Is there a way to reduce the infection associated with external ventricular shunts? A systematic review and meta-analysis of the recent bundle of care
Moustapha Ramadan, Shrouk Fawze Mohamed, Ahmed A. Abdulalim, Anas Ashraf Elassal, Aya Abdelsamad, Belal Shehata, Yasmeen Farag, Mohamed Elshaer, Samar Kolkas, Nesrine Fathi Hanafi

TL;DR
This study finds that using a bundle of care measures can reduce infections from external ventricular drains but does not affect mortality or hospital stay.
Contribution
The study evaluates the effectiveness of a bundle of care for reducing EVD-related infections through a systematic review and meta-analysis.
Findings
Bundle care significantly reduced infection risk and drain stay duration.
No significant effect on mortality or ventriculitis rates was observed.
The study supports standardized care bundles but highlights the need for further research on specific complications.
Abstract
Background: Although external ventricular drains (EVDs) are crucial in neurosurgical care, they carry a high risk of healthcare-associated ventriculitis, with reported infection rates. Numerous interventions were thought to aid in infection control, but there is still an ongoing increase in infection incidence. Recently, bundled interventions with standardized protocols, antimicrobial‐impregnated catheters, tunneling techniques, chlorhexidine dressings, and limited antibiotic prophylaxis have shown an interesting efficacy in shunt-related infection control. Methods: A systematic review was conducted using PubMed, Scopus, Google Scholar, Cochrane CENTRAL, and Web of Science to search for published articles on care bundles with at least three discrete preventive measures. Data analysis was performed using R software, estimating mean difference and risk ratios. Results: Seventeen studies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
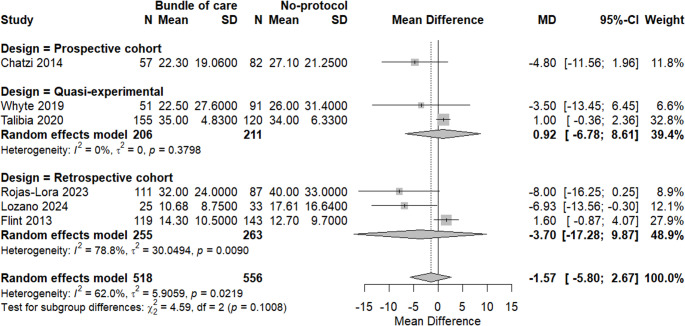 Figure 10
Figure 10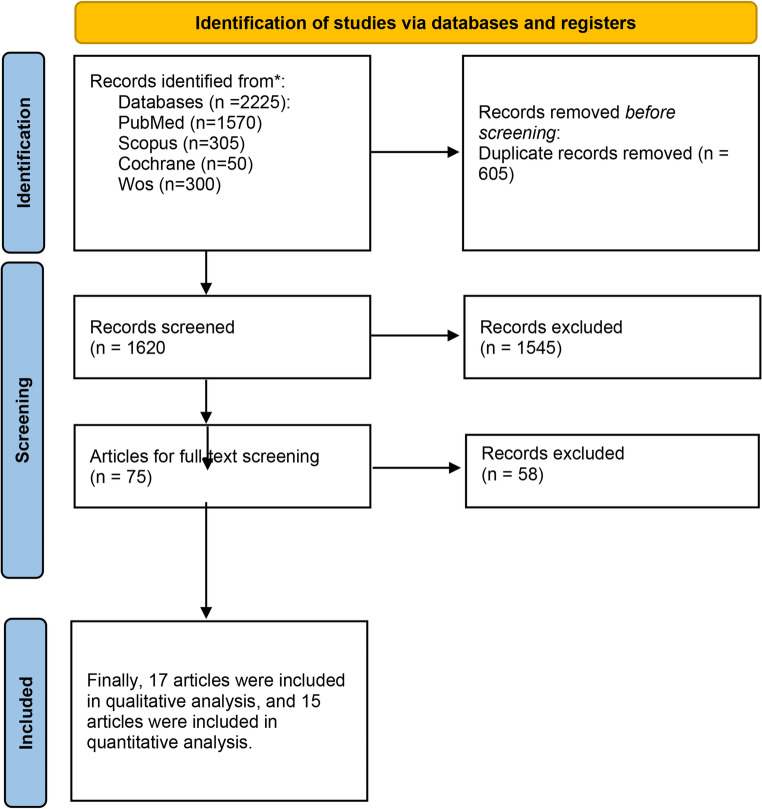 Figure 1
Figure 1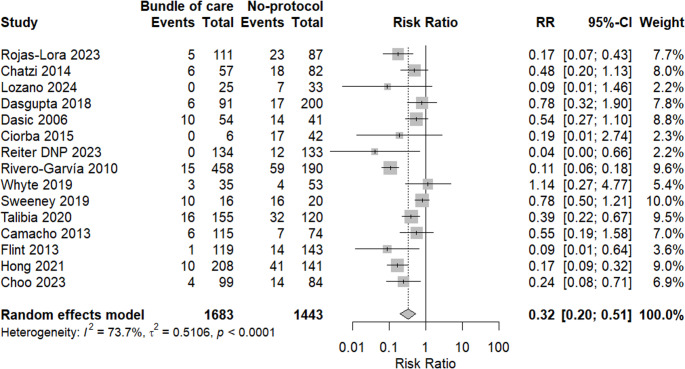 Figure 2
Figure 2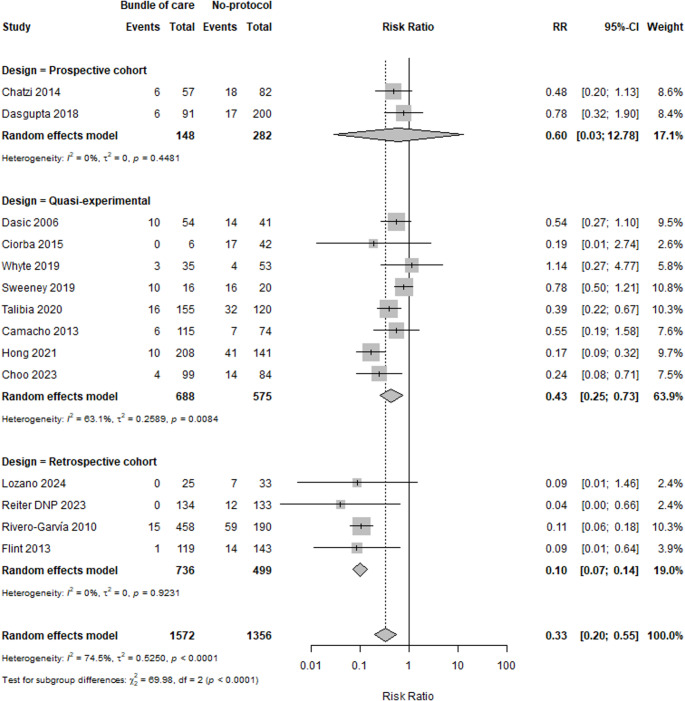 Figure 3
Figure 3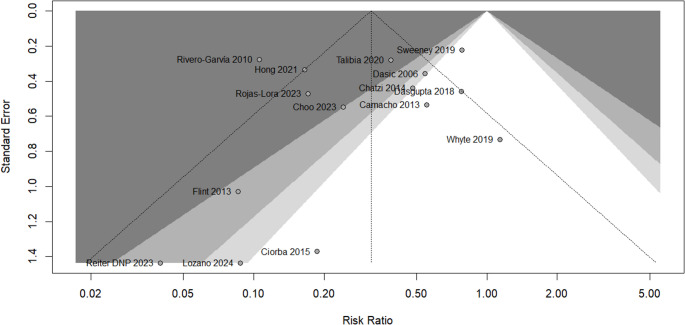 Figure 4
Figure 4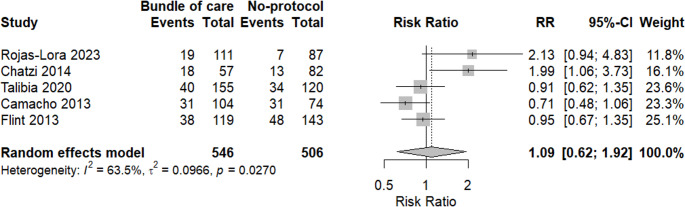 Figure 5
Figure 5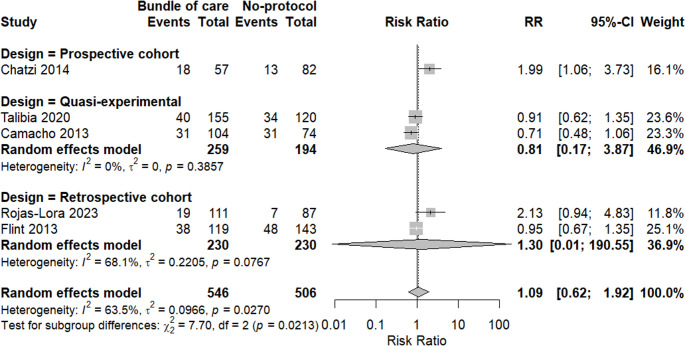 Figure 6
Figure 6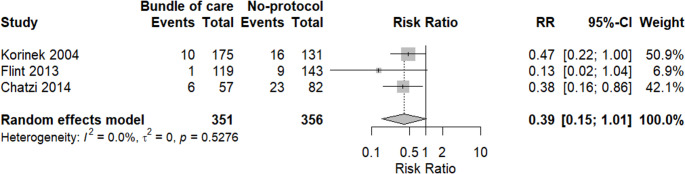 Figure 7
Figure 7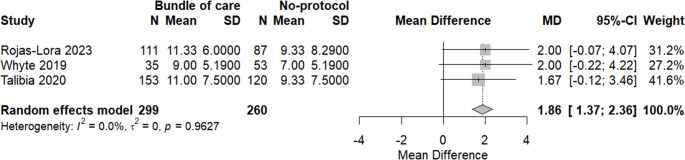 Figure 8
Figure 8 Figure 9
Figure 9- —Alexandria University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebrospinal fluid and hydrocephalus · Central Venous Catheters and Hemodialysis · Botulinum Toxin and Related Neurological Disorders
Introduction
