Management of malignant breast phyllodes tumor with rib invasion during pregnancy: a rare case report and literature review
Sijie Yu, Panni Li, Wenwen Wu, Xianan Guo, Huihui Chen, Kexin Liu, Dan Ye, Zhihua Teng, Wei He, Liquan Wang, Yunxiang Zhou, Yiding Chen

TL;DR
A rare case of malignant breast phyllodes tumor invading the rib during pregnancy was successfully treated with surgery, ensuring a healthy pregnancy outcome.
Contribution
This is the first documented case of complete resection of a rib-infiltrating malignant phyllodes tumor during pregnancy.
Findings
Radical extended resection with chest wall reconstruction was successfully performed in the second trimester without complications.
No local recurrence or metastasis was observed at six-month follow-up.
The case contributes insights into the management of pregnancy-associated malignant phyllodes tumors.
Abstract
Phyllodes tumors of the breast are rare fibroepithelial neoplasms accounting for less than 1% of breast tumors, with malignant phyllodes tumors (MPTs) representing approximately one-quarter of cases. Occurrence during pregnancy is exceedingly uncommon and may be associated with accelerated tumor growth. We report a 32-year-old woman at 15 weeks of gestation with a two-year history of recurrent MPT who had undergone four prior excisions. During the current pregnancy, the tumor recurred with rapid progression and rib invasion. After multidisciplinary evaluation, radical extended resection with chest wall reconstruction using the latissimus dorsi muscle was performed in the second trimester without perioperative complications. The pregnancy continued uneventfully, and a healthy full-term infant was delivered. At six-month follow-up, no local recurrence or metastasis was detected. Herein,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
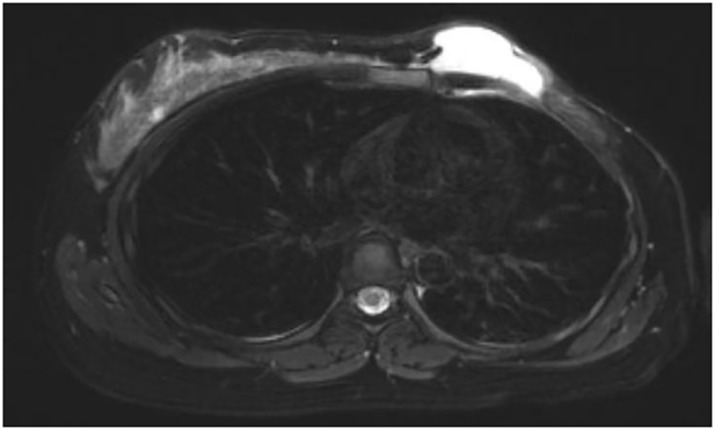 Figure 1
Figure 1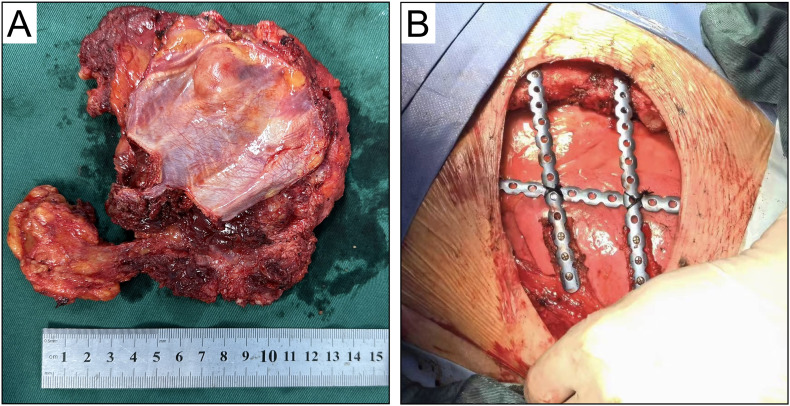 Figure 2
Figure 2 Figure 3
Figure 3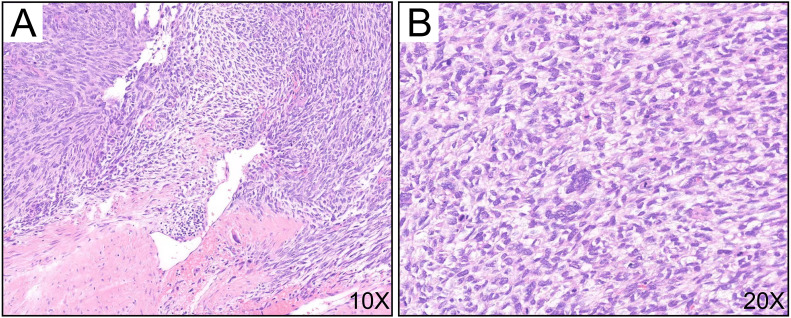 Figure 4
Figure 4| Time | Disease development | Size (cm) | Surgical approach | Pathology | Ki-67 |
|---|---|---|---|---|---|
| 2021.7 | Simple mass in the left breast | 4*2 | Simple lumpectomy of the left breast mass | Benign | NA |
| 2022.11 | Recurrence of a mass in the left breast | 2*1.5*1 | Left mastectomy | Malignant | 30%+ |
| 2023.10.11 | Left chest wall local recurrence | NA | Excision of the lesion in the left chest wall1 | Malignant | 50%+ |
| 2023.11.16 | Left chest wall local recurrence | NA | Excision of the lesion in the left chest wall1 | Malignant | 80%+ |
| 2023.12.13 | Recurrence on the left chest wall with invasion into the ribs | 4*3.5 | Radical extended surgery of the left chest wall | Malignant | 60%+ |
| First author, year | Age, year | Gestation presentation | Size (cm) | Recurrence | Rapid growth in pregnancy | Operation period | Surgical approach | Pathology | Follow up |
|---|---|---|---|---|---|---|---|---|---|
| Bal 2012 ( | 32 | Postpartum period | Whole breast | Y | Y | NR | SA+SLNB+IBR | Malignant | 6 m: free of disease |
| Blaker 2010 ( | 27 | 9th week | 4 | N | N | 11 weeks | WLE | Malignant | 8 m: free of disease |
| Hernanz 2018 ( | 35 | 14th week | 7.6 (R) | N | Y | 14 (R)/23 (L) weeks gestation | RB: SA+IBR | Malignant | Safe before labor1 |
