The Peking Health Anxiety Scale for Infectious Diseases: psychometric properties and short-form development
Junkai Feng, Yixuan Wang, Yinyin Zang

TL;DR
Researchers developed a new scale to measure health anxiety during infectious disease outbreaks, like the pandemic, and tested its reliability and usefulness.
Contribution
The study introduces the PHAID, a new and validated tool specifically for measuring health anxiety related to infectious diseases.
Findings
The PHAID has a two-factor structure (Catastrophic Thinking and Infection Worries) with strong reliability and validity.
The PHAID-S short form maintains good reliability and screening accuracy.
PHAID scores correlate with handwashing behaviors, distinguishing normal from excessive anxiety.
Abstract
Health anxiety can escalate rapidly during infectious disease outbreaks, yet existing assessment tools lack specificity for such contexts. This study aimed to develop and validate the Peking Health Anxiety Scale for Infectious Diseases (PHAID), a brief, context-sensitive measure tailored to infectious disease-related health anxiety. The PHAID was adapted from the Short Health Anxiety Inventory, with items revised to focus on COVID-19. Psychometric validation was conducted in a sample of 1,660 adults recruited primarily from the United States via Amazon’s MTurk during the COVID-19 pandemic. Factor structure was determined using exploratory and confirmatory factor analyses. Reliability, convergent and discriminant validity, and test–retest stability were assessed. A clinical cutoff and the relationship with preventive behaviors were examined. A 5-item short form (PHAID-S) was developed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
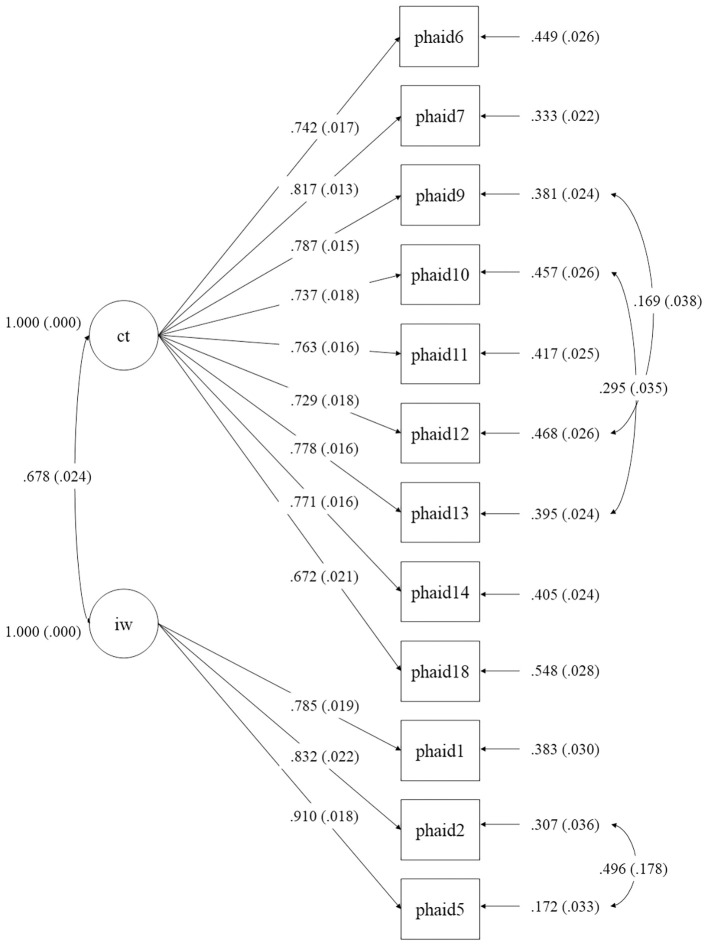 Figure 1
Figure 1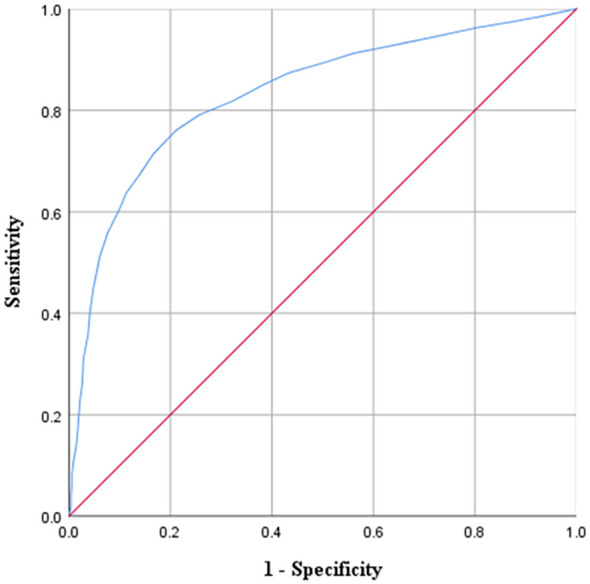 Figure 2
Figure 2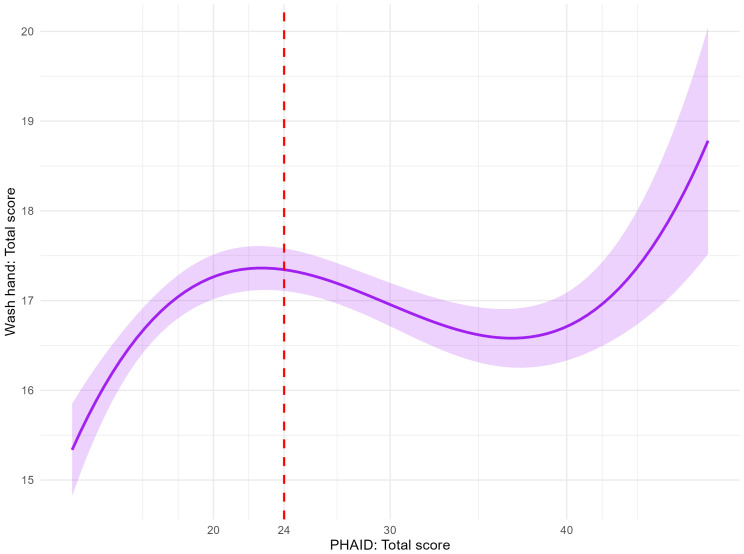 Figure 3
Figure 3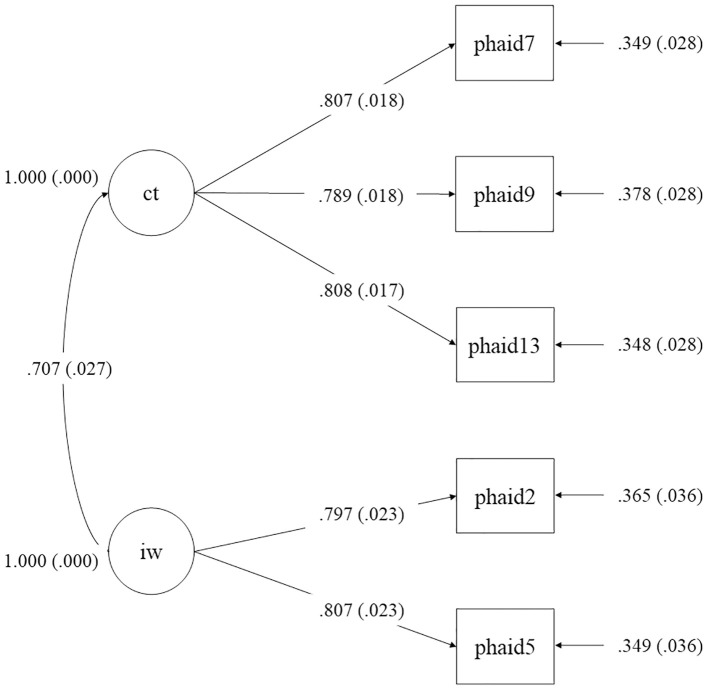 Figure 4
Figure 4| Items | Factors 1 catastrophic thinking | Factors 2 infection worries |
|---|---|---|
| 9. If I hear about COVID-19, I think I have it myself. |
