An innovative model for integrated delivery of prevention, screening and palliative care services of cancers at health and wellness centres in Assam
Rewati Raman Rahul, Nandini Vallath, Kunal Oswal, Ravikant Singh, Kumar Gaurav, Paul Sebastian, Venkataramanan Ramachandran, Arnie Purushottham

TL;DR
This paper presents a model for integrating cancer prevention, screening, and palliative care services in Assam through health and wellness centers.
Contribution
The study introduces a practical model for integrated cancer care delivery using frontline healthcare workers in Assam.
Findings
2106 households were screened, with 3.1% positivity for oral cancer, 1.8% for breast cancer, and 3.4% for cervical cancer.
0.5% of households were identified as needing palliative care, and all positive cases received counseling for further diagnostics.
Ambulance services were arranged for those needing diagnostics, demonstrating the model's practical application potential.
Abstract
There is a consensus on delivering prevention, early detection and palliative care services as effective cancer control strategies in primary healthcare settings; however, examples of practical application are few. The study describes the implementation of integrated delivery of preventive, early detection and palliative care needs assessment through the frontline healthcare workers at the Health and Wellness Centre. The study employed a master trainer team of dentist and nurses trained in prevention and needs assessment of palliative care services who would further provide the handhold training to the Community Health Officers (CHO), multi purpose workers and Accredited Social Health Activist for awareness, prevention and generalist palliative care needs assessment. 2106 households with 256 people were screened as a result, with an average of around 30 screenings a day. Screen…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
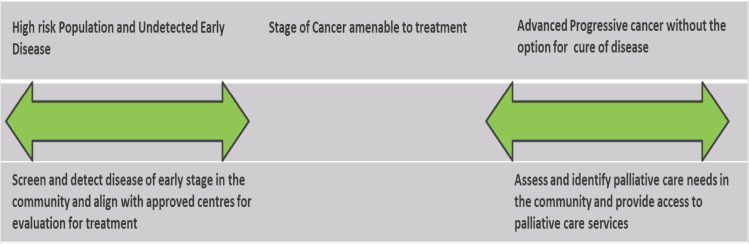 Figure 1
Figure 1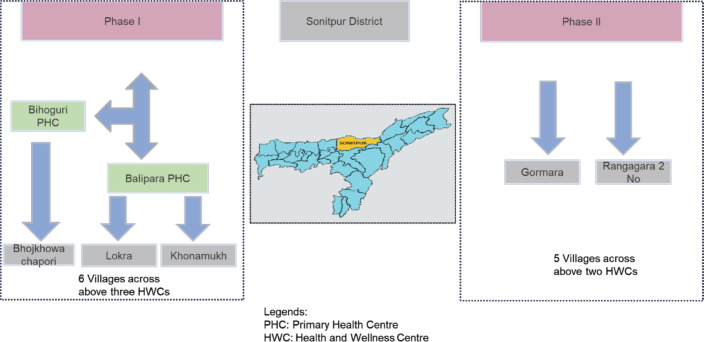 Figure 2
Figure 2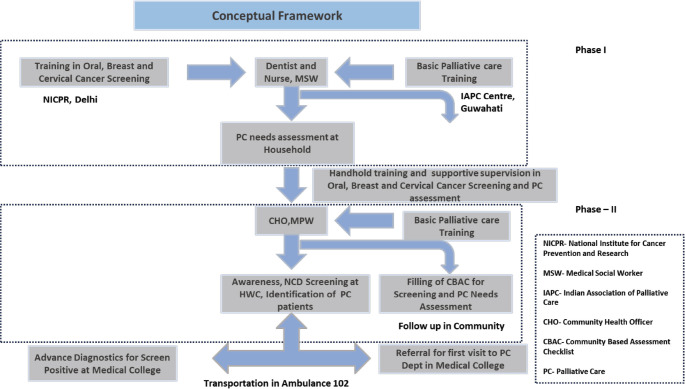 Figure 3
Figure 3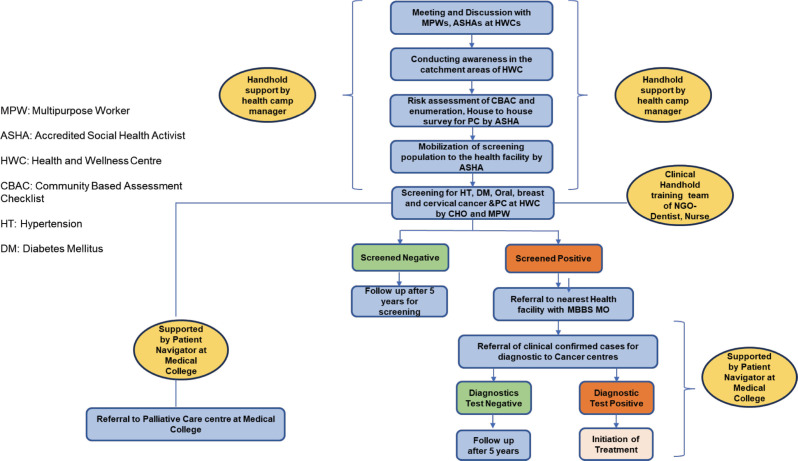 Figure 4
Figure 4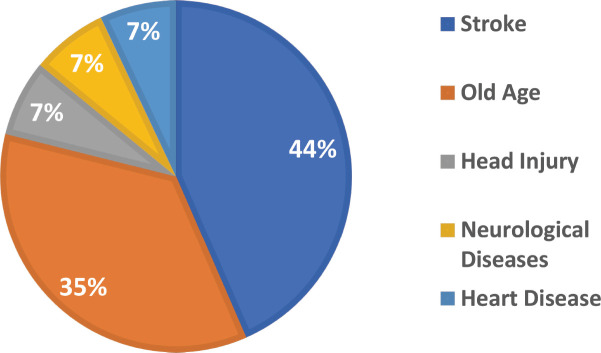 Figure 5
Figure 5- —The study was conducted as a part of collaboration for implementation of the cancer control programme between the Tata Trusts and the Government of Assam. The funding for the resources utilised for th
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare Systems and Reforms
Background
The annual incidence of cancer in India for 2022 was 1.41 million and is expected to reach 1.75 million by the year 2030 [1], while the cancer-related deaths were 0.91 million in 2022 and are estimated to reach 1.15 million by the year 2030 [2].