| Kelten 2016 ( | 37 | 4 weeks | 13 | N | Y | 4 weeks after labor | SM | Malignant | NR |
| Lee 2018 ( | 21 | NR | 2.9 | N | N | NR | Lumpectomy | Malignant | NR |
| Li 2008 ( | 29 | 6 months | Whole breast (36*28) | Y | Y | 6 months after labor | SM; then WLE and flap | Malignant | NR |
| Mrad 2000 ( | 32 | NR | 9 (R), | N | NR | NR | RB: WLE | RB: Benign | 17 m: free of disease |
| Mustață 2021 ( | 36 | 19th week | 10 | N | Y | 35 weeks | SM | malignant | 4 y: free of disease |
| Narla 2018 ( | 28 | Postpartum period | 14 | N | Y | NR | lumpectomy; then SM | Malignant | NR |
| Nejc 2008 ( | 28 | 34th week | 18 | N | Y | 2 weeks after labor | WLE | Malignant | 20 m: free of disease |
| Pacchiarotti 2011 ( | 41 | 17th week | 6 | N | Y | During pregnancy | WLE | Malignant | NR |
| Pasta 2012 ( | 43 | T2 | 1.5 | N | N | During pregnancy | WLE | Malignant | 1 y: free of disease |
| Pytel 2009 ( | 25 | T2 | NR | N | Y | 2 years after labor | SM | Malignant | NR |
| Ray 2011 ( | 24 | 36th week | 22 | N | Y | 8 weeks after labor | SM | Malignant | NR |
| Simpson 2007 ( | 29 | 20th week | 17 | N | Y | 22 weeks | WLE+SLNB | Malignant | NR |
| Tortoriello 2017 ( | 37 | T1 | 24 | N | Y | NR | Lumpectomy | Malignant | 2.5 y: free of disease |
| Vergine 2012 ( | 27 | Postpartum period | 10 | N | Y | NR | SM | Malignant | 1 y: free of disease |
| Zhang 2021 ( | 38 | T1 | 6 | Y | Y | 3 years after labor | SM | Malignant | 1.5 y after surgery, lung metastasis |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Lesions and Carcinomas · Cancer Risks and Factors · Breast Cancer Treatment Studies
Introduction
1
Phyllode tumors of the breast (PTBs) are rare fibroepithelial neoplasms characterized by a distinctive leaf-like histological pattern (1). They account for 2.5% of all fibroepithelial lesions of the breast and 0.3% to 1% of all primary breast tumors (2, 3), with a higher prevalence in Asia (4, 5), most commonly occurring in women aged 35 to 55 years (6, 7). Although relatively uncommon, these tumors exhibit a high propensity for recurrence (8). PTBs typically present as rapidly growing, painless masses, averaging 3 to 5 cm in size. In cases of large tumors, conspicuous congested veins, skin surface ulceration, or chest wall invasion may be observed. According to the latest WHO classification criteria in 2019, PTBs are pathologically categorized into benign, borderline, and malignant based on stromal cellular atypia, the proportion of mitotic figures, the degree of stromal overgrowth and necrosis (9). Among these, malignant phyllodes tumors (MPT) constitute approximately 25% of cases, with local recurrence rates of 23% to 30% and a distant metastasis rate of around 9% (1, 2). Despite ongoing controversies regarding the comprehensive management of MPT, adequate surgical excision remains the standard approach to achieve optimal local control (10). This study reports a rare and highly challenging case of recurrent MPT complicated by rapid progression and rib invasion, necessitating complex surgical management aimed at achieving complete tumor resection while preserving gestation. Beyond the case illustration, we provide a literature review to delineate the clinicopathological characteristics and comprehensive management of MPTs, with a focus on surgical approaches and on the specific considerations for pregnancy-associated cases.