| -0.203 |
| 12. I think that I have COVID-19. |
| -0.088 |
| 18. If I had COVID-19, I would feel that I had lost my dignity. |
| -0.129 |
| 13. If I notice an unexplained bodily sensation, I would think about COVID-19 all the time, and I find it difficult to think about other things. |
| 0.032 |
| 7. I have difficulty taking my mind off thoughts about COVID-19. |
| 0.113 |
| 14. My family/friends would say I worry too much about COVID-19. |
| 0.069 |
| 6. I have images of myself getting COVID-19. |
| 0.111 |
| 10. If I have a bodily sensation or change, I wonder whether I have COVID-19. |
| 0.142 |
| 11. I usually feel at risk for developing COVID-19. |
| 0.259 |
| 16. If I have COVID-19, there is a small chance that modern medicine would be able to cure me. |
| 0.045 |
| 1. I worry about contracting COVID-19 | 0.113 |
|
| 5. I am afraid of contracting COVID-19. | 0.219 |
|
| 2. I am more afraid of contracting COVID-19 compared with most other people of my age. | -0.125 |
|
| 8. I am relieved if my doctor tells me I do not have COVID-19. | 0.378 |
|
| Dimensions/items | Total score | Catastrophic thinking | Infection worries |
|---|---|---|---|
| Catastrophic Thinking | 0.975*** | – | – |
| Infection Worries | 0.777*** | 0.619*** | – |
| 1. I worry about contracting COVID-19. | 0.634*** | – | 0.876*** |
| 2. I am more afraid of contracting COVID-19 compared with most other people of my age. | 0.719*** | – | 0.874*** |
| 5. I am afraid of contracting COVID-19. | 0.692*** | – | 0.888*** |
| 6. I have images of myself getting COVID-19. | 0.780*** | 0.789*** | – |
| 7. I have difficulty taking my mind off thoughts about COVID-19. | 0.821*** | 0.826*** | – |
| 9. If I hear about COVID-19, I think I have it myself. | 0.774*** | 0.793*** | – |
| 10. If I have a bodily sensation or change, I wonder whether I have COVID-19. | 0.785*** | 0.766*** | – |
| 11. I usually feel at risk for developing COVID-19. | 0.736*** | 0.786*** | – |
| 12. I think that I have COVID-19. | 0.797*** | 0.821*** | – |
