Bridging gaps in breast cancer care: a Breast Cancer Care Quality Index to improve outcomes worldwide
Eduardo Cazap, Benjamin O Anderson, Giuseppe Curigliano, Sandeep Sehdev, Fatima Cardoso, Ana Rita Gonzalez, Emad Shash, Cheng-Har Yip, André Mattar, Yanin Chavarri-Guerra, Miriam Mutebi, Yongmei Yin, João Victor Rocha, Ilaria Lucibello, Namita Srivastava

TL;DR
This paper introduces a new index to improve breast cancer care globally by identifying key areas for improvement and promoting equitable treatment.
Contribution
The novel contribution is the development of the Breast Cancer Care Quality Index (BCCQI) as a strategic tool for national cancer control plans.
Findings
The BCCQI includes four dimensions, 10 targets, and 23 indicators to guide country-specific breast cancer care improvements.
The index emphasizes health equity, patient centricity, universal access, and treatment effectiveness.
The BCCQI is designed to be a dynamic tool adaptable to local contexts and real-world evidence.
Abstract
Breast cancer (BC) care faces challenges in early detection, timely diagnosis and comprehensive management. Disparities persist, with underserved populations facing the greatest barriers. Addressing these requires policies that support consistent, evidence-based practices and enhance healthcare capacity and technology advancements. This document presents the development of the Breast Cancer Care Quality Index (BCCQI), supported by evidence to promote equitable care and improve BC outcomes globally, and discusses its adoption as a strategic tool within National Cancer Control Plans. A two-part methodology identified challenges in BC care and defined dimensions, targets and indicators for the BCCQI, aligned with the World Health Organization Global Breast Cancer Initiative. A literature review and analysis of existing United Nations (UN) frameworks informed the initial structure of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
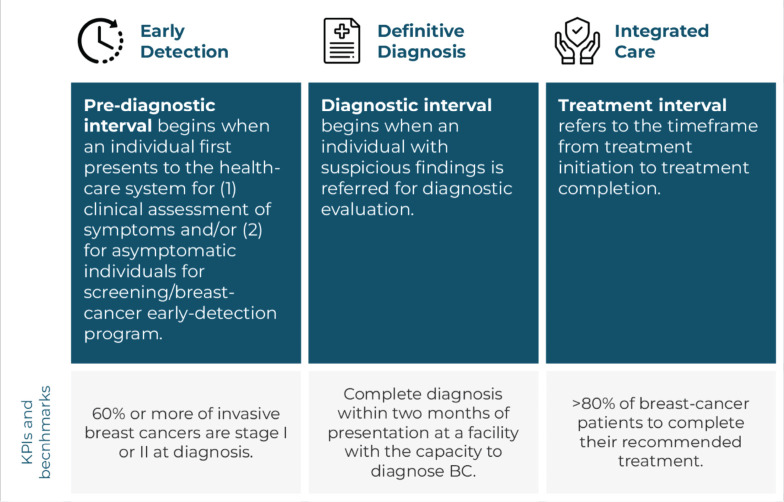 Figure 1
Figure 1 Figure 10
Figure 10 Figure 11
Figure 11 Figure 12
Figure 12 Figure 13
Figure 13 Figure 14
Figure 14 Figure 15
Figure 15 Figure 16
Figure 16 Figure 17
Figure 17 Figure 18
Figure 18 Figure 19
Figure 19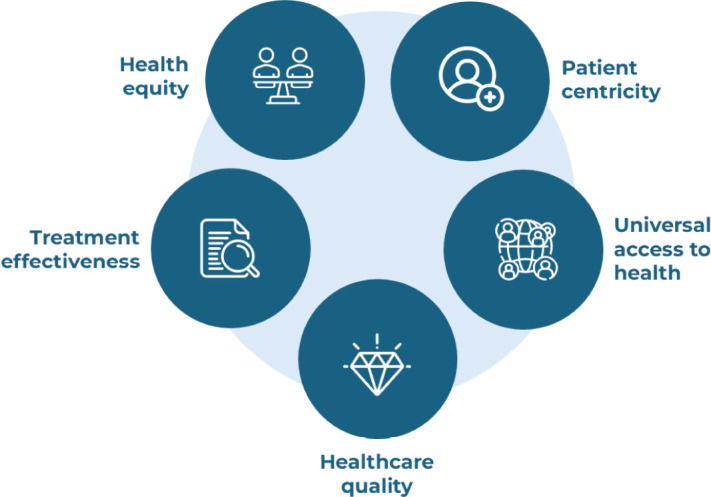 Figure 2
Figure 2 Figure 20
Figure 20 Figure 21
Figure 21 Figure 22
Figure 22 Figure 23
Figure 23 Figure 24
Figure 24 Figure 25
Figure 25 Figure 26
Figure 26 Figure 27
Figure 27 Figure 28
Figure 28 Figure 29
Figure 29 Figure 3
Figure 3 Figure 30
Figure 30 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7 Figure 8
Figure 8 Figure 9
Figure 9- —The authors disclose receipt of financial support from AstraZeneca for the research and the discussion process that was part of developing this document. AstraZeneca had no role in the conceptualisati
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEconomic and Financial Impacts of Cancer · Global Cancer Incidence and Screening
Introduction
Breast cancer (BC) was the most prevalent cancer in 2022, affecting over 8.1 million individuals worldwide [1]. It has a profoundly debilitating impact on patients and imposes substantial individual, societal and economic burdens. Despite significant advancements in BC research, diagnosis and treatment, substantial challenges persist. Access to optimal care remains limited, particularly in low- and middle-income countries (LMICs) [2]. Moreover, integrated, patient-centered approaches are not broadly available, with underserved populations facing the greatest barriers. These disparities highlight that challenges in BC care endure globally, leading to inequities both between and within countries [3–5].
Over time, significant efforts have been undertaken to guide and support countries in strengthening their national BC programs and service provision to improve patient outcomes, like for example, the Breast Health Global Initiative (BHGI) [6, 7] and the BC Initiative 2.5 (BCI2.5) [8, 9]. More recently, to achieve a 2.5% annual decrease in BC mortality rates at the global level, the World Health Organization (WHO) Global Breast Cancer Initiative (GBCI) provided evidence-based recommendations for countries to follow a phased approach to implementing interventions focused on improving BC early detection, diagnosis and treatment. The GBCI, which also describes the BC patient journey, identifies three evidence-based key performance indicators (KPIs) to pinpoint country-level gaps [2].