External ventricular drains (EVDs) play a crucial role in managing serious conditions such as acute hydrocephalus, traumatic brain injury, subarachnoid hemorrhage, and various other disorders that require cerebrospinal fluid (CSF) diversion and monitoring of intracranial pressure. Besides their role in diagnosis and treatment, EVDs facilitate the sampling of cerebrospinal fluid and enable the intrathecal administration of antibiotics or chemotherapeutic agents [1, 2]. The use of EVDs carries some danger even if their intended function is vital. One of the most important problems is EVD-related infection (EVDI), which could cause meningitis or ventriculitis, far more morbidity, longer hospital stays, and more healthcare expenses [3].
Recent research indicated that the incidence rates of EVDI vary significantly, ranging from 2% to 45%.
This wide variation underscores the impact of differing diagnostic criteria, institutional practices, adherence to sterile technique, and patient populations on reported infection rates. Many factors contribute to such variability. Key risk factors include duration of catheterization, frequency of CSF sampling or manipulation, number of catheter insertions or changes, and presence of CSF leak or bilateral EVDs. Also, underlying pathologies — such as subarachnoid hemorrhage/intraventricular hemorrhage (SAH/IVH), immunosuppression, concomitant systemic infection, or prior neurosurgical procedures — may increase risk [4–7].
