Comparison analysis of serum interleukin-6 levels and cervical cancer
Muisi A Adenekan, Joseph B Minari, Ayodeji Adefemi, Gbenga Olorunfemi, Ayomide I Fayinto, Adebayo Sekumade, Temitope V Adekanye, Adeyemi A Okunowo, Kehinde S Okunade

TL;DR
This study found that cervical cancer patients have significantly higher serum IL-6 levels compared to cancer-free women, suggesting IL-6 could help diagnose and monitor the disease.
Contribution
The study provides new evidence on elevated IL-6 levels in cervical cancer patients from sub-Saharan Africa, highlighting its potential as a diagnostic and prognostic biomarker.
Findings
Cervical cancer patients had a 214.9 ng/mL higher serum IL-6 level than cancer-free women (p = 0.007).
IL-6 levels were significantly higher in advanced-stage cervical cancer and in squamous cell carcinoma cases.
A serum IL-6 cut-off of 365.1 ng/mL showed good discriminatory ability for cervical cancer diagnosis.
Abstract
We found a significant increase in serum IL-6 levels of 214.9 ng/mL (95% CI: 60.1–369.7, p = 0.007) among women with cervical cancer (CC) compared to their cancer-free counterparts. Despite growing evidence of the role of interleukin-6 (IL-6) in CC, studies assessing this association among women of sub-Saharan African origin remain limited. This study investigated the association between serum IL-6 and CC and explored the effects of serum IL-6 levels on prognosis in patients with CC in Lagos, Nigeria. We conducted a cross-sectional study among women with and without CC in two hospitals. A venous blood sample was collected from each participant for laboratory analysis of serum IL-6 levels. We performed simple and multiple linear regression analyses to compare the unit increase in serum IL-6 levels between study groups while adjusting for relevant confounders. Our study found a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
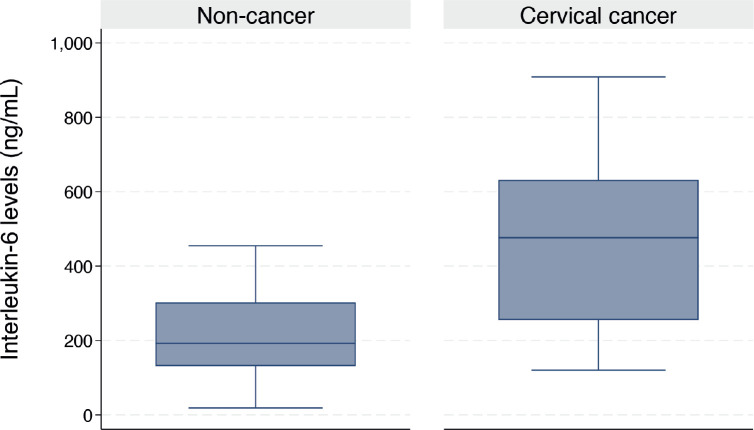 Figure 1
Figure 1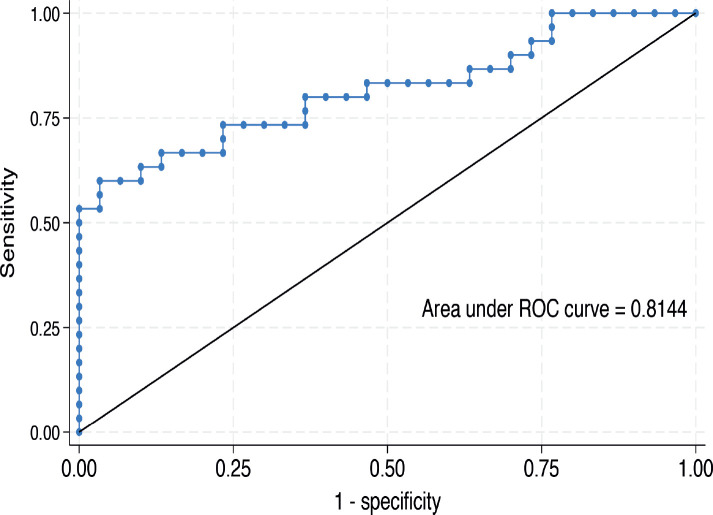 Figure 2
Figure 2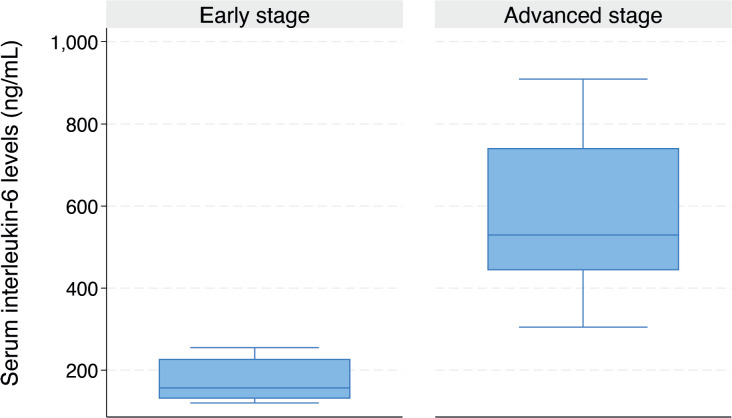 Figure 3
Figure 3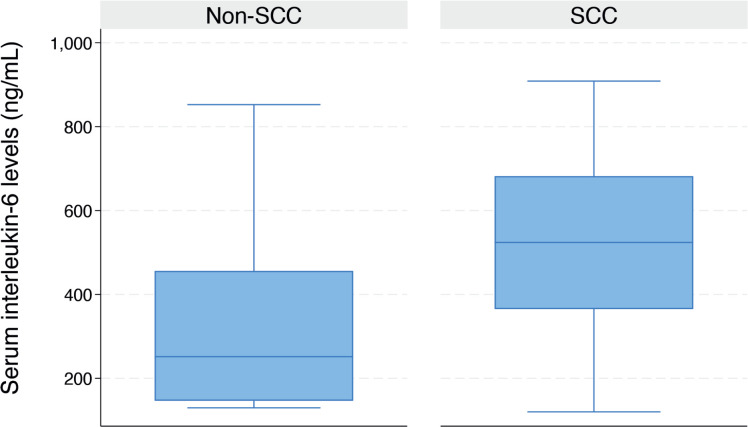 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Cytokine Signaling Pathways and Interactions · Endometrial and Cervical Cancer Treatments
Introduction
Cervical cancer (CC) remains a significant public health challenge worldwide [1], with its burden disproportionately affecting low- and middle-income countries [2]. Data indicate that sub-Saharan Africa bears the highest incidence and mortality rates from the disease [1, 3, 4], with Nigeria alone reporting approximately 12,075 new cases and 10,403 deaths annually [2, 5].
