Determinants, Pathways, and Outcomes of Health Literacy in India: A System Dynamics Modelling Study
Arjun B, Fathima Hassan, Akhil Jaison

TL;DR
This study uses system dynamics modeling to explore health literacy in India, revealing feedback loops that maintain poor health outcomes and showing that combined policies are more effective.
Contribution
The study introduces a system dynamics model of health literacy in India, identifying feedback loops and testing policy interventions.
Findings
Two reinforcing feedback loops, the 'Health Disparity Trap' and 'System Trust Spiral,' perpetuate poor health outcomes.
Isolated interventions had little impact, but a stacked, multimodal approach significantly reduced the population with poor health outcomes.
The baseline scenario predicted 55.6 million people with poor health outcomes, reduced to 35.7 million with the stacked intervention.
Abstract
Health literacy is a critical determinant of health. While many studies identify linear associations, the dynamic feedback mechanisms that create policy resistance and perpetuate health inequities remain poorly understood and studied. This study aims to develop a conceptual model of health literacy contextual for India, grounded in a systematic review of the literature, to identify key feedback loops and to test the comparative effectiveness of different policy interventions via system dynamics modelling. We conducted a systematic review to identify determinants, pathways and outcomes of health literacy in India. The search yielded 559 records. Two independent reviewers did title and abstract screening, resulting in 39 articles selected for full-text review. After four records could not be retrieved, 35 full texts were assessed for inclusion in the study, and 30 studies met the final…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
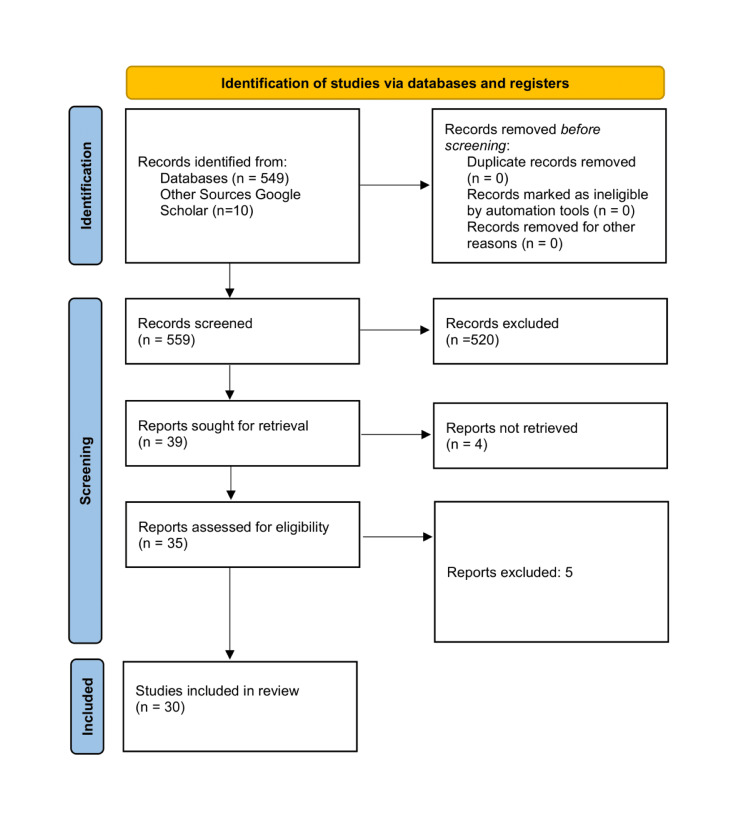 Figure 1
Figure 1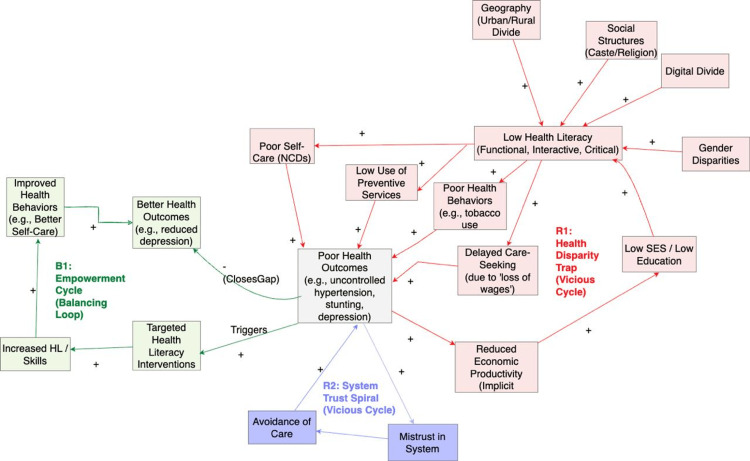 Figure 2
Figure 2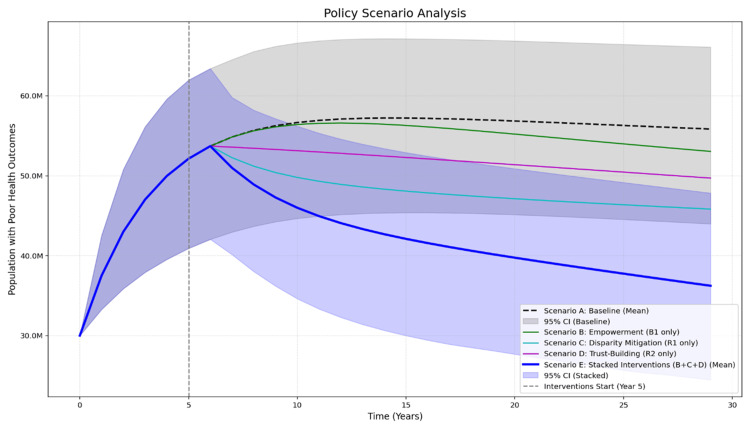 Figure 3
Figure 3| First Author, Year | Study Design | Target Population | Key Findings |
| Ahmad et al., 2021 [ | Cross-sectional | Women from rural Uttar Pradesh | An integrated microfinance and health literacy program improved knowledge of maternal danger signs. |
| Ahmad et al., 2022 [ | Quasi-experimental | Pregnant/recently delivered women from rural Uttar Pradesh | An integrated microfinance and health literacy program improved birth preparedness and complication readiness. |
| Baliga, 2019 [ | Editorial | Children and parents | Proposes comprehensive solutions focusing on education, policy, and service delivery to improve child oral health literacy. |
| Chauhan & Trivedi, 2024 [ | Mixed-method | Hypertensive adults from Gujarat | Illiteracy about tobacco hazards was significantly associated with tobacco addiction among hypertensive patients. |
| Das, 2020 [ | Cross-sectional | Adult population from Ghaziabad, Uttar Pradesh | 50% had inadequate oral health literacy, which was significantly associated with lower socioeconomic status and poorer oral health status. |