In consideration of these challenges, a range of preventive strategies has been suggested and implemented over time. These strategies are not limited to the implementation of antibiotic-impregnated catheters (AICs), silver-impregnated catheters, closed drainage systems, minimal handling protocols, and standardized care bundles. [8] The introduction of care bundles, which consist of a structured set of evidence-based practices designed to enhance outcomes when implemented together, has garnered significant attention. A recent meta-analysis showed that care bundles reduced the risk of EVD infections by about 54% (pooled risk ratio 0.46; 95% CI 0.33–0.65; P < 0.001) compared to non-bundle approaches [9]. Furthermore, meta-analyses and systematic reviews have found that both antibiotic-impregnated and silver-impregnated catheters may lower infection risk compared with standard catheters [10]. Bundles of care generally include hand hygiene practices, comprehensive barrier precautions during insertion, the implementation of AICs, ongoing staff training, and uniform protocols for CSF sampling and EVD maintenance [11]. However, reported results are highly heterogeneous across studies. Differences in study design, diagnostic criteria for infection (microbiological culture vs. clinical + laboratory criteria), definitions of catheter “duration,” frequency of sampling/manipulation, use (or not) of peri-procedural antibiotics, and types of antimicrobial coatings all vary widely. Because of this, it isn’t easy to draw definitive conclusions about the optimal bundle components or the relative efficacy of antibiotic-, silver-, or standard-impregnated catheters under different conditions (e.g., short vs. long-duration EVD) [9]. – [10].
While bundles appear effective in reducing infection rates, the data on their impact on broader outcomes such as morbidity, mortality, length of ICU/hospital stay, need for EVD replacement, and cost-effectiveness remain insufficiently characterized. This systematic review and meta-analysis aim to evaluate the safety and efficacy of the bundle of care in preventing infections and associated complications related to EVD.
Methods
This systematic review and meta-analysis followed the guidelines of PRISMA for this study design. The protocol of this study was registered at PROSPERO, with the following ID: CRD42025648331.
Study design and registration
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [12]. The study protocol was prospectively registered with PROSPERO (CRD42025648331) and is publicly available at https://www.crd.york.ac.uk/PROSPERO/view/CRD42025648331.
Approval was granted by the Ethics Committee of Alexandria University, faculty of Medicine (Date 6–7-2025/No 0307396).
Eligibility criteria
We included randomized controlled trials (RCTs) and observational studies (cohort studies, case-control studies, and case series) that evaluated the effectiveness of a bundle of care in reducing complications associated with external ventricular drains (EVDs), particularly infections. Studies were eligible if they involved patients requiring CSF drainage, such as those with hydrocephalus or intracranial hypertension, and compared outcomes between patients managed with a care bundle versus those without or pre-protocol groups.
Primary outcomes included:
- Incidence of EVD-related infection (ventriculostomy-related infection where microorganisms mainly bacteria enter the brain through the EVD, leading to conditions like bacterial meningitis or ventriculitis.)
- Mortality rate.
Secondary outcomes included:
- Duration of EVD placement.
- Hospital length of stay.
- Microbial etiology (e.g., Gram-negative vs. Gram-positive pathogens).
- Other complications such as catheter obstruction, hemorrhage, or malposition.
Search strategy
A comprehensive literature search was conducted in the following electronic databases: PubMed, Scopus, Web of Science, and Cochrane CENTRAL. The search strategy included terms such as “external ventricular drain,” “care bundle,” “infection prevention,” “ventriculitis,” and “CSF diversion.” No restrictions were placed on language or publication date.
Study selection and data extraction
Two individuals assessed titles and abstracts for relevance. Full-text papers of possibly qualifying research were examined utilizing established inclusion criteria. Conflicts at any phase were settled through discussion or consultation with an additional reviewer.
Data extraction was conducted independently by two writers utilizing a standardized form. The extracted data included study information (author, year, country, design), patient demographics, specifics of the intervention and comparator, and the outcomes assessed.
Risk of bias assessment
The Newcastle-Ottawa Scale was employed for cohort and case-control research which assessed the included papers across three domains: Selection, Comparability and outcome, whereas the JBI Critical Appraisal Checklist was utilized for quasi-experimental investigations which assessed the included studies according to several factors, including the clear establishment of the cause and effect relationship, the presence or absence of statistically significant differences among study groups, the elimination of confounding variables, the presence of a control group, the measurement of the outcome and the appropriateness of the statistical analysis used.