The development of CC has been strongly linked to persistent infection with oncogenic human papillomavirus (HPV), the primary etiological agent of the disease and its precursor lesions [6, 7]. However, the progression from HPV infection to invasive cancer is influenced by a complex interplay of environmental, lifestyle and host factors that modulate viral activity [1, 8]. Individual genetic variations in immune mediators play a critical role in susceptibility to neoplasia [9], with increasing evidence suggesting that pro-inflammatory cytokines contribute to CC pathogenesis [10].
Interleukin-6 (IL-6) is a multifunctional cytokine secreted by various cell types, such as macrophages, T cells, fibroblasts and endothelial cells, in response to infections, tissue damage and a range of inflammatory triggers [11, 12]. It is involved in immune regulation, inflammation, haematopoiesis and cancer development and progression [12]. IL-6 has been implicated in tumourigenesis by promoting cell proliferation, angiogenesis and resistance to apoptosis in several cancers [13–15], including CC, and is now considered a critical biomarker and therapeutic target in various diseases, particularly in inflammation-related pathologies and cancer [11, 13–15]. However, despite growing evidence of its role in CC [16–18], studies assessing the association between IL-6 and CC among women of sub-Saharan African origin remain limited. To address this gap and provide valuable insights into the role of IL-6 in CC susceptibility and progression, our study investigated the association between serum IL-6 and CC and then explored the effects of serum IL-6 levels on prognosis in patients with CC in Lagos, Nigeria.
Materials and methods
Study design and setting
This is a cross-sectional study conducted between January and December 2023 at the gynaecological oncology clinics of Lagos State University Teaching Hospital (LASUTH), Ikeja and Lagos Island Maternity Hospital (LIMH), Lagos Island, Lagos, Nigeria. The hospitals serve as public referral centres for other medical facilities in Lagos and its adjoining states. They both run gynaecology, cytology and colposcopy clinics from Monday to Friday of each week, providing evaluation, diagnosis and appropriate treatment for patients with pre-invasive and invasive CC.