The overall burden due to the high incidence of cancer is worsened due to the late presentation of patients to healthcare facilities. Of the patients seeking care from cancer care institutions, more than 60 percent of cases were reported in advanced stages, not amenable to curative treatment [3]. The lack of availability of standard facilities with skilled human resources closer to home results in patients travelling to far-off regions seeking treatment and care. This leads to high out-of-pocket expenses and dropout rates across the treatment pathway [4].
Government of India (GOI) adopted a policy in the year 2010 to implement breast, cervical and oral cancer screening with clinical breast examination (CBE), visual inspection with acetic acid (VIA) and oral visual inspection, respectively, through the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) [5].
The program was scaled gradually across the country with a defined operational guideline for the management of cancer. However, there were several implementation challenges and variability across different states. In 2023, GOI launched revised operational guidelines of the programme (National Programme for Prevention and Control of Non-Communicable Diseases: NP-NCD 2023-30) having focus on primary and secondary prevention, clinical support for non-communicable diseases (NCDs) and programme management with an objective to integrate NCD care at various healthcare delivery levels mainly focussing on health and wellness centre or Ayushman Arogya Mandir (AAM) [6].
Under the flagship health programme of Ayushmann Bharat, the GoI has identified the gap and developed a package of 12 service categories to be delivered under Comprehensive Primary Health Care, at the Health & Wellness Centres (HWC) commonly known as AAM. This package contains the screening of NCDs and the palliative care services [7].
The three most common cancers in India – oral, breast and uterine cervix cancer have well‑developed interventions for screening and early detection. They also have detectable early stages (mainly precancerous – oral and cervical) that are amenable to secondary prevention [8]. There is a consensus that about 60% of cancer deaths in India can be prevented with improved preventive and screening facilities alone. Moreover, generalist palliative care skills can help relieve the health-related suffering seen in different stages of the disease [9]. The frontline health care workers can be easily trained to achieve the required skills for these interventions. Building such capacity closer to patients in need can positively impact the cancer burden in the community. The role of frontline workers, including Accredited Social Health Activists (ASHAs), has already been demonstrated to be useful in the screening programmes [10]. It is hypothesised that frontline workers could play an important role in effective cancer control by integrated primary healthcare delivery of the screening of the three common cancers, as well as identification, assessment and referral of patients in the advanced stage of the disease, who need palliative care in the community [10, 11]. However, there has been very limited translation of this idea into practice in the community.