However, recent data indicate that only a few countries have achieved or are on track to achieve-the GBCI goal [5]. This suggests that further support might be needed to help countries more effectively and rapidly scale up their efforts to improve BC care.
A comprehensive approach aimed at reducing disparities and promoting equitable care for all individuals will require bold policy change in support of consistent, evidence-based practices and a two-pronged approach focused on increasing the existing healthcare system capacity while aligning rapid advancements in health technologies. Such an undertaking calls for expanding action on BC care and engaging a more diverse and comprehensive group of stakeholders to drive collaboration and shared responsibility.
To increase clarity around the required commitment and accountability for improving the quality of BC care and outcomes for all patients, we aspire for a new Breast Cancer Care Quality Index (BCCQI) to be integrated into National Cancer Control Plans (NCCPs). Building on the GBCI, the BCCQI will provide additional guidance on essential elements to enhance national-level BC care quality. The guidance provided should allow countries to tailor their own implementation plans to their specific needs and develop context-sensitive roadmaps to adapt over time as progress is achieved. This flexible and iterative approach encourages national ownership, supports inclusive participation and should facilitate incremental progress across five key domains essential to BC care improvement: health equity, patient centricity, universal access to health, healthcare quality and treatment effectiveness.
The objective of this document is to discuss the development of the BCCQI and facilitate alignment on its adoption and implementation as a strategic tool to advance BC care globally.
Methods
A two-part methodology was developed, adapted from the consensus approach [10], in which we aimed to gather general agreement on the key components to be included in the BCCQI, in order to address the limitations of empirical data supporting the impact and expected outcomes of commonly used metrics across real-world settings.
1. Parallel reviews to inform the preliminary framework
Peer-reviewed literature
A review of global evidence explored the multidimensional impact of BC, and the challenges and priority areas for quality improvement across the BC care continuum. We used Medical Subject Headings search terms on PubMed, including ‘breast cancer’, ‘breast cancer detection’, ‘breast cancer diagnosis’ and ‘breast cancer treatment’. The search was conducted between April 14th and May 24th, 2024. Target papers were identified based on their relevance to BC burden and challenges. Relevance to the BC burden was assessed based on evidence related to: (i) the disease burden, including BC incidence, mortality and disability-adjusted life years; (ii) the socio-economic impact, encompassing direct healthcare costs, out-of-pocket expenditures and productivity losses and (iii) the impact on the well-being of individuals and caregivers, including effects on physical and mental health, as well as on personal and professional relationships. Relevance to BC challenges was evaluated based on the extent to which the evidence addressed barriers encountered across the patient journey – from early detection and diagnosis to treatment, survivorship and recovery. A total of 89 papers were considered in the preliminary literature review.
Grey literature
Policy documents from governmental and international sources were reviewed to assess existing BC strategies, guidelines and recommendations and to identify potential areas for policy improvement.
United Nations (UN) resolutions and frameworks
Relevant UN health resolutions and frameworks were reviewed to shape the BCCQI’s structure (Box 1).
Based on the analysis of the literature, the BCCQI was aligned with the three pillars of the GBCI framework – health promotion, timely diagnosis and comprehensive treatment – as well as the patient pathway outlined within the GBCI.
A fourth dimension related to healthcare systems resilience was included as supported by literature review findings.
The parallel reviews provided valuable insights into the key issues the BCCQI should address, potential indicators for assessment, areas for policy improvement and the approach used by existing BC strategies. These findings informed the development of the preliminary BCCQI framework, with evidence justifying the inclusion of each target and indicator, which was subsequently refined through expert feedback.
2. Expert feedback
A multi-disciplinary group of 18 experts was consulted to provide key insights and feedback and to endorse the BCCQI through a three-phase feedback process. These experts were selected to ensure a comprehensive perspective on BC care, and with consideration for:
Affiliations and roles within reputable organisations dedicated to BC.Diverse range of geographic locations.Active engagement and participation in BC policymaking and guideline development.Active involvement in patient advocacy through international and regional organisations dedicated to BC and its care.Relevant publications and evidence of familiarity with the latest advancements in BC care.
Box 1.Example of UN-related frameworks reviewed to inform the Breast Cancer Care Quality Index (BCCQI).
- The 2030 Agenda for Sustainable Development
- The WHO Noncommunicable Disease (NCD) Global Monitoring Framework
- Monitoring and Evaluation of the Global Antimicrobial Resistance (AMR) Action Plan
- Indicator and Monitoring Framework for the Global Strategy for Women’s, Children’s and Adolescents’ Health
- Monitoring Framework for Universal Health in the Americas
The group comprised 11 experts selected for their experience as healthcare professionals, four as policymakers and public health specialists and three as patient and civil society representatives. It also included eight experts in medical and clinical oncology, with a strong focus on BC and four experts in breast surgery. A wide range of nationalities was represented, covering different regions. These included: four experts from the United States of America, two from Canada and one expert from each of the following countries: Argentina, Brazil, China, Egypt, Italy, Kenya, Malaysia, Mexico, Nigeria, Portugal, Puerto Rico and the United Arab Emirates. The expert feedback and validation process included:
Multistep expert preliminary feedback (May–July 2024)
This phase included a variety of engagement formats, including in-person and virtual advisory boards, as well as one-on-one meetings. During these sessions, experts discussed key challenges in BC care that the BCCQI should address and reviewed and endorsed the main structure of the preliminary BCCQI.
Following this round of discussions, a more refined second iteration of the Index was developed, supported by evidence justifying the inclusion of each target and indicator.
Pre-panel survey (October 2024)
In this pre-panel survey, experts were presented with the refined version of the BCCQI. For each indicator, they were asked to either validate it, validate it with modifications or indicate that it should not be validated. Additionally, they were encouraged to provide supporting evidence and sources as needed, addressing aspects such as the clinical and medical accuracy of the topics and the feasibility of data collection.
Following the pre-panel survey, the Index was refined and a third version was developed and supported by relevant literature.
Two expert panels (January 2025)
The panels were held to address outstanding issues in the near-final version of the BCCQI, in which experts could provide input and suggestions for further refinement. During these sessions, all outstanding issues achieved a minimum of 80% alignment among participants.