Study population
Eligible participants were women aged 18 years or more with histologically confirmed CC (case group) enrolled from the study clinics using the consecutive sampling technique. The comparison group comprised randomly selected, unmatched healthy and cancer-free women attending the gynaecological and cytology clinics during the same study period as the case group. Exclusion criteria included a history of other malignancies, withdrawal of consent during the study and lack of physical and mental capacity precluding understanding of informed consent.
Study procedures
On confirming each participant’s eligibility, informed written consent was obtained upon explanation of the goals and procedures of the study. Information on sociodemographic and clinical characteristics, including participants’ age, parity, marital (married or unmarried) and menopausal (pre- and post-menopausal) status, types of marriage (mono- or polygamous), educational, occupational and socioeconomic status, religion, ethnicity, initiation of sexual activity and age at coitarche, use of alcoholic beverages and oral contraceptive pills, number of lifetime sex partners and International Federation of Gynaecology and Obstetrics (FIGO) stage and histological type of disease, were obtained from each participant, after which about 5 mL of peripheral blood samples were collected through venipuncture into a plain specimen bottle (without anticoagulant), sealed and transported within an hour to the main laboratory at LIMH. The samples were centrifuged to separate the serum, which was then stored frozen at −80°C before batched analysis of serum IL-6 concentrations with Human interleukin-6 ELISA Kit (E0090Hu) (Thermo Fisher Scientific Inc., Waltham, MA, USA).
Sample size calculation
Using the sample size formula for comparing means in Stata, we determined that a total sample size of n = 58 would provide 80% power at a type 1 error rate of 5% with provision for a 20% non-response or data recording error rate. This calculation was based on mean IL-6 values of 23.16 ± 19.57 pg/mL for CC patients and 9.91 ± 9.25 pg/mL for non-CC participants, derived using Hozo’s method [19] from the median IL-6 values reported in the study by Lippitz and Harris [20].
Statistical analysis
Statistical analyses were performed using Stata version 18.0 for Windows (StataCorp LLC, TX, USA). Data were summarised using descriptive statistics with continuous variables presented as mean (standard deviation) for normally distributed data or median (25th—75th centile) for skewed distributions. Serum IL-6 levels between the women with and without CC were compared using the non-parametric Wilcoxon rank sum test. We performed simple (bivariable) and multiple (multivariable) linear regression analyses with a backward conditional approach to compare the unit increase in serum IL-6 levels between the study groups while adjusting for potential confounders such as participants’ age, menopausal status, age at coitarche and the number of lifetime sex partners using coefficient (b) at 95% confidence interval (95%CI). We then performed a receiver operating characteristic (ROC) curve analysis for serum IL-6 to derive an optimal discriminatory cut-off value for serum IL-6 levels that distinguished between CC and non-cancer. Subgroup analyses were also performed to compare the serum IL-6 levels between cancer stage (early versus advanced) and histological type squamous cell carcinoma (SCC versus non-SCC) in women with CC. Statistical significance was reported at p < 0.05.
Statement of ethics
This study was approved by the Health Research Ethics Committee of the LASUTH, the Health Service Commission and the LIMH (approval number LREC/10/1990). We conducted the study ethically per the World Medical Association Declaration of Helsinki. All the study participants read and signed a written informed consent before enrolment, and we ensured strict adherence to the privacy and confidentiality of participants' information during and after conducting the study.
Results
A total of 107 potential participants were screened for eligibility in the study (58 in LASUTH and 49 in LIMH). Of these, 37 (63.8%) were enrolled from LASUTH, while 23 (46.9%) were from LIMH. We included 60 women in the study (30 women diagnosed with CC and 30 cancer-free comparators). The mean age of participants with CC was significantly higher than that of the comparators (52.0 ± 10.0 years versus 42.6 ± 6.7 years, p < 0.001). Similarly, the median age at first sexual intercourse (coitarche) was higher among those with CC compared to the cancer-free comparison group (19.5 years (IQR: 18.0–21.0) versus 17.5 years (IQR: 17.0–18.0), p = 0.005). Similarly, women with CC also reported a higher median number of lifetime sexual partners (5 (IQR: 3–6) versus 3 (IQR: 2–5), p = 0.002). As summarised in Table 1, other sociodemographic characteristics were similar between the groups.
The clinicopathological characteristics of the CC patients (n = 30) are summarised in Table 2. Cervical SCC was the most common histological type of CC (70.0%, n = 21), while the least common was adeno-squamous carcinoma (6.7%, n = 2). Most CC patients presented with advanced disease (36.7%, n = 11).