Case presentation
2
A 32-year-old woman was admitted to the hospital with a chief complaint of enlargement and recurrence of a left breast mass for two years. Prior to this, she underwent multiple surgeries due to recurrent left breast masses, with specific diagnostic and treatment processes outlined in Table 1. It was two years ago when the patient first discovered a left breast mass during a routine physical examination. She underwent a segmental resection of the mass, with postoperative pathology revealing a benign PTB. One year later, during a follow-up visit, the left breast mass recurred. A biopsy confirmed the presence of an MPT, with no evidence of lymph node metastasis in the axilla. Consequently, the patient underwent a total mastectomy of the left breast, postoperative pathology indicated an MPT measuring approximately 21.51.0 cm. No adjuvant chemotherapy or radiotherapy was administered after the surgery. The patient became pregnant over two months ago, during which a nodule on the left chest wall was detected. She subsequently underwent two excisional surgeries under local anesthesia at an external hospital, with postoperative pathology confirming an infiltrative recurrence of the MPT. The patient is now experiencing skin ulceration and mass formation on the left chest wall and is currently 15 weeks and 4 days of gestation. She was admitted for further treatment of the left breast MPT as well as to preserve the pregnancy. As shown in Figure 1, preoperative chest magnetic resonance imaging (MRI) revealed a left chest wall mass suggesting recurrence of a PTB, classified as BI-RADS 4C, with invasion into the chest wall and close proximity to the pleura. Given the aggressive growth rate of this dangerous tumor, surgical excision to prevent further growth and metastasis is the primary objective.
Preoperative breast MRI imaging. Transverse T2 revealed a left chest wall mass suggesting recurrence of a phyllode tumors of the breast, classified as BI-RADS 4C, with invasion into the chest wall and close proximity to the pleura.
Considering the patient’s mid-pregnancy status and the tumor’s invasion into the chest wall and ribs, the breast surgery team initiated a preoperative MDT discussion involving thoracic surgery, obstetrics, anesthesiology, and orthopedics. All disciplines conducted a comprehensive analysis of the treatment plan. MPTs are not sensitive to chemotherapy or radiotherapy (11), and given the patient’s pregnancy and elevated hormone levels that could promote rapid tumor growth, the surgical indication was clear, with the primary goal being radical tumor excision. Thus, with the support of various specialties, the patient underwent “radical excision of the left chest mass” under general anesthesia on December 13, 2023. The surgery lasted 4 hours, and through careful intraoperative monitoring and meticulous handling, the malignant tumor was completely excised (Figure 2A). The surgery team removed the left 4th and 5th ribs and performed chest wall reconstruction with titanium plates (Figure 2B). Then the latissimus dorsi muscle was utilized to fill the chest wall defect (Figure 3), and the fetus was not significantly affected during the perioperative period, continuing to grow well. Postoperative pathology confirmed a recurrence of MTB (Figure 4), with a 1 cm excision margin.