Following the two expert panels, the final version of the BCCQI was reached.
Manuscript development, validation and finalisation
The manuscript was developed concurrently with the expert validation process, summarising key findings from the literature review and the expert feedback process. Twelve experts who contributed to the full process for the development of the BCCQI are listed as co-authors of the manuscript.
Background and context
Breast cancer: biological, clinical, epidemiological and socioeconomic perspectives
Breast cancer is the most common cancer among women in most countries and represents an important cause of premature mortality globally [2]. It imposes a staggering burden, straining healthcare systems, impacting the quality of life for patients and their families and with a great socioeconomic cost. The International Agency for Research on Cancer (IARC) estimates nearly 2.3 million new BC cases and 700,000 deaths globally in 2022 [1, 11], with 10.7% of new cases occurring in people aged less than 40 years [12]. In the absence of bold action, the burden of BC is projected to increase to 3.19 million cases by 2040, with around 1.04 million deaths per year [11]. Globally, it has been estimated that BC had an economic cost of 1.964 trillion international dollars in 2017 [13]. Beyond the economic strain and impact on productivity, BC itself and its treatment profoundly affect patients' psychosocial well-being and physical health. BC patients have an increased risk of mental health conditions such as depression and anxiety compared to individuals without BC [14, 15]. In addition, BC is associated with social stigma, along with self-stigma and associative stigma affecting family members, due to the value placed on women’s reproductive capacity or marital status [16]
The causes of BC are poorly understood, and most identified risk factors are not amenable to change [17]; therefore, improvements in early detection, timely diagnosis and comprehensive management are crucial to reducing mortality rates, enhancing patient quality of life and alleviating the economic and social burdens associated with this disease [2].
A recent study highlighted that countries with the highest human development index (HDI) show the highest age-adjusted BC incidence rates but the lowest BC mortality rates. Conversely, the countries with lower HDI scores have the lowest incidence but the highest BC mortality rates [5]. In addition, projections indicate that, between 2022 and 2050, BC incidence and mortality will increase more sharply in regions with limited resources [5].
The disproportionately greater mortality faced by LMICs might be affected by country-specific factors, like population structure, lifestyle, genetic factors and environment [18, 19].
Certain groups of women may face higher risks of developing BC, or of developing it at a younger age or experience more aggressive forms of the disease. For example, Ashkenazi Jewish women are at a significantly higher risk of developing BC than other Caucasian women [20, 21]. Within this group, a family history of BC further amplifies the risk, especially for early-onset disease. Similarly, African, Asian and Hispanic/Latina women are more likely to be diagnosed with BC at younger ages compared to their White or Western counterparts [19, 22–26].
However, access to and quality of BC detection, diagnosis and treatment services [27, 28] are also significant drivers of the inequities observed, as shown for example by the striking difference in BC stage at diagnosis, with only about 5%–10% of patients with metastatic BC at initial diagnosis in high-income countries (HICs), compared to up to 50%–80% of patients diagnosed with de novo stage III/IV BC, in LMICs [16, 29–31].
Breast cancer patient journey
The GBCI framework outlines the BC patient journey through three pillars, each corresponding to sequential patient-care intervals, as illustrated in Figure 1. For each pillar, the WHO provides a detailed description of the relevant interval, including the associated processes, interventions and the desired outcomes, which serve as benchmarks for countries to aspire to in improving BC care [2].
Challenges in BC care: findings from the literature review
Numerous challenges affect the quality of the BC care delivered at the country level. These challenges are often particularly pronounced in LMICs and among vulnerable populations that are more significantly impacted by access barriers, leading to worse patient outcomes [16, 29, 30, 32]. Table 1 presents key challenges identified along the BC patient journey in the initial literature review.
Based on the challenges described above, our analysis led to the identification of the following four dimensions: early detection, timely diagnosis, comprehensive management and strong and resilient healthcare systems.
Early detection and timely diagnosis are vital for reducing BC mortality; analysis of evidence from 1990 to 2020 showed that only countries detecting at least 60% of the invasive cancers at stages I or II achieved a 2% reduction in BC mortality for three consecutive years [2]. Timely diagnosed BCs are treated more effectively, with treatment being better tolerated and less costly [2]. Comprehensive care combines timely cancer therapies (surgery, radiotherapy and systemic treatments) and supportive services, following WHO guidelines and international standards, to ensure holistic BC management, improve patient outcomes and enhance quality of life. Strong, resilient healthcare systems are essential to meet the growing BC burden while ensuring quality, equity and patient-centered care across the BC patient journey [53, 62, 63].
Results
Importance of a BC care quality index
Breast cancer is a public health priority for health systems and countries worldwide, given its significant impact on patients, families, health systems and society overall. However, countries are tasked with the challenging responsibility of addressing patients’ healthcare needs while ensuring the economic sustainability of their healthcare system [64, 65]. Considering the projected growing burden of BC, this task appears even more daunting.
To support these efforts, a multitude of initiatives and organisations have focused over the years on providing guidance for countries, healthcare systems and individual healthcare institutions, on how to ensure the quality of BC services and how to develop programs and interventions to successfully improve outcomes of BC patients (Box 2).
In 2021, the WHO, in collaboration with the International Atomic Energy Agency (IAEA) and the IARC, [70] launched the GBCI which aims to provides national program managers, policymakers and multisectoral stakeholders the valuable guidance they need to assess gaps, strengthen and scale-up services for the early detection, diagnosis and management of BC [2]. The GBCI framework’s objective is to reduce BC mortality by 2.5% per year and save 2.5 million lives over a 20-year period [2]. For this purpose, the GBCI identified essential KPIs that countries should adopt to measure progress.