The current study tries to present this novel model of delivering integrated services of prevention, early detection and palliative care (PEP model) through the HWCs by training frontline health workers.
Materials and Methods
The study was devised with an aim to assess the feasibility of conducting traditionally divergent activities like NCD screening and palliative care needs assessment in an integrated approach. Figure 1, named Primary Healthcare Interventions Across Prevention, Early Detection and Palliative Care Across Cancer Care Spectrum, demonstrates the intervention planned in the outreach.
The objectives of the study were
Assessment of palliative care needs in the community through a master trainer team equipped in the prevention and early detection of NCDs in the community.Delivering NCD screening and primary palliative care services through frontline healthcare workers at the HWC.
Programme design
A MoU was signed by Tata Trusts, a Non-Governmental Organisation (NGO), with the Government of Assam for the effective implementation of the project. Some of the major provisions of the MoU were to a) design and implement a cancer control programme for prevention, early diagnosis, clinical down-staging, improved treatment, survival and cure rates and better palliative care, b) integrate and upgrade comprehensive cancer-related infrastructure, personnel and services across the state from the primary health centre to tertiary referral cancer hospitals and c) devise a cancer control programme that is innovative, evidence-based, locally appropriate, low cost and cost-effective. Sonitpur district was chosen due to the necessary administrative approval from the government, ongoing collaborative team activities and access to cancer care and palliative care for screen-positive cases. Figure 2, Intervention District and Health Facilities, shows the selection of the health facilities in the districts.
A two-phase project was devised to achieve the objectives. A four-member team of a dentist, a nurse, a medical social worker and a data entry operator was constituted. The dentist and the nurses were trained in screening for NCDs, including common cancers (oral, breast and cervical) at the National Institute for Cancer Prevention and Research. The same team underwent generalist palliative care training in an essential certificate programme conducted by the Indian Association of Palliative Care at the nearby centre in Guwahati. Appendix 1, named Training Schedule for Cancer Prevention, Early Detection and Palliative Care for Dentists and Nurses of the supplementary is attached for the training curriculum and schedule. While In the first phase, this team primarily conducted the needs assessment for palliative care at the HWC with the support of the frontline health workers using the Palliative care questionnaire integrated into the Community based assessment checklist shared in Appendix 2, in the second phase it played the role of master trainer and provided hands-on training to the frontline health workers (Community Health Officers, Multipurpose Health Workers and the ASHAs) to conduct awareness and screening for NCDs including the three common cancers (oral, breast and cervical) and facilitate assessment of palliative care needs by training the ASHAs on filling the Community Based Assessment Checklist (CBAC) forms. Linkages with the specialist department at the cancer centre and medical college were set up, and the team also helped develop a pathway for referral of the screen-positive cases arising from the screening for further diagnostic tests for confirmation of cancer. The conceptual framework and referral pathway for the Prevention, Early Detection and Palliative care (PEP) study, as well as the implementation of the PEP interventions, are shown in Figure 3 and Figure 4, respectively, with the same names.
Summary of the PEP activities planned at different levels of public healthcare is shown below.
Household-level activities (conducted by ASHA)
Mapping of the households for the eligible population for NCD screening.Filling out the CBAC forms for assessment of NCD screening and the palliative care needs assessment form.Dissemination of information regarding screening camps at HWC.
Community-level intervention (conducted by ASHA)
Facilitating awareness in the community through community camps regarding thePrevention of cancer and palliative careMobilisation of the people to the HWC for screening camps.
Health facility (CHO and MPW)
Conduct screening camps at the HWC by CHO and MPW at HWC. Identifying people in need of care for palliative care through screening of CBAC forms submitted by ASHA. Manage referrals through arranged transportation for palliative care and NCD-screened cases.Follow-up of the screened positive and palliative care cases for generalist care.