Radical extended resection of tumor and chest wall reconstruction. (A) specimen of left breast malignant phyllodes tumor after extended resection; (B) Removed the left 4–5 ribs and performed chest wall reconstruction with titanium plates.
Early postoperative aspect after radical extended resection of the tumor, with left breast reconstruction using the latissimus dorsi muscle.
H and E staining of the tumor. Recurrence of breast malignant phyllodes tumor, demonstrating infiltrative tumor growth, with marked atypia of tumor cells and a markedly increased cellularity (>10/HPF). (A) H and E staining; magnification, ×10; (B) H and E staining; magnification, ×20.
Postoperatively, the patient recovered well. She successfully delivered a healthy child on May 24, 2024. Follow-up outpatient visits over the next six months indicated good recovery, with no signs of local recurrence or distant metastasis detected.
Discussion and literature review
3
MPTs are rare and typically require aggressive surgical management due to their tendency for recurrence and metastasis. Adequate surgical excision with clear margins remains the standard approach for non-metastatic MPT (10). According to the National Comprehensive Cancer Network (NCCN) guidelines, the optimal approach for conservative surgery involves excising a margin of at least 1 cm or more (12). A negative margin serves as an independent prognostic factor for disease-free survival (DFS) and local recurrence in PTB. For malignant and borderline tumors, wider excision is recommended, as shown in the guideline, the risk of recurrence and metastasis is higher when margins are less than 1 cm. In this case, the patient had already undergone a total mastectomy during previous recurrences, and the current lesion had infiltrated the ribs from the residual chest wall. To achieve complete excision and minimize the risk of recurrence, a radical resection involving the chest wall and the 4th and 5th ribs was performed, with both superior and inferior margins being negative. In cases of significant tissue defects following large PTB excision, reconstructive techniques such as tissue flap transfer can be employed, as demonstrated by the latissimus dorsi flap reconstruction in this case. Previous studies indicate that the axillary involvement rate of MPT is only 1% to 3% (3, 13, 14). As the therapeutic value of axillary lymph node (ALN) removal remains uncertain, ALN dissection or surgical staging of the axilla is generally not performed unless clear clinical or pathological evidence of ALN involvement exists (10). Given that preoperative imaging in this patient indicated no significantly enlarged or abnormal ALNs, we did not perform ALN biopsy or dissection.
While the established role of surgical excision in treating MPT is undeniable, the significance of postoperative radiotherapy continues to be uncertain. Two large retrospective studies, in which 455 of 2261 and 458 of 3210 patients received adjuvant radiotherapy, respectively, reported no improvement in long-term survival for MPT (15, 16), although adjuvant radiotherapy was associated with a significant reduction in local recurrence (16, 17). Similarly, a meta-analysis highlighted that while adjuvant radiotherapy effectively improves local disease control in PTB, it does not confer a survival benefit (18). Currently, adjuvant radiotherapy may be selectively considered for high-risk MPT, such as tumors with high-grade histology, size >5 cm, or positive surgical margins (3). Furthermore, the use of adjuvant chemotherapy remains controversial due to its limited clinical benefits (19). However, when the tumor metastasizes or surgery is not feasible, chemotherapy and radiotherapy appear to reduce recurrence rates and prevent disease progression. In this case, the patient did not undergo adjuvant radiotherapy or chemotherapy postoperatively and remained in good health during follow-up.