Box 2.Overview of key initiatives driving quality improvement in BC care through evidence-based guidelines, scalable care models and clinical frameworks.The BHGI, founded in 2002, sought to improve breast health care and cancer treatment for women in economically disadvantaged countries, [66] by crafting and applying evidence-based guidelines, specifically developed and adapted for enhanced feasibility and contextual appropriateness [6, 7]. In collaboration with critical players, the BHGI defined best practices and created consensus guidelines for BC early detection, diagnosis, treatment, healthcare systems and public policy [6]. The BCI2.5, founded in 2014, aims to promote evidence-based care models for early detection, diagnosis, treatment and supportive care that can be scaled up when and where needed, providing regional leaders with analytics, assessment and planning tools, educational materials and implementation science research [8, 9]. Critical tools developed include Breast Health Care Assessment Questionnaire and Knowledge Summaries, which are used for baseline assessments and situation analyses, in partnership with countries or centers of excellence [8]. The BCI2.5 also developed a phased implementation model of an evidence-based framework to improve breast health care delivery in LMICs, which is being implemented in Brazil, Peru and Tanzania [67, 68].Guidance from a strictly clinical perspective is provided through quality indicators outlined in various documents, including CPGs, integrated BC healthcare processes, clinical pathways and position papers [69]. This guidance is valuable not only for individual institutions but also serves as a framework for countries to assess and regulate the overall quality of BC services at the clinical level.
However, recent data show that only seven of the most developed countries are meeting, and six additional countries are close to meeting, the GBCI goal of 2.5% annual decreases in BC mortality rates [5]. This outlines a possible gap with countries requiring further support and guidance on a set of more practical and applicable essential measures to consider to more effectively and rapidly scale up action for improved BC care.
Building on the GBCI and previous global initiatives, the BCCQI proposes a unified framework that outlines essential elements for countries to prioritise in order to enhance BC care quality at the national level. By providing a structured set of targets and indicators, this framework enables countries to develop tailored implementation strategies, adapted to their specific contexts and create actionable roadmaps to address gaps in BC care.
Unlike rigid, prescriptive models or ‘one-size-fits-all’ approaches of the past, the BCCQI seeks to promote a flexible, context-sensitive approach, empowering countries to set their own short- and medium-term priorities. In doing so, countries are encouraged to leverage existing guidance from initiatives such as the GBCI and other resource-stratified frameworks. Recognising that no country has fully addressed all barriers to optimal BC care, the BCCQI helps nations identify specific areas for improvement. Some may focus on enhancing healthcare professionals knowledge and education, while others may work to improve access to supportive services that enhance patient-centered care. Because the framework is designed as a continuous, inclusive process, countries can refine their priorities and strategies iteratively, making stepwise enhancements based on local challenges and opportunities. In this way, countries with immediate limited investment capacities or differing priorities can still advance toward meaningful progress. This flexibility fosters a sense of ownership among national stakeholders, allowing each country to make strategic decisions aligned with their specific situation.
In addition, to ensure that improvements are truly impactful for patients, the BCCQI centers on five key domains essential for high-quality BC care: health equity, patient centricity, universal health access, healthcare quality and treatment effectiveness (Figure 2 and Box 3).
By emphasising the importance of national policies and strategies, the BCCQI is designed to drive bold policy reforms that establish essential national frameworks. These frameworks will empower countries to sustainably strengthen healthcare system capacity while striving to keep pace with rapid advancements in BC clinical practice.
Given the scale of the challenge, no single stakeholder can drive this transformation alone. The BCCQI is intended to serve as a catalyst for collective action by uniting key actors around a comprehensive set of actionable targets and indicators. This shared framework helps expand and clarify responsibilities, enhances accountability and fosters a sense of ownership among national stakeholders when prioritising actions and measuring progress toward the GBCI goals.
Finally, over time, by supporting the harmonisation of progress tracking, as outlined by previous initiatives [71, 72], the BCCQI is expected to facilitate the generation of comparable global evidence. This will enable intercountry comparisons, trend identification and cross-country learning – critical information for policymakers seeking to refine existing frameworks and develop targeted interventions. Ultimately, this is expected to support decision-making, increased stakeholder engagement and advocacy and enhanced accountability, ensuring continued global progress toward the highest standards of BC care.
Box 3.Definitions of the key domains for improvement prioritised by the Breast Cancer Care Quality Index (BCCQI).
- Health equity: Describes the state in which everyone has a fair and just opportunity to attain their highest level of health. This involves removing obstacles to health such as poverty, discrimination and their consequences, including lack of access to good jobs with fair pay, quality education and housing, safe environments and health care [73, 74].
- Patient-centered care: Is achieved when services provided reflect the patient's preferences, needs and values [75]. This approach ensures that patient values guide program and service planning, as well as clinical decisions, emphasising the importance of effective communication, pain management, clear care plans and a comfortable environment.
- Universal health coverage (UHC): Means that all individuals and communities receive the health services they need without suffering financial hardship. It includes the full spectrum of essential, quality health services, from health promotion to prevention, treatment, rehabilitation and palliative care [76–79].
- Healthcare quality: Is the degree to which healthcare services for individuals and populations increase the likelihood of desired health outcomes. It encompasses six domains: safe, effective, patient-centered, timely, efficient and equitable care [80, 81].
- Treatment effectiveness: Is the likelihood that a certain treatment protocol will benefit patients in a certain clinical population when administered in clinical practice [82].
Breast Cancer Care Quality Index
The BCCQI aims to increase action and implementation of healthcare system transformation to improve BC care for all patients, highlighting key elements that each country should focus on to advance the quality of BC care. The BCCQI represents a catalyst for engagement for policymakers, the international community and multisectoral stakeholders. Box 4 provides an overview of key principles that were followed during the conception of the BCCQI to ensure its robustness and maximise the likelihood of its successful adoption.
The BCCQI is structured into dimensions, goals, targets and indicators, mirroring the structure of key outcome-driven health-related frameworks established by international organisations and their collaborators. Box 5 provides more information regarding their development.
Each target and its supporting indicators have been designed to facilitate advances in the key domains of BC care improvement: health equity, patient centricity, universal access to health, healthcare quality and effectiveness of treatment (Figure 2 and Box 3).
Box 4.Key guiding principles of the Breast Cancer Care Quality Index (BCCQI).(1) The BCCQI framework was developed in alignment with global health policy priorities and conventions to facilitate its adoption by policymakers (2). Through an inclusive collaboration and co-creation process, it ensures balanced representation and shared ownership among stakeholders, adhering to internationally recognised best practices (3). Designed to be both pragmatic and effective, the framework prioritises essential elements to enhance BC care quality globally. To promote fairness and equity, it emphasises inclusivity, ensuring that no population or individual is marginalised (4). Furthermore, to enhance its applicability across diverse settings, the framework has been built in consideration of a broad spectrum of evidence from various country contexts and income levels (5). Finally, the BCCQI is conceived as a flexible, iterative tool, allowing countries to adapt its implementation to their specific priorities and develop context-sensitive roadmaps.