Each evaluation was performed separately by two reviewers, with conflicts reconciled through consensus.
Data synthesis and statistical analysis
The meta-analysis was conducted utilizing Review Manager (RevMan) version 5.4.1. Risk ratios (RRs) with 95% confidence intervals (CIs) were computed for dichotomous outcomes. Mean differences (MDs) were employed for continuous outcomes. The I² statistic was utilized to evaluate statistical heterogeneity. In instances with significant heterogeneity (I² > 50%), a random-effects model was utilized. A fixed-effect model was employed. Sensitivity analyses were conducted by systematically excluding individual studies to evaluate the consistency of the findings. Funnel plots were generated to evaluate publication bias.
Results
Literature search revealed 2225 papers through searching different databases, 605 results were duplicates, 1620 were screened by title and abstract. 1545 were excluded, and 75 were screened by full text. Finally, 17 papers were included in our study, as illustrated in Fig. 1. Out of 17 studies, 9 were quasi-experimental, 6 were retrospective, and 2 were prospective cohorts [4, 5, 13–27]. Quality assessment for the included studies showed that 9 studies were of good quality, while 3 studies were of poor quality and 5 showed fair quality, as mentioned in (Table 1) in the supplements.Fig. 1. Prisma flow diagram
Outcomes.
A meta-analysis of 15 studies was done, supporting that the bundle of care showed a protective effect against EVDI in comparison to another group with an RR of 0.32 (95% CI: 0.20, 0.51, p = 0.0001). There was a significant heterogeneity with I^2^ = 73.7%, so a random effect model was applied as shown in Fig. 2.Fig. 2A forest plot showing the incidence of EVDI in both groups
Subgrouping analysis based on study design was done in a try to explore the source of heterogeneity. We found that heterogeneity was obviously resolved among retrospective cohort studies (I^2^ = 0%) without any change in the context of the results, except in prospective cohorts, where there was no significant difference between the two groups. Quasi-experimental studies showed a high level of heterogeneity, but the results remain significant (I^2^ = 63.1%). There was a significant difference between subgroups with p < 0.0001, as shown in Fig. 3.Fig. 3. Subgrouping analysis of EVDI based on study design
Egger’s test was conducted to assess the potential presence of publication bias. We found that there was no statistically significant evidence of asymmetry in the funnel plot (p = 0.4324), as seen in Fig. 4.Fig. 4. Funnel plot of studies in EVDI
In terms of bacterial infections, we analyzed the incidence of gram-negative and gram-negative bacteria. A meta-analysis of seven studies revealed that there was no difference between the two groups in the incidence of gram-negative (RR = 0.59, 95% CI: 0.28;1.7, p = 0.1442). There was a moderate reported heterogeneity, with I^2^ = 34.1%, as seen in Figure S1 in the supplements.
A sensitivity analysis was done by excluding Sweeney et al., and heterogeneity was totally resolved, with a change in the context of the results, supporting that the bundle group had a lower risk for gram-negative (RR = 0.46, 95% CI: 0.24;0.86, p = 0.0.025), as shown in Figure S2 in supplements.
According to the gram-positive, there was no significant difference between both groups (RR = 0.85, 95% CI: 0.32;2.21, p = 0.6554). Moderate heterogeneity was found (I^2^ = 53.1%), as shown in Figure S3 in the supplements.
A sensitivity analysis was done by excluding Rojas-Lora et al., and heterogeneity was reduced with I^2^ = 12.1%, with no change in the context of the results (RR = 0.67, 95% CI: 0.35;1.28, p = 0.1415), as shown in Figure S4 in the supplements.