| 13. If I notice an unexplained bodily sensation, I would think about COVID-19 all the time, and I find it difficult to think about other things. | 0.716*** | 0.756*** | – |
| 14. My family/friends would say I worry too much about COVID-19. | 0.634*** | 0.789*** | – |
| 18. If I had COVID-19, I would feel that I had lost my dignity. | 0.692*** | 0.835*** | – |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and Mental Health · Vaccine Coverage and Hesitancy · Psychology of Moral and Emotional Judgment
Introduction
1
Health anxiety refers to persistent worries and fear about the perceived threats to one’s health (1–3). Conceptualized as a continuum, it ranges from minimal health awareness to excessive anxiety, previously termed hypochondriasis (4). According to the cognitive-behavioral model, this anxiety is maintained by maladaptive processes, including the catastrophic misinterpretation of bodily sensations and safety-seeking behaviors (4–6).
Illness-related events can trigger health anxiety (7), with infectious disease outbreaks such as SARS, H1N1 influenza, and COVID-19 acting as especially potent stressors (8). Several features make infectious diseases particularly anxiety-provoking: their transmission can be covert and unpredictable, often involving aerosols or asymptomatic carriers (9–14). Moreover, the physical symptoms of anxiety (e.g., shortness of breath, chest tightness) can closely mimic those of infectious diseases, leading to misinterpretation of benign sensations (15). Additionally, the perceived severity and lethality of certain infectious diseases can intensify fears of infection and death (16). Together, these factors create a context in which health anxiety can escalate rapidly during infectious disease outbreaks. While severe health anxiety is linked to higher risks of mental disorders (e.g., depression and generalized anxiety; 17, 18), impaired stress coping (19, 20), and reduced quality of life (21), moderate levels can motivate adaptive behaviors during pandemics, such as social distancing, improved hygiene, and information seeking (22).