Box 5.Methodological information regarding the development of the goals, targets and indicators of the Breast Cancer Care Quality Index (BCCQI).The dimensions were identified through an in-depth review of the existing literature and are strongly supported by prior work on BC. The goals outline broad objectives, defining the desired achievements within each dimension. Targets specify measurable outcomes with defined timeframes, articulated through clear statements or quantitative benchmarks.Indicators are the metrics used to monitor progress, assess gaps and measure advancement toward Targets. Achieving these targets is expected to help fulfil the overarching goals.The dimensions are aligned to the three pillars of the GBCI framework: (1) early detection; (2) timely diagnosis and (3) comprehensive BC management. A fourth dimension that underlies the continuum of care and poses many challenges to the delivery of optimal BC services was strongly supported by the literature review findings. This dimension focuses on strong and resilient healthcare systems [2, 16].The goals associated with each dimension were defined in accordance with the GBCI framework, the patient pathway presented in the GBCI framework and analysis of peer-reviewed literature.The targets under each dimension were set and defined based on the analysis of each pillar during discussions with experts, the patient pathway presented in the GBCI framework and peer-reviewed literature [2, 16, 83, 84].Finally, one or more indicators were built to translate each Target into measurable metrics. Indicators are categorised into ‘Structure, Process, Outcome’, following Donabedian's quality of care model [85], in which structure is defined by the attributes of the settings in which care is provided, process by the provision of care itself and outcome by the measurable change in the health status of the patient. Some adaptations of this model, shown in Table 2 below, were made to ensure the BCCQI is practical and easily implementable across countries, minimising hurdles that could impede its adoption.
As discussed above, when seeking to improve BC patients’ care, every country would need to identify its medium–short term priorities to advance specific targets and indicators of the BCCQI, based on the country context, including challenges and opportunities.
Table 3 summarises the BCCQI targets and indicators by dimension, including the domains each indicator contributes to enhancing. Additional information regarding each target and indicator is provided in the Supplementary Tables S1 and S2.
Discussion
The BCCQI provides an opportunity to promote renewed attention and focus on health care and mobilising new streams of funds for BC care. It is envisioned as a dynamic tool, subject to continuous refinement and improvement based on real-world application and evolving evidence. As a flexible and adaptable framework outlining essential elements for assessing and improving the quality of care for BC patients across the care continuum, it promotes stakeholder ownership and accountability at all levels [86], empowering countries to drive iterative improvements through context-specific roadmaps aligned with local needs, opportunities and challenges. Moving beyond the prescriptive, rigid models of the past, it encourages action through an inclusive and continuous process that recognises incremental progress. This allows countries to address public health challenges at their own pace and has the potential to serve as a replicable model for advancing care in other critical disease areas. Ultimately, this approach brings countries closer to fulfilling the three pillars of the GBCI framework, providing additional guidance and more practical and applicable details to help them reduce BC mortality and address its broader societal impact.
The essential domains that guided development of the BCCQI serve to enhance alignment of the framework with the international community’s global health priorities, like as example, the 2030 Agenda for Sustainable Development. Additionally, in the lead up to the fourth UN high-level meeting on noncommunicable diseases (NCDs), the BCCQI presents an opportunity for the cancer and BC communities to push for reprioritisation of an unfinished agenda. The marked alignment of the BCCQI with other global health priorities, such as universal health coverage and non-communicable disease management, guarantees that policymakers can more easily secure the necessary political and financial support due to this synergy with ongoing efforts at the country and global level.
As seen in previous disease-specific programs, foundational frameworks can often serve as a platform for broader service integration, yielding benefits that extend beyond their original scope [86–88]. Similarly, the BCCQI framework has the potential to generate positive spillover effects that enhance the overall strength and resilience of national healthcare systems. This is particularly relevant for the BCCQI, which directly focuses on overall healthcare system strengthening by dedicating a full dimension to integral healthcare system components.
By incorporating metrics related to governance, financing, resource allocation, service organisation and results, this framework is fully geared towards ensuring that impact and advances in overall healthcare system capacity can be systematically recorded and monitored. Monitoring and evaluation should indeed become a pivotal component of any BC planning and implementation effort, as outlined by previous initiatives [71, 72]. The fact that the BCCQI already provides a general reference aids countries in setting a starting point to begin recording the baseline, in support of BC and healthcare system performance assessment and improvement over time.
Yet, several challenges must be understood and mitigated to ensure the successful adoption of the BCCQI. First and foremost, the perception that BC is an already addressed need might reduce the willingness of policymakers to continue working on it.
In addition, the inadequate public awareness and the lack of robust advocacy movements further hinder the prioritisation of BC as a key health issue. There is also a lack of comprehensive data, as many countries face gaps in national cancer staging, timely diagnosis and treatment completion data, which leads to a lack of agreement on critical aspects of BC care. More specifically, for example, in LMICs, there are critical evidence gaps in building the case for comprehensive BC management services, especially when considering the full spectrum of the desirable supportive services to be offered. These gaps pose remarkable challenges for countries with limited capacity to invest in data infrastructure development in the short-medium term but, on the other hand, offer them the opportunity to leverage the index as a tool for broader awareness creation, resource mobilisation and collaborative action for iterative progress.
Finally, financial, infrastructural and human resource constraints, along with competing priorities within and beyond healthcare systems, pose substantial barriers to the adoption of the BCCQI.
As we look ahead, sustained collaboration among governments, the international community and multisectoral stakeholders will be essential to driving continuous progress in addressing growing healthcare needs worldwide. By offering a unified framework for action and fostering inclusivity and adaptability to support decision making, the index empowers countries and multisectoral stakeholders to develop and advance tailored efforts to bridge gaps in BC care. Collaboration will be especially valuable in advancing data infrastructure needs and pilot programs to field test and further refine the BCCQI, which is conceived as a dynamic tool that, once adopted, will be subject to ongoing refinement and future improvements based on real-world application and evolving evidence. In this regard, key opportunities for immediate action, which are ultimately expected to have positive repercussions on the broader healthcare system and global health, have been pinpointed in the recommendations.