| Douglass et al., 2021 [ | Mixed-methods | Emergency Department clinicians | Low health literacy among patients was a major barrier to effective communication in multilingual Indian Emergency Departments. |
| Dsouza et al., 2021 [ | Cross-sectional | Hindi and Kannada-speaking individuals | Validated the HLS-EU-Q16 for use in India. |
| Gautam et al., 2021 [ | Cross-sectional | Chronic disease patients from Rajasthan | 65.8% had insufficient health literacy, which was a significant predictor of lower COVID-19 awareness and preventive behaviour. |
| Gokdemir et al., 2024 [ | Editorial | General | Discusses micro, meso, and macro-level factors influencing health literacy and highlights the need for culturally acceptable, target-specific interventions. |
| Gupta et al., 2020 [ | Prospective observational | Adult cancer patients from Karnataka | Inadequate health literacy and cognitive impairment were associated with severe adverse drug reactions to chemotherapy. |
| Harding, 2022 [ | Qualitative | Cancer patients, families, and clinicians from Southern India | Families often conceal cancer diagnoses, leading to poor patient outcomes and a lack of agency in decision-making. |
| Jagan, 2018 [ | Cross-sectional | School teachers from Karnataka | Conceptual oral health knowledge was fair; it was influenced by gender, age, education, and income and was associated with periodontal health. |
| Johri, 2015 [ | Cross-sectional | Mothers in Uttar Pradesh and New Delhi | Maternal health literacy was associated with higher child vaccination completion rates in both rural and urban settings. |
| Johri, 2016 [ | Cross-sectional | Mothers with children from Uttar Pradesh and New Delhi | High maternal health literacy was associated with severe child stunting and being severely underweight. |
| Khanna & Khanna, 2023 [ | Letter to the Editor | General population | Highlights a significant research gap on the role of health literacy in India's extremely low cancer screening coverage. |
| Konsam et al., 2023 [ | Randomised controlled trial | Primigravid women from South India | A combined health literacy and relaxing music intervention significantly improved sleep quality and reduced the risk of antenatal depression. |
| Mittal, 2023 [ | Cross-sectional | Adult population from Haryana | Validated the All Aspects of Health Literacy Scale (AAHLS) in Hindi; found that higher socioeconomic status was associated with higher scores. |
| Muniyandi, 2015 [ | Cross-sectional | Saharia tribal population from Madhya Pradesh | 48% had never heard of tuberculosis (TB). Health literacy was very low, with general education being the only independent predictor. |
| Nagarjuna, 2023 [ | Cross-sectional | Hypertensive patients from a Maharashtra urban slum | Most participants (76.9%) had low health literacy, which was significantly associated with poor self-care management of hypertension. |
| Ogorchukwu, 2016 [ | Cross-sectional | Adolescents from Karnataka | Mental health literacy was very low; adolescents preferred informal help sources over formal ones due to pervasive stigma. |