However, existing health anxiety scales and their cutoff scores were developed for general health concerns, not for the unique context of infectious disease outbreaks (e.g., anxiety about diseases like cancer; 23, 24). Infectious diseases present acute, population-wide threats that can rapidly shift what is considered adaptive versus maladaptive anxiety. As such, there is a critical need for measurement tools and empirically validated cutoffs specifically designed to assess health anxiety related to infectious diseases, to support research, clinical care, and public health responses.
To address this gap, the present study developed and validated the Peking Health Anxiety Scale for Infectious Diseases (PHAID). The scale adapts items from the widely used Short Health Anxiety Inventory (SHAI, 23), a decision grounded in its strong psychometric properties and its alignment with the cognitive-behavioral model of health anxiety. While developed in China, the PHAID was validated in an international sample to assess its utility beyond a single cultural context, acknowledging the global nature of infectious disease threats and as a first step toward establishing broader cross-cultural validity.
This study aimed to: (1) develop the PHAID and examine its factor structure; (2) evaluate its reliability, validity, and test-retest stability; (3) establish a preliminary clinical cutoff score; and (4) develop and validate a psychometrically sound short form (PHAID-S). We hypothesized that the PHAID would demonstrate a stable factor structure, excellent reliability, and strong validity, providing a context-sensitive tool to enhance the identification of clinically significant health anxiety during infectious disease outbreaks.
Methods
2
Participants
2.1
Data was collected at two points. At Time 1 (August-October 2020), 1,660 participants were recruited from Amazon Mechanical Turk (MTurk), an international platform accessible to anyone with internet and English proficiency. No geographical restrictions were applied, resulting in a naturalistic, international sample primarily from the United States (n = 1,136, 68.4%), India (n = 209, 12.6%), Brazil (n = 117, 7.0%), Canada (n = 66, 4.0%), Italy (n = 38, 2.3%), and 94 participants (5.6%) from 29 other countries. Participants were compensated $0.90 USD. The study was approved by the Peking University IRB (No.: 2020-04-18).
Eligibility criteria included informed consent, correct responses to an embedded validity check (judging the size of a common animal relative to a human; 25). Individuals with a confirmed COVID-19 diagnosis were excluded. This was necessary to ensure the scale specifically measured the fear of contracting the virus, rather than capturing the distinct psychological responses, such as illness-related distress or anxiety about recovery, that follow a confirmed infection, which would confound the construct of interest. The final Time 1 sample comprised 821 men, 830 women, and 9 individuals of other genders, with a mean age of 36.94 years (SD = 11.97).
Time 2 data were collected one month after Time 1, in November 2020. Following the same inclusion criteria, 355 participants were retained (181 men and 174 women), with a mean age of 39.21 years (SD = 12.69). Due to the high attrition rate (21.4%), a logistic regression analysis was conducted to examine potential attrition bias between participants who completed both time points (n = 355) and those who completed only the baseline assessment (n = 1,305). The analysis revealed that younger age (OR = 0.97, p < 0.001), higher baseline health anxiety (OR = 1.06, p < 0.001), and US residency (OR = 1.69, p < 0.001) were significant predictors of attrition. While this indicates some systematic patterns in dropout, the follow-up sample remains adequate for test-retest reliability analysis, though estimates should be interpreted with the understanding that they may be slightly conservative due to the selective attrition of more anxious participants.
The participant’s characteristics are shown in Supplementary Table S1 in the supplementary material.