A meta-analysis of mortality rates between the two groups was done. There was no significant difference between the bundle of care group and the other one, revealing an interesting increased risk with the bundle of care group (RR = 1.09, 95% CI: 0.62, 1.92, p = 0.6924). Heterogeneity was high among included studies, with I2 = 63.5%, as shown in Fig. 5.Fig. 5. Forest plot showing mortality rates in both groups
Subgrouping analysis was done based on study design, and we found that heterogeneity was reduced among quasi-experimental studies with I^2^ = 0%, while retrospective studies revealed moderate heterogeneity with I^2^ = 68.1%, as shown in Fig. 6.Fig. 6. Subgrouping analysis of mortality based on study design
In terms of EVD-associated ventriculitis, a meta-analysis of three studies revealed that the bundle of care application did not show any significant difference in incidence of EVD-associated ventriculitis compared to the group with no protocol (RR = 0.39, 95%CI 0.15: 1.01, p = 0.0509). In addition, there was no heterogeneity among included studies, as shown in Fig. 7.Fig. 7A meta-analysis of the risk of EVD-associated ventriculitis incidence between both groups
Regarding drain stay, a meta-analysis was done; there was a significantly lower duration in the bundle of care group (MD = 1.89, 95% CI: 1.37; 2.36, p = 0.0038). No heterogeneity was found, as seen in Fig. 8.Fig. 8. Meta-analysis of drain stays
A meta-analysis of six studies was done to assess the difference in hospital stay duration between applying a bundle of care and not applying it; there was no significant difference in hospital stay in the bundle group with MD = −1.57 (95% CI: −5.80; 2.67, p = 0.3855). Moreover, there was a significant heterogeneity among included studies, with I^2^ = 62%, as shown in Fig. 9.Fig. 9A meta-analysis of hospital stay duration between both groups
Subgrouping analysis revealed that heterogeneity was resolved among quasi-experimental studies, while retrospective studies showed significant heterogeneity without any significant change in the context of the results. There was no significant difference between subgroups, as shown in Fig. 10.Fig. 10. Subgrouping analysis of hospital stays based on study design
Discussion
Infection rates associated with shunts have been growing rapidly in recent years. Sometimes, shunts are a lifesaving procedure to aid in decreasing intracranial pressure; the literature reports incidence rates varying between 3.1% and 11.4 per 1,000 catheter-days, indicating a continuous need to make the procedure safer for patients [28, 29]. This systematic review and meta-analysis evaluated the impact of implementing care bundles on outcomes related to EVDs.
The results of the present meta-analysis show a notable decrease in EVDI incidence through the use of care bundles, which aligns with earlier research emphasizing the effectiveness of such standardized preventive strategies. Choo et al. reported a reduction in EVDI rates from 16.7% to 4.0% after implementing a care bundle based on guidelines from the Centers for Disease Control and Prevention [14]. Similarly, Lora et al. reported a 58% lower EVDI rate after implementing a bundle that emphasized CSF sampling minimization [5]. These findings support the protective effect of care bundles observed in the present meta-analysis.
Furthermore, there was no significant difference in the incidence of gram-negative or gram-positive bacterial infections associated with EVD between the care bundle and control groups in this study. Gram-negative organisms remained the most frequently isolated pathogens, in agreement with prior studies reporting a predominance of gram-negative bacteria. In contrast, Jamjoom et al. reported that Gram-positive organisms were the most frequent in their study [30].
Our results did not reveal a statistically significant difference in mortality rates or length of hospital stay between patients managed with a care bundle and those receiving standard care in the context of EVD. While care bundles have been shown in some studies to improve compliance with best practices and reduce certain complications, such as catheter-related infections, their impact on hard clinical outcomes, including mortality and hospital stay, remains controversial [5, 11, 31]. Numerous studies have reported that implementing a care bundle reduces EVD-related infection rates, but there is no significant effect on mortality or length of stay, aligning with our current findings [5, 15, 21]. These findings suggest that while care bundles are beneficial in standardizing care and reducing preventable adverse events, broader clinical outcomes such as mortality may be influenced by multifactorial elements beyond the scope of bundle-based interventions. More high-quality, controlled studies are needed to determine whether additional factors, such as timing, patient severity, or institutional resources, modulate the effectiveness of care bundles on long-term outcomes.