| Passi et al., 2023 [ | Cross-sectional | Residents of a resource-poor village in Chandigarh | Identified eight distinct health literacy profiles, with challenges in actively managing health and finding good health information. |
| Rathnakar U.P. et al., 2013 [ | Cross-sectional | Patients in a tertiary care hospital in Karnataka | Younger age, higher education, and having a family physician were associated with better scores. |
| Saini, 2023 [ | Experimental study | Soldiers in Pune and Panchkhula | A community-based psycho-educational module significantly improved mental health literacy among troops, with gains stable at six months. |
| Saraf, 2018 [ | Cross-sectional | Adolescent girls in a Bengaluru urban slum | Mental health literacy regarding depression was low; stigma and lack of awareness were major barriers to seeking professional help. |
| Sharma et al., 2021 [ | Intervention evaluation | University students from Haryana | A mobile health intervention was a cost-effective method for improving eye health literacy. |
| Shikha et al., 2023 [ | Editorial | General | Emphasises that health literacy is crucial for maternal health, NCD prevention, and public health emergencies, influenced by diverse determinants. |
| Sil et al., 2017 [ | Cross-sectional | Caregivers of sick children from Eastern India | While caregivers showed good practical skills, significant knowledge gaps existed regarding medicine dosing, storage, and dosage intervals. |
| Singh, 2018 [ | Cross-sectional | Adult diabetic patients from Karnataka | 63% of diabetic patients had low health literacy, which was significantly correlated with poorer understanding of prescription instructions. |
| Sowmya et al., 2021 [ | Cross-sectional | Pre-school children and their mothers in Bangalore | Mothers' oral health literacy and behaviour were significantly associated with their children's dental caries experience. |
| Wu and Dubé, 2021 [ | Cross-sectional | Rural households from Odisha | Higher home-grown food consumption was associated with higher fruit and vegetable intake, and this effect was concentrated among those with low health literacy. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth Literacy and Information Accessibility · Global Maternal and Child Health · Global Public Health Policies and Epidemiology
Introduction and background
Health literacy is increasingly recognised as a foundational public health asset. It represents the capacity of individuals and communities to access, understand, appraise, and apply health information. This is crucial for making sound decisions regarding healthcare, disease prevention, and health promotion [1]. In India, with its vast demographic, linguistic, and social diversity, health literacy acts as a critical mediator that could alter the course of a wide range of public health challenges, ranging from the growing burden of non-communicable diseases to improving maternal and child health outcomes [2-4].
