungs was visualized holographically for operator familiarization and treatment planning in open space (Figure 2). Subsequently, this 3D rendering and tracked tools were then registered to the electromagnetic (EM) coordinate space overlaying the 3D structures' patient's anatomy within the EM field to guide biopsy. Upon identifying the optimal trajectory, extraneous structures were removed with verbal command to localize the mass (Figure 3a). A 17‐gauge biopsy guide needle was then advanced into the splenic mass using combined AR and ultrasound guidance (Figure 3b). Core needle biopsies were subsequently performed using sonographic guidance via the head up display feature, allowing for continuous dual confirmation of needle positioning with both sonography and AR throughout the remainder of the procedure.
Treatment planning is pursued external to the patient. AR visualization of structures of interest in this case, spleen (blue), splenic mass (purple—partially visualized), and the lower lung (green) allows for dynamic manipulation of structures and review of potential procedural trajectories and plans.
(a) Splenic mass (purple) is visualized in AR onto and within the patient's anatomy. (b) 17‐gauge biopsy guide needle is advanced into the mass under sonographic and AR guidance. (c) Real‐time sonographic guidance of a percutaneous biopsy pass closure with SinglePass Kronos electrocautery is now visualized via a “heads up display” while retaining AR guidance of the splenic mass within the patient torso.
Three core needle biopsy passes were performed and three core needle specimens were successfully obtained using an 18‐gauge biopsy device (Bard Max‐Core, Becton Dickinson, Franklin Lakes, NJ). The needle track was closed with an electrocautery device (Single Pass Kronos, Single Pass, Lake Forest, CA), with clear delineation of the cauterization tract on final imaging (Figure 3C). Total procedural duration was 15 min.
The patient was observed for 4 h under bedrest restrictions and then discharged home without complications. Biopsy specimens were diagnostic. Final pathology confirmed adequate and diagnostic specimens, revealing high‐grade B‐cell lymphoma, leading to the initiation of treatment. No intra‐procedural or immediate post‐procedural complications were observed.
Discussion
3
This case report demonstrates the successful application of the AR system for a percutaneous splenic mass biopsy performed in a minor procedure room. The procedure, which can be challenging due to the spleen's anatomical location, mobility, and vascularity, was executed with precision and efficiency.
The integration of AR technology provided distinct advantages over conventional 2D ultrasound guidance. The real‐time holographic superposition of pre‐procedural CT data with live ultrasound offered an enhanced spatial understanding of the target and critical adjacent structures as compared to traditional techniques. This “X‐ray vision” capability allowed the proceduralist to navigate the needle path with increased confidence and precision, potentially reducing the risk of complications associated with inadvertent organ or vessel puncture. Furthermore, this added confidence resulted in anecdotally faster procedural time and, therefore, reduced sedation time and room utilization. This aligns with findings from other studies exploring AR in percutaneous procedures, which suggest comparable accuracy and reduced cognitive load compared to traditional guidance methods [3, 16].
A key implication of this case is the demonstrated feasibility of operationalizing advanced AR navigational technology in a minor procedure room. Historically, such image‐guidance systems have been confined to highly equipped operating rooms or angiography suites due to infrastructure requirements coupled with perceived complexity. This successful application in a less specialized setting suggests broader applicability for AR systems, potentially democratizing access to precision guidance for a wider range of percutaneous interventions and treatment settings.
Conclusion
4
The AR system effectively guided a percutaneous splenic mass biopsy in a minor procedure room, demonstrating enhanced anatomical visualization, improved procedural ergonomics, and successful target acquisition without complications. This case highlights the system's potential to improve precision and efficiency in challenging interventions and suggests a broader utility of AR technology in diverse clinical environments beyond conventional specialized suites.
Author Contributions
Alexander S. Misono: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing – original draft, writing – review and editing.
Funding
MediView provided funding for publication fees.
Ethics Statement
As a single case report with the patient's signed consent, no other ethical review was required.
Consent
Written informed consent was obtained from the patient for the publication of this case report.
Conflicts of Interest
Author is a member of the Scientific Advisory Board for MediView XR Inc.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. Lusch , P. L. Bucur , A. D. Menhadji , et al., “Evaluation of the Impact of Three‐Dimensional Vision on Laparoscopic Performance,” Journal of Endourology 28, no. 2 (2013): 261–266.10.1089/end.2013.034424059674 · doi ↗ · pubmed ↗
- 2G. Gadodia , J. Yanof , A. Hanlon , et al., “Early Clinical Feasibility Evaluation of an Augmented Reality Platform for Guidance and Navigation During Percutaneous Tumor Ablation,” Journal of Vascular and Interventional Radiology 33, no. 3 (2022): 333–338.35221048 10.1016/j.jvir.2021.11.014 · doi ↗ · pubmed ↗
- 3G. Gadodia , M. Evans , C. Weunski , A. Ho , A. Cargill , and C. Martin , “Evaluation of an Augmented Reality Navigational Guidance Platform for Percutaneous Procedures in a Cadaver Model,” Journal of Medical Imaging 11, no. 6 (2024): 062602.38370135 10.1117/1.JMI.11.6.062602 PMC 10868591 · doi ↗ · pubmed ↗
- 4S. Datta , R. F. Short , J. W. Milsom , et al., “In‐Vivo Evaluation of an Augmented Reality Enhanced Ultrasound Needle Guidance System for Minimally Invasive Procedures in Porcine Models: A Preclinical Comparative Study,” Journal Minimum Invasive Surgery 28, no. 3 (2025): 122–129.10.7602/jmis.2025.28.3.122PMC 1243904440947929 · doi ↗ · pubmed ↗
- 5Q. Guo , X. Li , Y. Tang , Y. Huang , and L. Luo , “Augmented Reality and Three‐Dimensional Plate Library‐Assisted Posterior Minimally Invasive Surgery for Scapula Fracture,” International Orthopaedics 46, no. 4 (2022): 875–882.35061064 10.1007/s 00264-022-05303-6 · doi ↗ · pubmed ↗
- 6P. Auloge , R. L. Cazzato , N. Ramamurthy , et al., “Augmented Reality and Artificial Intelligence‐Based Navigation During Percutaneous Vertebroplasty: A Pilot Randomised Clinical Trial,” European Spine Journal 29, no. 7 (2020): 1580–1589.31270676 10.1007/s 00586-019-06054-6 · doi ↗ · pubmed ↗
- 7E. Faiella , G. Castiello , C. Bernetti , et al., “Impact of an Augmented Reality Navigation System (SIRIO) on Bone Percutaneous Procedures: A Comparative Analysis With Standard CT‐Guided Technique,” Current Oncology 28, no. 3 (2021): 1751–1760.34066651 10.3390/curroncol 28030163 PMC 8161791 · doi ↗ · pubmed ↗
- 8N. Montemurro , S. Condino , M. Carbone , et al., “Brain Tumor and Augmented Reality: New Technologies for the Future,” International Journal of Environmental Research and Public Health 19 (2022): 6347.35627884 10.3390/ijerph 19106347 PMC 9141435 · doi ↗ · pubmed ↗