The median serum IL-6 level was higher in women with CC than in their cancer-free counterparts (476.3 (IQR: 254.9–631.9) versus 192.4 (IQR: 131.0–302.4) ng/mL, p < 0.001) as shown in Figure 1. In the bivariable linear regression analysis performed in Table 2, CC was significantly associated with increased serum IL-6 levels (p < 0.001). As shown in Table 3, after adjusting for potential confounders in the multivariable model, this association remained statistically significant with an estimated unit change of +214.9 ng/mL (95% CI: 60.1–369.7, p = 0.007). Figure 2 shows the ROC curve for serum IL-6, demonstrating its discriminatory ability. The area under the curve (AUC) was 0.814 (95%CI: 0.704–0.925), indicating good diagnostic performance. The optimal serum IL-6 cut-off value for distinguishing between CC patients and their cancer-free counterparts was 365.1 ng/mL, corresponding to a sensitivity of 66.7% and a specificity of 86.7%.
As illustrated in the box plot in Figure 3, the median serum IL-6 level was significantly higher in women with advanced-stage CC compared to those with early-stage disease (324.7 ng/mL (IQR: 188.5–516.2) versus 156.7 ng/mL (IQR: 130.4–227.6), p = 0.015). The median serum IL-6 level was significantly higher in women diagnosed with SCC compared to those without SCC (523.9 ng/mL (IQR: 365.1–682.1) versus 203.6 ng/mL (IQR: 131.3–334.3), p < 0.001) (Figure 4).
Discussion
Our study evaluated the association between serum IL-6 and CC and explored the effects of serum IL-6 levels on prognosis in patients with CC in Lagos, Nigeria. We reported that serum IL-6 levels were significantly higher in patients with CC compared to cancer-free women, with an optimal serum IL-6 cut-off value of 365.1 ng/mL for distinguishing between CC and cancer-free participants. Further stratification of CC patients revealed that IL-6 levels were significantly elevated in patients with advanced-stage CC compared to those with early-stage disease and in patients diagnosed with SCC compared to those without SCC.
Our study has further provided compelling evidence supporting the association between elevated serum IL-6 levels and CC in corroboration with the findings by Cai et al [16] in Jiangsu, China and Wagh et al [21] in Maharashtra, India. This was even similar to the study by Song et al [18] in Shanghai, China, which reported a significantly higher IL-6 expression in formalin-fixed, paraffin-embedded CC tissues than in adjacent non-tumour tissues examined by immunohistochemistry. This further suggests that IL-6 plays a critical role as a pro-inflammatory cytokine in the tumour microenvironment [22] and its elevated levels in CC patients may reflect ongoing chronic inflammation, which promotes tumour growth, angiogenesis and immune evasion [14]. Persistent infection with high-risk HPV strains, a known driver of cervical carcinogenesis [1], induces inflammatory responses that may contribute to increased IL-6 expression [23]. Furthermore, similarly to previous studies [16, 21], our study demonstrated a high discriminatory ability for serum IL-6, indicating its good diagnostic performance and potential usefulness as a diagnostic adjunct in resource-constrained settings like ours, where access to more advanced diagnostic tools is limited.
As revealed in our study, IL-6 levels were significantly elevated in patients with advanced-stage CC compared to those with early-stage disease. This finding is consistent with previous studies indicating that IL-6 plays a critical role in tumour progression, angiogenesis and immune modulation in CC [15, 16, 18, 20, 21]. The immunosuppressive role of IL-6 contributes to immune evasion by suppressing anti-tumour immune responses, particularly by promoting regulatory T-cell expansion and inhibiting cytotoxic T-cell activity [24]. Additionally, we reported that IL-6 levels were markedly higher in patients diagnosed with SCC than those without SCC, underscoring its role in the pathophysiology of this predominant and inflammation-driven [25] form of CC. These findings reinforce the role of IL-6 as a potential biomarker for CC and highlight its likely relevance in the pathogenesis and progression of the disease [24, 26]. Therefore, given its involvement in inflammation and cancer progression [18, 23], IL-6 could serve as a potential target for therapeutic interventions in CC [11, 14].
The main strength of this study is that it is the first to evaluate the association between serum IL-6 and the risk of CC in Lagos State, Nigeria. However, the study has a few limitations that should be acknowledged. First, we used a cross-sectional study design, which precludes a definitive conclusion of a causal relationship between IL-6 and CC. Second, the sample sizes used in the subgroup analyses may be insufficient to detect significant associations between IL-6 and CC stages and histological types. Therefore, future longitudinal studies with large cohorts and diverse populations are necessary to confirm the findings of our study.