Previous Indian literature has successfully identified numerous linear associations, linking low health literacy to upstream determinants like education, socioeconomic status, and gender [5,6], and to downstream outcomes like poor medication adherence [7], uncontrolled hypertension [2], and child stunting [4]. However, these factors do not exist in isolation. The interplay between poverty, education, systemic mistrust, and the healthcare system itself creates a complex web of causality. These factors often interact and reinforce one another, creating "feedback loops" that trap populations in cycles of poor health outcomes and poverty. Low health literacy can lead to poor outcomes, which may foster mistrust in the health system. This mistrust, in turn, can lead to care avoidance, which further worsens health outcomes, creating a vicious cycle [8].
While many conceptual frameworks for health literacy exist, most remain qualitative in nature. To date, few studies have attempted to quantify these interactions and feedback loops in the Indian context. This gap leaves policymakers without the tools to understand why well-intentioned, isolated interventions may fail, or to identify which combination of interventions might be most effective [9]. Quantitative models enable the simulation of policies over time, allowing the testing of hypotheses about systemic behaviour and the identification of high-yielding interventions before committing resources in the real world. This study aims to address this gap by developing a conceptual model of health literacy contextual for India, grounded in a systematic review of the literature, to identify key feedback loops and to test the comparative effectiveness of different policy interventions via system dynamics modelling [10].
Review
Methods
This study was conducted in two phases: (1) a systematic review to identify determinants, pathways and outcomes to build a conceptual model of health literacy and gather parameters for subsequently building a Stock-and-Flow model, and (2) to simulate the impact of various policy scenarios.
Eligibility Criteria
This review included primary research studies, quantitative, qualitative, or mixed-methods studies, and editorials that discuss the determinants, pathways, and outcomes of health literacy and examine their linear relationships. To be included, studies had to be relevant to the Indian context and discuss the determinants, pathways, and outcomes of health literacy, as well as their relationships. Review articles were excluded from the analysis.
Search Strategy
A systematic search was conducted in PubMed and Google Scholar for articles published up to October 1, 2025. The review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [11]. The search strategy combined Medical Subject Headings (MeSH) and keywords relevant to the concept of health literacy, including terms such as "functional," "communicative," and "critical health literacy", and the location of the study, including names of specific states (Appendix 1).
The search yielded 549 records from the PubMed database and 10 from Google Scholar. After removing duplicates, two independent reviewers screened titles and abstracts. This resulted in 39 articles selected for full-text review. We were unable to retrieve four of these records. Of the 35 full-text articles assessed for eligibility, 30 studies met the final inclusion criteria and were included in the review (Figure 1). Data from the 30 included studies were extracted onto a data extraction sheet. Key variables extracted included study design, setting, population, Health literacy measurement tool, and key findings, with a specific focus on quantitative effect measures and qualitative themes related to determinants and pathways. The quality appraisal of the included studies was conducted using the Mixed Methods Appraisal Tool (MMAT).
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram
Model Building
The extracted data was first synthesised into a qualitative Causal Loop Diagram (CLD) to map the system's structure. This process identified the core components (Determinants, Pathways, Outcomes) and three key feedback loops that govern the system's behaviour, a vicious cycle of disparity (Reinforcing Loop 1, or R1), a vicious cycle of system mistrust (Reinforcing Loop 2, or R2), and a virtuous cycle of empowerment (Balancing Loop 1, or B1). The CLD was then quantified into a Stock-and-Flow simulation model using Python (v3.10) [12] with NumPy and Matplotlib libraries [13,14]. The model can be understood as a system of four interconnected stocks representing key population segments and system states. The simulation tracks how the distribution of 100 million people across these stocks changes over a 30-year period (Appendix 2).
Population with low health literacy: this stock is depleted by the health literacy improvement flow, which represents individuals gaining health literacy and moving to the population with high health literacy stock. Functionally, this stock represents the at-risk population. The model applies the effect of low health literacy on health [2], causing this population to transition to a state of poor health at an accelerated rate.
Population with high health literacy: health literacy improvement flow from the low health literacy population fills it. Functionally, this is the "protected" population. The model applies a protective effect of high health literacy on health [4], causing individuals in this stock to enter a state of poor health at a slower rate.
Population with poor health outcomes: This stock is our primary outcome indicator. It is filled from both the low health literacy and high health literacy stocks and is depleted by the recovery outflow.