Limitations
The methodology used in this study, which includes a review of peer-reviewed literature, grey literature, UN resolutions and frameworks and an expert feedback process, guided the development of the BCCQI as an expert-endorsed tool designed to drive actionable, systematic healthcare transformation and improve the quality of BC care for all patients. However, the HIC-bias of grey literature and CPGs may represent a limitation of the tool.
This geographic concentration may not fully capture the unique challenges and resource constraints faced by LMICs. However, the inclusion of peer-reviewed literature from countries across diverse regions and development levels helps mitigate this limitation by incorporating a broader range of perspectives. Future iterations of the BCCQI could further enhance its comprehensiveness and generalisability through a systematic review of the existing evidence.
The expert feedback process, although robust and multidisciplinary, reflects the perspectives of a selected group of professionals. While this could potentially limit the generalisability of findings, the experts consulted for this study were carefully chosen based on their affiliations and roles within reputable organisations dedicated to BC, extensive experience in oncology and related fields and active engagement and participation in BC policymaking and guideline development.
Moreover, their representation from a diverse range of geographic locations and healthcare systems reinforces the global applicability of the BCCQI.
Finally, while the metrics outlined in the BCCQI are derived from evidence, they have not been field-tested. The primary goal of this study is to initiate meaningful discussions on the development of the BCCQI as a global tool to be adopted in NCCPs. It is intended to represent, despite its limitations, a first attempt at developing such a framework at the global level and to lay the foundation for following iterations as more evidence becomes available. However, it is important to recognise that incorporating the BCCQI into NCCPs does not guarantee better patient outcomes and higher quality care delivery, as clear evidence of the impact of similar frameworks in key governance documents at the national level is still missing.
Recommendations
The BCCQI serves as a catalyst for unifying stakeholder efforts and accelerating global progress in BC care by building on existing initiatives and maximising the impact of prior investments. It offers a clear, actionable and adaptable framework focused on key dimensions, including early detection, timely diagnosis, comprehensive management and healthcare system resilience. However, while adopting as part of NCCPs and implementing the BCCQI stands as a key recommendation, existing challenges may hinder global commitment to its success. To this end, policymakers, international organisations and stakeholders across sectors play a critical role in building momentum and fostering broad engagement toward a strong global partnership striving to guarantee that the BCCQI becomes a pivotal tool to ensure that all BC patients have access to the highest standards of care.
To advance this objective, the following recommendations are proposed (Box 6).
Box 6.Recommendations. Recommendations for policymakers
- Leverage upcoming international platforms to advocate for renewed international commitment to the unfinished BC agenda: Maximise opportunities created by major global gatherings, such as the UN high-level meeting on NCDs, to elevate the unfinished BC agenda and garner support for implementation of the BCCQI.
- Support integration of the BCCQI into National Cancer Control Plans by emphasising the BCCQI’s alignment with the UN global health agenda and specific sustainable development goals, such as SDG 3.4 (reducing premature mortality from NCDs) and SDG 3.8 (achieving universal health coverage): Emphasise the BCCQI’s alignment with the UN global health agenda and specific sustainable development goals, such as SDG 3.4 (reducing premature mortality from NCDs) and SDG 3.8 (achieving universal health coverage), and encourage governments to champion a UN-led initiative to improve BC care globally by integrating the BCCQI into NCCPs.
- Promote cross-sector and supranational collaboration for BCCQI implementation to tackle key barriers, including resource allocation, data collection and monitoring systems: Foster alliances among governments, NGOs, healthcare institutions and the private sector to leverage expertise and mobilise the resources needed for the implementation of the BCCQI.
- Prioritise BC public education and awareness to create the demand for adoption and implementation of the BCCQI: Promote comprehensive awareness programs and campaigns to reduce stigma and fear surrounding BC. Leverage existing platforms and channels, like advocacy networks and international days and events, to amplify public support for improved BC care and increase endorsement for the BCCQI.
- Build the economic case for investment in coordinated global efforts to improve BC care, reduce inequities and promote new funding stream: Work with multisectoral stakeholders to generate the necessary evidence in support of continued investments in BC care and mobilise both traditional and innovative funding streams to facilitate the implementation of the BCCQI.
- Support phased national adoption of the BCCQI by developing context and resources -specific pathways for implementing the BCCQI: Develop context-specific pathways for implementing the BCCQI. Prioritise key areas of improvement based on available resources, opportunities and challenges, and gradually expand efforts as capacity grows. When necessary, set up pilot programs to test feasibility and scalability before nationwide rollout.
Recommendations for the international community
- Leverage the BCCQI to galvanise Member States and trigger renewed actions for improved BC care quality in support of the GBCI framework: Build on stakeholders’ activities and harness the momentum of the BCCQI to ignite enthusiasm and drive faster progress in improving BC care quality worldwide. Foster collaborative actions and interactions, encouraging cross-pollination between WHO/UN-led initiatives and externally driven efforts as a model for action that could be expanded to other disease areas in the future.
- Strengthen global coordination, knowledge sharing and synergies with the WHO initiatives: Foster collaboration among stakeholders by aligning efforts with the GBCI framework and leveraging key resources such as the WHO Patient Navigation Toolkit, the WHO Noncommunicable Disease Facility-Based Monitoring Guidance and the WHO–IAEA Framework for Setting Up a Cancer Centre. Actively encourage stakeholders and Member States to maximise these tools while promoting international knowledge-sharing platforms to facilitate peer-to-peer learning, avoid duplication of efforts and accelerate country progress in BCC quality worldwide.
- Promote renewed focus and attention on BC across upcoming global platforms: Ensure that upcoming global appointments, such as the UN High-Level Meeting on NCDs, prioritise discussions on the unfinished BC agenda. Advocate for dedicated attention to BC care, emphasising to Member State its urgency and alignment with key commitments, including the 2030 Sustainable Development Agenda—particularly SDG 5 (gender equality) and SDG 10 (reducing inequalities).
- Support member States’ initiatives and actions to accelerate country-level progress on improved quality of BC care delivered: Offer support and provide technical assistance for countries seeking to adopt and implement the BCCQI. Promote the development of research networks and collaborations that focus on scaling successful models and monitoring BCCQI implementation.