The effectiveness of care bundles depends on proper implementation, staff adherence, and institutional support. Several studies have highlighted the importance of multidisciplinary collaboration, staff education, and strict adherence to standardized protocols in achieving sustained reductions in infection rates [22, 32].
Limitations
This meta-analysis has several limitations. First, the “care bundle” components were not uniform: each study implemented a slightly different set of practices, and specific measures (e.g., use of antibiotic-impregnated catheters, frequency of CSF sampling, use of prophylactic antibiotics) were often poorly detailed. Protocols for EVD care varied greatly between hospitals, and adherence also differed. This inconsistency makes it difficult to generalize findings; a bundle that was effective in one setting may not have the same impact in another if the components or compliance differ. In addition, definitions of EVD infection varied, with some studies requiring positive CSF cultures with clinical signs, while others included any positive culture or used different diagnostic time frames. This contributed to the substantial heterogeneity observed among the included studies. Although only bundles containing more than three components were included, methodological variability remained significant. Additionally, the care bundle had no statistically significant impact on patient-centered outcomes such as mortality or hospital length of stay. Across the aggregated data, implementing EVD care bundles did not measurably reduce death rates or shorten hospitalization time compared to standard care. This is even though EVD infections themselves are associated with higher mortality and prolonged hospital stay in individual studies. This may reflect the influence of multiple confounding clinical factors unrelated to EVD infection alone.
Conclusion
This meta-analysis supports the use of care bundles in lowering EVDIs. The general trend shows that care bundles have a preventive action against infections. Still unclear whether there are no improvements in terms of mortality and hospital stay, which emphasizes the necessity of more research.
Future research should focus on enhancing the implementation of standardized elements of the bundle of care and investigating other interventions to improve overall clinical outcomes.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1 (DOCX 111 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cui Z, Wang B, Zhong Z, Sun Y, Sun Q, Yang G et al (2015) 1;43(7):e 23-32 Impact of antibiotic- and silver-impregnated external ventricular drains on the risk of infections: A systematic review and meta-analysis. Am J Infect Control. 10.1016/j.ajic.2015.03.01510.1016/j.ajic.2015.03.01525934064 · doi ↗ · pubmed ↗
- 2Blacker SN, Prabhakar H, Moreton EO, Burbridge M, Dunn L, Gouker LN et al (2025) Effect of bundled care on external ventricular drain infections: A systematic review and Meta-analysis. J Neurosurg Anesthesiol 17. 10.1097/ANA.000000000000107110.1097/ANA.000000000000107141243982 · doi ↗ · pubmed ↗
- 3Kubilay Z, Amini S, Fauerbach L, Archibald L, Friedman W, Layon A (2012) Decreasing ventricular infections through the use of a ventriculostomy placement bundle: experience at a single institution. J Neurosurg 118. 10.3171/2012.11.JNS 12133610.3171/2012.11.JNS 12133623259820 · doi ↗ · pubmed ↗
- 4Hong B, Apedjinou A, Heissler HE, Chaib H, Lang JM, Al-Afif S et al Effect of a bundle approach on external ventricular drain-related infection n.d. 10.1007/s 00701-020-04698-8/Published 10.1007/s 00701-020-04698-833427989 · doi ↗ · pubmed ↗
- 5Lozano M, Wang AS, Siddiqi I, Dy O, Ko K, Sweiss R et al (2024) Extraventricular Drain Care Bundle Decreases Cerebrospinal Fluid Infection Rates Associated With Extraventricular Drain-Related Procedures and Systemic Infection. Cureus. 10.7759/cureus.5244010.7759/cureus.52440 PMC 1087102438371086 · doi ↗ · pubmed ↗
- 6Ciorba VCGAMLCD (2015) Reducing external drainage-related cerebrospinal fluid infections through implementation of a multidisciplinary protocol: experience in a paediatric hospital 26499427 · pubmed ↗