Public trust: This stock is measured on a 0-100 scale. It is filled by a trust-building flow and depleted by a trust erosion flow. If the population with poor health outcomes stock exceeds a predefined threshold, the trust erosion flow is activated, and public trust declines. Functionally, this stock creates "policy resistance," as a decline in trust renders empowerment interventions less effective (Appendices 3, 4).
Policy Scenarios
We simulated five policy scenarios, with all interventions activated at Year 5 of the 30-year run. Scenario A (Baseline), a "do nothing" scenario, represents the system's natural trajectory. Scenario B (Empowerment) tests an IEC health literacy intervention [15-17]. Scenario C (Disparity Mitigation) tests a hypothesised social support policy aimed directly at the health outcome. Scenario D (Trust-Building) tests a policy focused on improving healthcare quality and system trust. A hypothesised intervention, such as provider communication training. Scenario E (Stacked Interventions) simulates a multi-pronged, systemic strategy by activating Scenarios B, C, and D simultaneously (Appendix 5).
We conducted a 100-run bootstrap sensitivity analysis. In each run, data-driven parameters were sampled from normal distributions defined by their 95% CIs and assumed parameters were varied by ±20%. We report the mean results for all scenarios and the 95% CIs for Scenarios A and E.
Results
Systematic Review and Model Structure
A summary of the included studies is provided in Table 1. A narrative synthesis approach was used to develop the conceptual model. Data on determinants, pathways, and outcomes were synthesized thematically. Causal statements and reported effect sizes were then mapped, translating the synthesised narrative into a Causal Loop Diagram visualised in Figure 2.
Causal Loop Diagram of Health Literacy NCDs: non-communicable diseases; SES: socioeconomic status
Determinants of Health Literacy
These are the upstream, socio-ecological factors that shape an individual's health literacy. Education is consistently identified as one of the strongest predictors. A study among diabetic patients in Mangalore found a significant association between educational status and health literacy [35]. Similarly, a study in Gujarat identified illiteracy as a significant factor associated with a higher likelihood of tobacco consumption [3]. Socioeconomic status is also critical; inadequate oral health literacy was found to be significantly associated with lower and lower-middle socioeconomic status [2,19]. Age and gender were also significant determinants [5,6,25].
Systemic barriers compound individual factors. A profound urban-rural divide exists, with rural populations having significantly lower health literacy on diseases like tuberculosis [29]. Social structures, such as caste, were also found to be strongly associated with health literacy levels [8]. Finally, India's vast linguistic diversity [20] creates further barriers, necessitating tools adapted to local contexts and languages [21,28].
Core Dimensions of Health Literacy
This is the central, multidimensional capacity that is influenced by the determinants. The data highlights a set of core skills [38]. These include Functional Literacy (basic reading/numeracy) [7,35], Communicative/Interactive Literacy (engaging with providers), and Critical Literacy (appraising information) [28]. The literature maps to a four-step patient journey of accessing information and care, understanding it, appraising its quality, and applying it to make a decision [2,4,28].
Mediating Pathways
These are extra steps that operate between the central components of health literacy and poor health outcomes. Low literacy is linked to delayed care-seeking. This delay is often mediated by a fear of "loss of daily wages", weighed against the perceived health risk [8]. Poor health literacy is significantly associated with poor self-care practices for non-communicable diseases (NCDs) like hypertension [2]. A lack of knowledge (functional literacy) is a significant predictor of harmful behaviours, such as tobacco use [3]. Higher maternal health literacy is strongly associated with better child nutritional status, an outcome of preventive behaviours [4]. Low parental health literacy is associated with pediatric medication dosing errors [7].
Health and System-Level Outcomes
These pathways culminate in population-level outcomes. Low health literacy is strongly linked to poor self-care management of hypertension [2]. High maternal health literacy was found to be strongly protective, halving the likelihood of severe child stunting [4]. Gaps in mental health literacy compromise help-seeking for conditions like depression and antenatal depression [27,30]. A critical outcome is the level of trust in the health system; mistrust and communication barriers act as a barrier to care [24].
Key Feedback Loops
The three key feedback loops that governed the behaviour of this dynamic system (Figure 2) are listed below.