- Enhance international and multisectoral cooperation for resources mobilisation and expansion: Promote cross-sector partnerships to address key barriers related to resource availability, by fostering collaborations between governments, NGOs, healthcare institutions and the private sector. Promote the expansion of traditional funding initiatives and facilitate the exploration of innovative solutions to support countries in implementing the BCCQI, with particular focus on low- and middle-income countries.
- Support research and country-level evidence generation to accelerate progress in the quality of the BC services delivered: Strengthen efforts to improve data collection systems, emphasising the importance of investments in robust and sustainable data gathering and analysis mechanisms to measure progress against BCCQI indicators and identify gaps and disparities to generate actionable, context-specific evidence and inform policy and program evaluation and adaptation.
- Assist BC stakeholders’ monitoring and evaluation efforts: Build on existing international data gathering and monitoring initiatives, like IARC CanScreen 5 and IARC CanReg 5, to expand BC related data gathering and analysis. In support of these initiative, consider the establishment of an international multistakeholder mechanism, modeled after the Global Coordination Mechanism on NCDs, to enhance commitment and global accountability for standardised data reporting to enable inter-country comparisons and generate global evidence on BC care.
Recommendations for multisectoral stakeholders
- Scale up advocacy towards policymakers for enhanced efforts to improve BC care and adoption of the BCCQI: Advocate at the national level to ensure that BC remains or becomes a priority. Highlight the significant gaps, the growing burden and the societal impact and cost of BC, supporting policymakers in making the case for continued investment, even in well-resourced settings. Urge adoption and implementation of the BCCQI as a way to improve the quality of BC care provided at the national level and globally.
- Join forces at the international level to build momentum for the BCCQI and renewed BC attention: Collaborate with partners at regional and global levels to ensure visibility of the current gaps and challenges faced by BC patients and in providing quality BC diagnosis and management. Use discussions and side events of key fora, like for example the World Health Assembly, the UN General Assembly and the UN High-level Meeting on NCDs, to raise awareness about the need to ramp up efforts for BC and foster international collaboration for a joint UN-resolution on BC and the adoption of the BCCQI.
- Foster support and commitment for BC and the BCCQI as part of broader global health and sustainable development efforts: Emphasise how the BCCQI aligns with the broader sustainable development agenda – especially with SDG 3.4 (reducing premature mortality from NCDs), SDG 3.8 (achieving universal health coverage), SDG 5 (gender equality) and SDG 10 (reducing inequalities) – as well as with prominent ongoing efforts by the WHO and other UN-related agencies, e.g., the GBCI framework, IARC CanScreen 5 and CanReg 5. Call upon the international community to continue advancing initiatives that promote inter- and intra-country equity in BC care.
- Participate in international platforms and collaborative initiatives: Support efforts championed by the international community to promote the BCCQI by contributing with expertise, information and resources as needed. For example, commit to support standardised data reporting from the country level to key global BC-related initiatives and platforms, like for example IARC CanScreen 5 and CanReg 5.
- Expand advocacy, education and capacity-building efforts in support of BC awareness and BCCQI implementation: Intensify advocacy and capacity-building initiatives directed toward the general public, peer advocates and healthcare workers at the regional and national levels. Strengthen awareness, build support and activate grassroots movements for the adoption and implementation of the BCCQI as a way to reduce disparities and improve BC outcomes locally and globally.
- Leverage synergy and alignment with other initiatives to expand efforts and partnerships: Collaborate with partners and stakeholders at every level to integrate BC care into broader health system strengthening and development efforts, such as those focused on universal health coverage, non-communicable disease management and addressing global inequities.
- Strengthen evidence-generation efforts to monitor and evaluate progress in the quality of BC care: Leverage collective expertise, technological resources and financial capacity to build a compelling case for scaling up initiatives. Learn from successful examples of previous and ongoing efforts, such as the global burden of disease (GBD), Globocan and Concord, to promote coordinated and synergistic evidence-generation activities at both regional and global levels.
- Engage financial actors to support effective fund mobilisation: Foster discussions with economic institutions and financial stakeholders to explore new opportunities for resource mobilisation, including innovative financing mechanisms and successful initiatives. Support policymakers and the international community in their efforts to mobilise and expand resources for BC care and implementation of the BCCQI.
Conclusion
Significant disparities in BC access and quality of care persist globally, including within HICs, highlighting the urgent need for a unified framework that supports all countries in advancing BC care, regardless of their context, resources, infrastructure or specific challenges. The Breast Cancer Care Quality Index (BCCQI) offers countries the guidance they need to design results-driven approaches supported by evidence to tackle their respective challenges at their own pace.
The global action to combat BC calls for coordinated and effective measures that streamline efforts, reduce unnecessary duplication and address existing gaps in care. In this spirit, it is important to emphasise that the BCCQI has been thoughtfully designed to further support and strengthen action under the GBCI and other relevant initiatives by providing more detailed metrics that countries can adopt in a context-specific manner. Rather than competing, it acts as a valuable tool to help operationalise the general guidance applicable to broad country groups provided by existing initiatives such as the GBCI framework, deepening their impact by empowering countries to develop their own tailored roadmaps for implementation.
In the lead-up to the UN high-level meeting on NCDs in September 2025, this framework presents an opportunity to drive renewed attention to BC care and mobilise new funding streams to enhance its quality at the global level. However, the successful adoption and implementation of the BCCQI requires multisectoral collaboration and coordinated action to overcome multiple barriers. It is envisioned that, by establishing clear benchmarks to be tracked through regular audits for the refinement of its implementation, integration of the BCCQI into NCCPs can enable more systematic efforts towards strong governance, sustainable financing and robust data collection and analysis systems.
Future studies can explore the implementation process of the BCCQI, and field-test the index to refine it, validate its metrics and ensure its relevance and reliability across different contexts. This will help make the BCCQI more evidence-based and context-validated.
By providing a tool for coordinated action at the global, national and regional levels, the BCCQI has the potential to serve as a catalyst for enhanced efforts towards more equitable and sustainable BC care worldwide. Its adoption and effective implementation are expected to lead to higher quality, patient-centered services globally, ultimately improving BC care for all patients, regardless of geographic or economic barriers.
Conflicts of interest
BOA declares consulting fees from AstraZeneca as Global Oncology Consultant (2024–25).