Beyond being a rare instance of PTB, our case is particularly distinctive due to the involvement of a rapidly growing MPT occurring in the first trimester of pregnancy. Pregnancy-associated breast cancer (PABC) is defined as breast cancer diagnosed during pregnancy or within one year postpartum (20). In cases of early-stage PABC, if postoperative treatment such as radiotherapy or chemotherapy is not required, the pregnancy may continue. For PABC, there is no evidence suggesting that therapeutic abortion improves prognosis (21). Treatment plans should be individualized, and prior to starting therapy, each pregnant patient should be thoroughly informed about the treatment options, their impact on pregnancy, and potential teratogenic effects. The decision to continue or terminate the pregnancy is a personal one. Surgical management of breast cancer during pregnancy should follow the same guidelines as for non-pregnant women. However, due to the increased risk of miscarriage, it is generally recommended to postpone surgery until after the first trimester (22). As mentioned above, MPT can exempt patients from chemotherapy and radiotherapy, so despite the lack of formal guidelines, continuation of pregnancy with MPT can still be considered. Specifically, the patient in this case, who had not conceived in six years of marriage and had previously undergone curettage for a missed abortion, was determined to preserve the pregnancy after being informed of the associated risks. Given the necessity for surgical intervention and the imperative to ensure maternal-fetal safety, an MDT approach was employed. Ultimately, with the cooperation of various specialties, the surgery was successfully completed. The MDT model allowed for optimal allocation of healthcare resources, enhanced quality control, and facilitated interdisciplinary decision-making, ultimately improving the patient’s clinical outcome.
Actually, PTB during pregnancy accounts for only 25% of all PTBs (23), while MPT is even rarer. A comprehensive review pertaining to pregnancy-associated breast MPT was conducted of the existing literature. Overall, fewer than 20 case reports of MPT during pregnancy and lactation have been reported, but there are some interesting consistencies. Information from each case report is summarized in Table 2 (24–41). The mean age of the patients was 31.6 years, with 50% diagnosed during the first or second trimester of pregnancy. The average size of these malignant tumors is 12.8 cm (ranging from 1.5 to 32cm), with most exhibiting a rapid growth rate during pregnancy. Notably, 17.8% of the cases were recurrent tumors. Similarly, the patient in this case experienced multiple recurrences of the PTB. Despite four local excisions, the tumor continued to infiltrate the ribs. Prognostic factors influencing disease recurrence include tumor size, grade, postmenopausal status, necrosis, cellular atypia, infiltrative margins, and positive surgical margins (42). In these reports, it is suspected that pregnancy played a significant role in the recurrence. Hormonal changes during pregnancy may stimulate proliferative changes in breast glandular tissue, such as lobular and acinar growth, potentially contributing to both recurrence and accelerated tumor progression. As shown in Table 2, 14 out of 18 MPTs (77.8%) exhibited rapid enlargement during pregnancy or lactation, highlighting the potential hormone dependence of MPTs. However, due to the relatively limited number of MPTs during pregnancy, further research is needed to confirm a definitive link between pregnancy-related hormonal changes and MPT pathogenesis. Moreover, due to the characteristic rapid growth of MPT during pregnancy, breast examination in early pregnancy is particularly important. Among previously reported cases, only three patients underwent phyllodes tumor resection in the mid-early stages of pregnancy (25, 26, 38), with the earliest case involving a partial mastectomy at 11 weeks of gestation (25). Early detection and timely management theoretically increase the rate of breast conservation and reduce the occurrence of complications.
Notably, PTB can also metastasize, posing significant challenges in treatment. PTB primarily metastasizes through hematogenous rather than lymphatic routes (43), with metastases mainly observed in patients with MPT. The most common metastatic sites for MPT are the lungs and bones, though metastases to adrenal glands and the brain can occur concurrently (44). Once patients with MPT develop distant metastases, the prognosis is extremely poor, with a median survival time of 10.7-11.5 months (43). Therefore, gaining a deeper understanding of the mechanisms underlying the development and progression of PTB is crucial. Dios et al. (45) proposed that PTBs may be associated with MED12 mutations. Additionally, there are theories suggesting that tumor-associated macrophages promote the transformation of PTB into malignant forms by facilitating fibroblast activation (46). For individuals with recurrent disease or high-risk factors, relevant genetic testing can be conducted to explore potential molecular biological therapeutic targets for PTB. Furthermore, patients with MPT during pregnancy are typically younger, necessitating the consideration of hereditary breast cancer risks. Genetic testing may also guide patients in managing reproductive choices and assessing hereditary breast cancer risks for future generations.