Results
Results of the study are compiled in Table 1 below. During phase I of the needs assessment for palliative care, a total of 14 cases were identified to have palliative care needs across 1,035 households surveyed, with an average of 1.35% of households requiring palliative care. Figure 5 below shows the results of the data for the Needs assessment conducted for Palliative Care by disease in the first phase of the project. Stroke and old age-related illness were the top two contributors, with almost 44% and 35%, whereas heart, neurological and head injuries were other contributing factors.
In the second phase, a total of 2,106 households were covered, targeting a population of 11,811. A total of 11 talks and community awareness meetings were organised by the frontline health workers during the study period. 9 camps were organised in which a total of 256 people attended (Male: 63 and Female: 193) and were screened for oral cancer through oral visual examination methods. 163 females out of the total 193 participating females were eligible for breast cancer screening and were screened through the clinical breast examination method. 59 females out of the total 193 participating females were eligible for cervical cancer screening and were screened through visual inspection with the acetic acid method. Screen positivity rates were found to be 3.1% for oral cancer (in males, 4.76% and females 2.59%), for breast cancer, it was 1.8%, while for cervical cancer, it was 3.4%. All cancer-positive cases were counselled and followed up for their confirmatory diagnosis, in which 75% of oral suspected cases (66.6% male and 80% female) were reached and did their confirmatory test at referred centres, and 100% of breast and cervical cancer suspected cases did their confirmatory diagnosis. None of the screen-positive cases of oral, breast and cervical cancer were found to be positive after their confirmatory test at the higher centre. In the second phase of screening conducted for palliative care by the public health workers, 0.5% households required palliative care. All of these were provided services through the palliative care physician from the Baptist Christian Hospital and follow up done through the nurse-led home care team of the hospital.
Discussion
Cancer screening in India has been a least priority due to multilevel barriers in implementation and is highly variable across 28 states and 8 union territories [12]. Community-based cancer screening programs in India have shown promise for early detection and improved outcomes. VIA has been widely used for cervical cancer screening, with sensitivity ranging from 16.6% to 82.6% and specificity from 82.1% to 96.8% [13]. Reports from the experiences from Tamil Nadu, the only state in the country to have scaled up services for the prevention of common cancers and other NCDs, have revealed that effective translation of evidence depends on a range of implementation issues, including context-specific communication strategies, provision of high quality services, linkages between screening, diagnosis and treatment and uptake of evidence by policy-makers and health care providers [14]. Engaging local health workers, such as Anganwadi workers, has improved attendance and follow-up rates in screening camps [15]. A large-scale breast cancer screening program in Kerala demonstrated the feasibility of door-to-door screening, with 93% of eligible women screened and 61% of detected cases in early stages [16]. Data from our study shows that the participation rate for oral, breast and cervical screening amongst those invited in community clinics were 100%. 84.5% and 30%, respectively. In a similar programme conducted in Jharkhand, the results for participation rates for oral, breast and cervical screening were 34.9%, 34.7%and 29.9% in an all women group [17], while in another study in Uttar Pradesh, this rate was 32% for cervical [18]. Major success of the programme as shown in the study, was a compliance rate of 75%, 100% and 100% amongst the screen positives of oral, breast and cervical cancer for confirmatory diagnosis within the public health system. The same was reported to be 14.6%, 48.1% and 28.3% community screening programme in Jharkhand [17] and 70% in a study from Kolkata [19] and 60% from a study in Kerala [16] from studies. However, the unique aspect of the implementation in this study was delivery of integrated programmes of cancer awareness, screening and palliative care services. Integrating palliative care into overall cancer control strategies like cancer prevention, early detection and curative treatments allows for a seamless response while making the best use of scarce resources [20]. The current model of PEP is timely and establishes a cost-effective and sustainable way for the government to provide an effective cancer control strategy at the primary level of care by effectively implementing the National Programme of NCD for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) and National Program for Palliative Care at the HWC.
Experience at HWCs in Assam suggests that reducing the cancer burden in the community, through an integrated delivery as in the PEP approach, is a sustainable solution at primary-level public health facilities. It not only adds value to the public health programme by early detection and control of cancer, but is also effective in providing care to the incurable patients suffering from NCDs in the community near their homes.