GC declares consulting fees from BMS, Roche, Pfizer, Novartis, Lilly, AstraZeneca, Daiichi Sankyo, Merck, Seagen, Ellipsis, Gilead and Menarini; is a speakers’ bureau member for Lilly, Pfizer, Relay, Gilead, Novartis and Menarini; and received support for attending meetings/travel from Daiichi Sankyo.
SS received speaking fees and participated in advisory boards for Novartis, Gilead, Lilly, Roche, AstraZeneca, Daiichi Sankyo, Knight, Merck, Bristol Myers Squibb, Incyte and Sandoz.
FC holds consultancy roles with Amgen, Astellas/Medivation, AstraZeneca, Bayer, Celgene, Daiichi Sankyo, Eisai, GE Oncology, Genentech, Gilead, GlaxoSmithKline, IQVIA, MacroGenics, Medscape, Merck Sharp & Dohme, Merus BV, Mylan, Mundipharma, Novartis, Pfizer, Pierre Fabre, prIME Oncology, Roche, Sanofi, Samsung Bioepis, Seagen, Teva and TouchIME; is the President of the ABC Global Alliance, Chair of the ABC Consensus Conference and Guidelines, and a Fellow of the European Academy of Cancer Sciences; and is a member or committee member of ESMO, ESO, ASCO, AACR, ECO, AORTIC, UICC, EORTC, IBCSG, SOLTI, EACR, SIS, ASPIC, SPO and EVITA.
ARG reports being the CEO of Policy Wisdom LLC.
ES received travel grants from Boehringer Ingelheim, Hikma, Janssen, Lilly, Merck Sharp & Dohme, Mundipharma, Novartis, Pfizer and Roche; participated in advisory board meetings, consultancy and/or speakers’ bureaus for Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Clinart MENA, Genomics Genetics, GSK, Hikma, EVA Pharma, Janssen, Lilly, Merck Sharp & Dohme, Mundipharma, Nebridge Pharmaceutical, Novartis, Pfizer, Pierre Fabre, Roche and Sandoz; and has been involved in clinical trials for AstraZeneca, Boehringer Ingelheim, Novartis, Pfizer and Roche.
CHY declares payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from Novartis; and participation on a Data Safety Monitoring Board or advisory board for AstraZeneca.
AM declares consulting fees from Roche and Eli Lilly; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from Merck, Roche, Eli Lilly and AstraZeneca; and received support for attending meetings and/or travel from Roche.
YCG received research support from Roche and Pfizer; participated in speakers’ bureaus for Gilead, AstraZeneca, Lilly and Merck Sharp & Dohme; received support for travel expenses from Novartis, Pfizer, Gilead and Lilly; and holds an advisory role with AstraZeneca.
EC, MM, YY, JVR, IL and NS declare no competing interests.
EC, BOA, GC, SS, FC, ES, AM, YCG and YY received honoraria for their involvement as expert panel members. MM’s honorarium was allocated in support of the Kenya Society of Hematology and Oncology (KESHO). The participation of JVR, IL and NS was covered through their regular roles at Policy Wisdom LLC.
Author contributions
Conceptualisation- Formulation: IL, NS.Conceptualisation- Evolution: EC, BOA, GC, SS, FC, ARG, ES, CHY, AM, YCG, MM, YY.Data curation: JVR, IL.Formal analysis, data adaption to real world experience, data interpretation: EC, BOA, GC, SS, FC, ARG, ES, CHY, AM, YCG, MM, YY, JVR, IL, NS.Investigation: EC, BOA, GC, SS, FC, ARG, ES, CHY, AM, YCG, MM, YY, JVR, IL, NS.Methodology- Original: JVR, IL, NS.Methodology- Refinement and adaptation: EC, BOA, GC, SS, FC, ARG, ES, CHY, AM, YCG, MM, YY.Index Endorsement: EC, BOA, GC, SS, FC, ARG, ES, CHY, AM, YCG, MM, YY.Project administration: NS.Supervision: NS.Writing – original draft: JVR, IL.Writing – review & editing: EC, BOA, GC, SS, FC, ARG, ES, CHY, AM, YCG, MM, YY, NS.
Data sharing statement
Not applicable.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1International Agency for Research on Cancer Global Cancer Observatory – World. Cancer Today 202429/02/24Lyon International Agency for Research on Cancer[Fact sheet] [Internet] [https://gco.iarc.who.int/media/globocan/factsheets/populations/900-world-fact-sheet.pdf]
- 2World Health Organization Global Breast Cancer Initiative Implementation Framework: Assessing, Strengthening, and Scaling Up of Services for the Early Detection and Management of Breast Cancer 202313/05/24Geneva World Health Organization[Internet] [https://www.who.int/publications/i/item/9789240065987]
- 3Barrios CH Global challenges in breast cancer detection and treatment Breast 202262 S 3S 610.1016/j.breast.2022.02.00335219542 PMC 9097801 · doi ↗ · pubmed ↗
- 4Wilkerson AD Gentle CK Ortega C Disparities in breast cancer care – how factors related to prevention, diagnosis, and treatment drive inequity Healthcare 202412446210.3390/healthcare 1204046238391837 PMC 10887556 · doi ↗ · pubmed ↗
- 5Kim J Harper A Mc Cormack V Global patterns and trends in breast cancer incidence and mortality across 185 countries Nat Med 202510.1038/s 41591-025-03502-339994475 · doi ↗ · pubmed ↗
- 6Anderson BO Cazap E Breast health global initiative (BHGI) outline for program development in Latin America Salud Publica Mex 200951 s 309s 31510.1590/S 0036-3634200900080002219967287 · doi ↗ · pubmed ↗
- 7Fred Hutch Cancer Center Breast Health Global Initiative (BHGI)202004/02/25Washington Fred Hutchinson Cancer Center[Internet] [https://www.fredhutch.org/en/research/divisions/public-health-sciences-division/research/epidemiology/breast-health-global-initiative.html]
- 8Fred Hutch Cancer Center Breast Cancer Initiative 2.5 (BCI 2.5)201404/02/25Washington Fred Hutchinson Cancer Center[Internet] [https://www.fredhutch.org/en/research/divisions/public-health-sciences-division/research/epidemiology/breast-cancer-initiative-2-5.html]