This study has inherent limitations. As a case-based review, this study is restricted by the single-patient nature of the report, which limits the generalizability of its observations, particularly in complex clinical settings such as malignant phyllodes tumors occurring during pregnancy. Robust evidence on this topic remains scarce, and higher-level studies including prospective multicenter cohorts, randomized controlled trials when feasible, and meta-analyses based on such data are needed to refine clinical guidelines and clarify optimal management strategies. Until stronger evidence becomes available, treatment decisions should be individualized with careful consideration of tumor biology, expected surgical outcomes, maternal and fetal factors, and patient preferences.
Conclusions
4
In summary, this study reports a rare case involving a patient with an MPT of the breast that recurred and affected the ribs, while also pregnant at the time of admission. The patient underwent a complex radical resection while simultaneously requiring treatment to preserve the pregnancy. PTBs that develop during pregnancy typically exhibit a faster growth rate and may be prone to multiple recurrences or malignant transformation. In patients with rapidly growing breast tumors, particularly during pregnancy, there should be a high suspicion for MPT. Multiple recurrences can alter the nature and invasiveness of PTBs, making vigilance crucial when signs of recurrence appear. This is especially important for women of childbearing age or those planning pregnancy, who should undergo breast examinations prior to ruling out any potential risks, enabling early detection and timely, effective treatment. To reduce the risk of tumor recurrence, standardized treatment strategies need to be established. Complete surgical excision remains the preferred treatment for non-metastatic PTB, while the efficacy of adjuvant radiotherapy and chemotherapy in PTB management remains uncertain. In complex cases, such as those involving recurrent breast tumors during pregnancy, an MDT approach is particularly crucial for standardized diagnosis and treatment. Future clinical studies with more in-depth analysis are needed to explore the diagnosis and treatment of PTB at various stages.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Telli ML Horst KC Guardino AE Dirbas FM Carlson RW . Phyllodes tumors of the breast: natural history, diagnosis, and treatment. J Natl Compr Canc Netw. (2007) 5:324–30. doi: 10.6004/jnccn.2007.0027, PMID: 17439760 · doi ↗ · pubmed ↗
- 2Lissidini G MulèA Santoro A Papa G Nicosia L Cassano E . Malignant phyllodes tumor of the breast: a systematic review. Pathologica. (2022) 114:111–20. doi: 10.32074/1591-951X-754, PMID: 35414723 PMC 9248247 · doi ↗ · pubmed ↗
- 3De Lauretis F Sanchez AM Accetta C Carnassale B D'Archi S Di Leone A . Malignant mesenchymal tumors of the breast: current challenges and new perspectives on primary sarcomas and Malignant phyllodes tumors. Life (Basel). (2025) 15(4):673. doi: 10.3390/life 15040673, PMID: 40283227 PMC 12028549 · doi ↗ · pubmed ↗
- 4Chua CL Thomas A Ng BK . Cystosarcoma phyllodes–Asian variations. Aust New Z J Surgery. (1988) 58:301–5. doi: 10.1111/j.1445-2197.1988.tb 01060.x 2855393 · doi ↗ · pubmed ↗
- 5Tan PH Jayabaskar T Chuah KL Lee HY Tan Y Hilmy M . Phyllodes tumors of the breast: the role of pathologic parameters. Am J Clin Pathology. (2005) 123:529–40. doi: 10.1309/U 6DVBFM 81MLJC 1FN 15743740 · doi ↗ · pubmed ↗
- 6Salvadori B Cusumano F Del Bo R Delledonne V Grassi M Rovini D . Surgical treatment of phyllodes tumors of the breast. Cancer. (1989) 63:2532–6. doi: 10.1002/1097-0142(19890615)63:12<2532::AID-CNCR 2820631229>3.0.CO;2-Q 2541890 · doi ↗ · pubmed ↗
- 7Testori A Meroni S Errico V Travaglini R Voulaz E Alloisio M . Huge Malignant phyllodes breast tumor: a real entity in a new era of early breast cancer. World J Surg Oncol. (2015) 13:81. doi: 10.1186/s 12957-015-0508-7, PMID: 25880837 PMC 4350953 · doi ↗ · pubmed ↗
- 8Yu CY Huang TW Tam KW . Management of phyllodes tumor: A systematic review and meta-analysis of real-world evidence. Int J Surg. (2022) 107:106969. doi: 10.1016/j.ijsu.2022.106969, PMID: 36328344 · doi ↗ · pubmed ↗