Utilising their strengths, the NGO and government came together in making the initial effort at capacity building and stabilising the programme and shared the resources required for infrastructure, human resources and training as summarised in Table 2 below. This kind of synergistic partnership to work towards a shared vision of cancer control not only resulted in a demonstrated increase in the confidence of the primary-level healthcare providers but also led to an effective and judicious use of the resources. All of the above-mentioned factors resulted in better outcomes of the health programmes in the community.
Limitations
The study shows data from the very early stages of the program with intervention conducted over a small number of health facilities in a district. There is a need for generating further evidence from other geographies in a diverse setting. While the possibility of delivering primary care for PEP activities is possible, there will be a constant need for handholding and supervision before the services are regularly delivered at the HWCs. With further refresher training and monitoring within the health systems, the participation rates for the screening programme are more likely to go up. Presence of a nodal centre with well-established preventive and palliative care departments is an essential prerequisite for providing diagnostics and curative services for screen-positive and palliative care services. This project has already established cancer care and palliative care centres in the districts before the community training of the frontline health workers was planned. However, this may not be feasible for all the districts and would require setting up such departments first as nodal centres.
Conflict of interest
None of the authors have declared conflict of interest.
Ethical Declaration
Necessary consents were taken from the participants during the course of screening and the same has been attached at the end of the documents.
Author contributions
Conception and design: Nandini Vallath, Rewati Raman Rahul, Kunal Oswal
Administrative support: Ramachandran Venkataramanan, Kunal Oswal
Collection and assembly of data: Ravikant Singh, Kumar Gaurav, Rewati Raman Rahul
Data analysis and interpretation: Rewati Raman Rahul, Nandini Vallath, Kunal Oswal
Technical inputs and manuscript review: Nandini Vallath, Kunal Oswal, Paul Sebastian, Arnie Purushotham
Proof reading: Kunal Oswal, Paul Sebastian
Manuscript writing: All authors
Final approval of manuscript: All authors
Accountable for all aspects of the work: Rewati Raman Rahul, Kunal Oswal
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1International Agency for Research on Cancer W. H. O. Estimated Number of New Cases From 2022 to 2030, Both Sexes, Age [0–85+] All Cancers 2024 India Global Cancer Observatory
- 2International Agency for Research on Cancer W. H. O. Estimated Number of Deaths From 2022 to 2030, Both Sexes, Age [0–85+] All Cancers 2024 India Global Cancer Observatory
- 3World Health Organization Cancer Control: Knowledge Into Action: WHO Guide for Effective Programmes: Module 3: Early Detection 2007 Geneva World Health Organization 24716262 · pubmed ↗
- 4Mohanti BK Mukhopadhyay A Dash S Estimating the Economic Burden of Cancer at a Tertiary Public Hospital: A Study at the All India Institute of Medical Sciences 2011 New Delhi, India Indian Statistical Institute, Delhi Centre
- 5Ministry of Health and Family Welfare | GOI National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS)[https://main.mohfw.gov.in/Major-Programmes/non-communicable-diseases-injury-trauma/Non-Communicable-Disease-II/National-Programme-for-Prevention-and-Control-of-Cancer-Diabetes-Cardiovascular-diseases-and-Stroke-NPCDCS]
- 6National Health Systems Resource Centre (NHSRC)Operational Guidelines For Comprehensive Primary Health Care Through Health and Wellness Centers.pdf [Internet][https://nhsrcindia.org/sites/default/files/202103/Operational%20Guidelines%20For%20Comprehensive%20Primary%20Health%20Care%20through%20Health%20and%20Wellness%20Centers.pdf]Date accessed: 15/08/23
- 7Ministry of Health and Family Welfare Comprehensive Primary Health Care through Health and Wellness Centers: Operational Guidelines 2018 New Delhi Government of India, National Health Systems Resource Centre[Internet] [https://nhm.gov.in/New_Updates_2018/NHM_Components/Health_System_Stregthening/Comprehensive_primary_health_care/letter/Operational_Guidelines_For_CPHC.pdf]
- 8Rajaraman P Anderson BO Basu P Recommendations for screening and early detection of common cancers in India Lancet Oncol 201516 e 352e 36110.1016/S 1470-2045(15)00078-926149887 · doi ↗ · pubmed ↗