R1 - The health disparity trap (vicious cycle): This loop illustrates how socioeconomic disadvantage is translated into poor health, thereby reinforcing the initial disadvantage. Lower socioeconomic status and education [19,6] lead to low health literacy, which leads to poor health behaviours [3,7] and poor self-care [2]. This results in poor health outcomes (e.g., poor hypertension management; child stunting [2,4]), which leads to reduced economic productivity [8], reinforcing the lower socioeconomic status.
R2 - The system trust spiral (vicious cycle): This loop explains how the system resists improvement. Poor outcomes and difficult-to-navigate systems (driven by R1) lead to mistrust in the health system [24]. This mistrust fosters care avoidance and delayed care-seeking, allowing conditions to worsen and leading to even poorer health outcomes, which further reinforces the initial mistrust.
B1 - The community empowerment cycle (balancing loop): This loop represents the primary pathway for intervention. The data show that targeted interventions are effective [31,33]. They lead to improved health behaviours, such as increased birth preparedness, which in turn lead to better health outcomes, e.g., reduced antenatal depression [15,27]. This improvement "closes the gap," counteracting the negative loops.
Policy Scenarios Simulation Results
We simulated five policy scenarios over 30 years to compare their effectiveness in reducing the population with poor health outcomes. The mean results of all five scenarios are presented in Figure 3.
Policy Scenarios Analysis
The baseline (Scenario A), or do nothing, showed a steady increase in the population with poor health, stabilising at a mean of 55.6 million with 95% CI 43.8M-65.5M by Year 30. The 'Health Disparity Trap' (R1) is fully active, with low health literacy driving a high sickness rate. The 'System Trust Spiral' (R2) is also active; as the population with poor health outcomes remains high, trust continuously erodes, suppressing any natural improvement in health literacy. The 'Community Empowerment Cycle' (B1) is inactive, with only a small baseline rate of health literacy improvement occurring, leading to the system being "stuck" in its vicious cycles, causing the population with poor health outcomes stock to fill and stabilise at the worst possible outcome.
Scenario B (Empowerment) only reduced the mean population with poor health outcomes to 52.6M. This scenario activates the B1 loop by applying the effectiveness of the intervention [15,17]. The health literacy improvement flow is turned on, accelerating the movement of people from the population with low health literacy to the population with high health literacy stock. This intervention does not directly mitigate the high sickness rate from R1, and its effectiveness is actively suppressed by the policy resistance created by eroding trust from the R2 loop.
Scenario C (Disparity Mitigation) was the most effective single lever, reducing the mean population with poor health outcomes to 45.5 million. This scenario tests a hypothesised social support policy. While it is the most direct and effective single intervention, it treats the symptom (poor health) without addressing the root causes (low health literacy and low system trust).
Scenario D (Trust-Building) reduced the mean population with poor health outcomes to 49.4 million. This scenario tests a policy focused on improving healthcare quality and system trust. A hypothesised intervention, such as provider communication training, that addresses the R2 loop. This policy acts in two ways: it reduces the total sickness inflow to simulate higher quality care, and it activates the trust-building flow to begin refilling the public trust stock. It helps improve outcomes and system resilience, but fails to address the large population with low health literacy.
The Stacked Intervention (Scenario E), which combined all three policy levers simultaneously, was the only scenario to show a powerful, synergistic effect, reducing the mean population with poor health outcomes to 35.7 million. The interventions cease to conflict and begin to reinforce one another. The trust-building flow refills the public trust stock, which lifts the policy resistance and amplifies the power of the Empowerment intervention (Scenario B). This, in turn, accelerates the depletion of the high-risk population with low health literacy stock, weakening the R1 disparity trap. As the population's poor health outcomes stock falls due to the combined effects of Scenarios B, C, and D, the trust erosion flow of the R2 loop breaks, creating a virtuous cycle where rising trust further boosts empowerment. This is the only scenario designed to break both vicious cycles (R1 and R2) while strengthening the virtuous cycle (B1). However, its 95% confidence interval (CI: 24.9M-47.6M) still showed a minor overlap with the lower bound of the baseline's CI (43.8M).