Conclusion
We observed that serum IL-6 levels were comparably higher in patients with CC than in cancer-free women, giving an optimal discriminatory cut-off value of 365.1 ng/mL. Serum IL-6 levels were also significantly higher in patients with advanced-stage CC compared to those with early-stage disease and in those diagnosed with SCC compared to those without SCC. These findings highlight the potential utility of serum IL-6 as a biomarker for CC diagnosis and prognosis. However, further studies are needed to explore IL-6 as a target for therapeutic intervention and assess its use in risk stratification and treatment monitoring in CC patients.
Conflicts of interest
The authors have no conflicts of interest.
Funding
The authors have received no specific funding for this research. However, the author (KSO) protected time was supported through funding from the National Cancer Institute and Fogarty International Center of the National Institutes of Health under Award Numbers K43TW011930 and D43TW010934 and the Conquer Cancer International Innovation Grant under Project ID 2024IIG-2761200216. The content of this paper is solely the responsibility of the authors. It does not necessarily represent the official views of the National Cancer Institute, Fogarty International Center or the National Institutes of Health and the Conquer Cancer Foundation. The funding agencies were not involved in the study design, manuscript preparation or the decision to submit the manuscript for publication.
Author contributions
Conceptualisation and design: Muisi A Adenekan, Joseph B Minari
Provision of study materials or patients: Muisi A Adenekan, Ayodeji Adefemi, Adebayo Sekumade, Adeyemi A Okunowo, Kehinde S Okunade
Data collection: Muisi A Adenekan, Ayodeji Adefemi, Ayomide I Fayinto, Adebayo Sekumade, Temitope V Adekanye
Data analysis: Gbenga Olorunfemi, Ayomide I Fayinto, Kehinde S Okunade
Funding acquisition: Muisi A Adenekan
Writing—original draft: Muisi A Adenekan, Joseph B Minari, Kehinde S Okunade
Writing—review and editing: Muisi A Adenekan, Joseph B Minari, Adeyemi A Okunowo, Kehinde S Okunade
Supervision: Joseph B Minari, Adeyemi A Okunowo, Kehinde S Okunade
All the authors approved the final version of the manuscript
All authors are accountable for all aspects of the work.
Data availability
The dataset for this study will be made available on reasonable request from the corresponding author (KSO).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Okunade KS Human papillomavirus and cervical cancer J Obstet Gynaecol 20204060260810.1080/01443615.2019.163403031500479 PMC 7062568 · doi ↗ · pubmed ↗
- 2Sung H Ferlay J Siegel RL Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin 2021712092493353833810.3322/caac.21660 · doi ↗ · pubmed ↗
- 3Mwanahamuntu MH Sahasrabuddhe VV Kapambwe S Advancing cervical cancer prevention initiatives in resource-constrained settings: insights from the Cervical Cancer Prevention Program in Zambia P Lo S Med 20118 e 100103210.1371/journal.pmed.100103221610859 PMC 3096609 · doi ↗ · pubmed ↗
- 4Sankaranarayanan R Overview of cervical cancer in the developing world Int J Gynaecol Obstet 200695 Suppl 1S 205S 21010.1016/S 0020-7292(06)60035-029644674 · doi ↗ · pubmed ↗
- 5Global Burden of Disease Cancer Collaboration Fitzmaurice C Dicker D Pain A The global burden of cancer JAMA Oncol 20151505527201310.1001/jamaoncol.2015.073526181261 PMC 4500822 · doi ↗ · pubmed ↗
- 6Ezechi OC Ostergren PO Nwaokorie FO The burden, distribution and risk factors for cervical oncogenic human papilloma virus infection in HIV positive Nigerian women Virol J 201411510.1186/1743-422X-11-524433568 PMC 3896716 · doi ↗ · pubmed ↗
- 7Kombe Kombe AJ Li B Zahid A Epidemiology and burden of human Papillomavirus and related diseases, molecular pathogenesis, and vaccine evaluation Front Public Health 2021855202810.3389/fpubh.2020.55202833553082 PMC 7855977 · doi ↗ · pubmed ↗
- 8John-Olabode SO Udenze IC Adejimi AA Association between tumour necrosis factor-a polymorphism and cervical cancer in Lagos State, Nigeria Ecancermedicalscience 202519184510.3332/ecancer.2025.184540259899 PMC 12010130 · doi ↗ · pubmed ↗