Discussion
The model demonstrates that the system is currently dominated by two powerful, reinforcing (vicious) cycles: the "Health Disparity Trap" (R1) and the "System Trust Spiral" (R2). R1 shows how social and economic disadvantage are converted into poor health, which in turn reinforces that disadvantage. R2 explains why this inequity is so persistent, as it erodes the trust required for the system to function, leading to a cycle of disengagement.
Our simulation shows that a standalone empowerment program (Scenario B) is likely to underperform. Our model suggests this is due to "policy resistance" from the R2 loop; as trust erodes, the effectiveness of the empowerment intervention is suppressed. This simulated 'policy resistance' aligns with qualitative evidence from the review, which found that significant mistrust and challenging family dynamics in clinical settings can create barriers to patient agency and informed decision-making, even when relevant health information is available [24]. The Stacked Intervention (Scenario E) produced a mean result (35.7M) far superior to any isolated intervention, suggesting a powerful synergistic effect. However, the most critical finding from our sensitivity analysis is the persistent uncertainty. The overlap between the 95% CIs of the stacked (24.9M-47.6M) and baseline (43.8M-65.5M) scenarios indicates uncertainty in the effectiveness, given the wide variance in the parameters. Future research could potentially address this uncertainty and improve model precision through more precise effect size estimates.
Conclusions
This is the first study in India to apply system dynamics modelling to synthesise the evidence on health literacy, providing a novel tool for understanding systemic feedback and policy simulation. It demonstrates that the system is dominated by reinforcing feedback loops that link social disadvantage, low literacy, and system mistrust, perpetuating health inequities. Our model provides a quantitative argument that to solve this complex problem, we must move from isolated projects to a sustained, systemic, and multi-pronged strategy. However, our simulation also highlights that the high variance in intervention effectiveness is a critical barrier, emphasising the need for more robust, scalable intervention models and research to validate them.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Health literacy and public health: a systematic review and integration of definitions and models BMC Public Health Sørensen K Van den Broucke S Fullam J Doyle G Pelikan J Slonska Z Brand H 801220122227660010.1186/1471-2458-12-80PMC 3292515 · doi ↗ · pubmed ↗
- 2Role of health literacy and primary health-care access in self-care management of hypertension Indian J Public Health Nagarjuna P Kumar V Faujdar DS Yadav AK 4424476720233792938810.4103/ijph.ijph_1704_22 · doi ↗ · pubmed ↗
- 3Health literacy and tobacco cessation among hypertensive individuals: a mixed method study J Educ Health Promot Chauhan D Patel D Yogesh M Trivedi N 3801320243970366010.4103/jehp.jehp_1922_23PMC 11657896 · doi ↗ · pubmed ↗
- 4Maternal health literacy is associated with early childhood nutritional status in India J Nutr Johri M Subramanian SV KonéGK 1402141014620162730689510.3945/jn.115.226290 · doi ↗ · pubmed ↗
- 5Association between maternal health literacy and child vaccination in India: a cross-sectional study J Epidemiol Community Health Johri M Subramanian SV Sylvestre MP 8498576920152582746910.1136/jech-2014-205436 PMC 4552929 · doi ↗ · pubmed ↗
- 6Evaluation of health literacy status among patients in a tertiary care hospital in coastal Karnataka, India J Clin Diagn Res Rathnakar UP Belman M Kamath A Unnikrishnan B Shenoy AK Udupa AL 25512554720132439239810.7860/JCDR/2013/6120.3608 PMC 3879879 · doi ↗ · pubmed ↗
- 7A study of knowledge, attitude and practice regarding administration of pediatric dosage forms and allied health literacy of caregivers for children J Family Med Prim Care Sil A Sengupta C Das AK Sil PD Datta S Hazra A 636642620172941702210.4103/2249-4863.214433 PMC 5787969 · doi ↗ · pubmed ↗
- 8Health literacy strengths and challenges among residents of a resource-poor village in rural India: epidemiological and cluster analyses PLOS Glob Public Health Passi R Kaur M Lakshmi PV Cheng C Hawkins M Osborne RH 03202310.1371/journal.pgph.0001595 PMC 1002201236963029 · doi ↗ · pubmed ↗