Measures
2.2
Peking Health Anxiety Scale for Infectious Diseases
2.2.1
The PHAID is a 12-item scale designed to assess health anxiety in the context of infectious disease outbreaks, with its initial validation focused on COVID-19. The PHAID was adapted from the SHAI through a structured process to ensure content validity. First, an expert panel of two doctoral-level clinical psychologists systematically revised all items to focus on COVID-19-related health anxiety. Next, this adapted version was pilot-tested with a group of psychology students and practicing therapists to evaluate item clarity and relevance. Their feedback was used to refine the wording, resulting in the final item pool for psychometric evaluation. The measure was developed by adapting an initial pool of 18 items from the Short Health Anxiety Inventory (26). The content was revised to specify COVID-19 by (1) replacing general references to “illness” with “COVID-19,” (2) emphasizing the risk of contagion (e.g., “I am afraid of contracting COVID-19”). The reference period was set as “during the past six months,” corresponding to the pandemic timeframe. All items are rated on a 4-point Likert scale (1 = never to 4 = always), with higher scores indicating greater COVID-19-related health anxiety. After exploratory factor analysis, four items were removed due to low loadings or excessive cross-loading, yielding the final 12-item version. Although the PHAID was developed for COVID-19, its structure allows for straightforward adaptation to other public health emergencies. By substituting the relevant disease name in each item, the scale can be rapidly tailored to assess health anxiety related to future infectious disease outbreaks or similar public health events.
Hospital Anxiety and Depression Scale
2.2.2
The HADS (27) is a 14-item scale with two 7-item subscales for anxiety (HADS-A) and depression (HADS-D). Each item is rated from 0 to 3, with higher scores indicating greater symptom severity. A subscale score of 8 or above indicates clinically significant anxiety or depression (28). Cronbach’s alpha in this study was.74.
Handwashing
2.2.3
Handwashing was measured with four items, each assessing the frequency of proper hand hygiene (using soap and water or hand sanitizer) in a specific scenario during the past three days: arriving home, before cooking or eating, after coughing or sneezing, and after using the restroom. All items are rated on a 5-point Likert scale (1 = never to 5 = always). Cronbach’s alpha in this study was.81.
Statistical analysis
2.3
All analyses were conducted using SPSS 25, Mplus 8.3, and R. Parallel analysis, exploratory factor analysis (EFA), assessments of convergent and discriminant validity, internal consistency, test-retest reliability, Receiver Operating Characteristic (ROC) analysis, and Pearson correlations were performed in SPSS. Confirmatory factor analysis (CFA) was conducted in Mplus. Item Response Theory (IRT) analysis was performed in R using the ltm package.
To determine the factor structure of the PHAID, the full Time 1 sample (n = 1,660) was randomly split into two equal subsamples (n = 830 each). The first subsample was used for EFA. Prior to EFA, a parallel analysis was conducted to determine the number of factors to retain, which involved comparing actual data eigenvalues with the 95th percentile of eigenvalues from 1,000 simulated random datasets (29, 30). Factors were retained if the i-th eigenvalue from the data exceeded the corresponding random value (31, 32). EFA was performed using principal axis factoring with Promax (oblique) rotation (33). Items were iteratively removed if they had a factor loading below 0.35 or a cross-loading difference less than 0.2 between primary and secondary factors.
A series of CFAs were conducted in the second subsample to evaluate and compare three competing models: (1) the original SHAI factor structure, (2) the two-factor structure derived from EFA, and (3) a modified version of the EFA-based model. For the EFA-derived model, items with loadings below 0.50 were excluded. In line with methodological recommendations to avoid overfitting (34), model modifications were made only for a limited number of item pairs that demonstrated both high modification indices (MI > 10, 35) and a strong, a priori substantive rationale based on close semantic content. The model fit was evaluated against conventional standards (36). An adequate model fit was indicated by 1 < χ^2^/df < 3, comparative fit index (CFI) and Tucker Lewis index (TLI) values ≥ 0.90, root-mean-square-error of approximation (RMSEA) ≤ 0.08 (more liberal) or ≤ 0.05 (stricter), and standardized root-mean-square residual (SRMR) value ≤ 0.05.
Scale validity and reliability were assessed via multiple methods. Convergent validity was evaluated by correlating the PHAID total score with the HADS anxiety subscale; discriminant validity was assessed via correlation with the HADS depression subscale. Internal consistency was estimated using Cronbach’s alpha for the total scale and subscales. Test-retest reliability was assessed by correlating PHAID scores at Time 1 and at the one-month follow-up (Time 2).
To establish a clinical cutoff for the PHAID, ROC analysis was conducted using the HADS anxiety subscale and its established cutoff (28) as the reference standard. Regression analyses were performed to examine the relationship between PHAID total score and hand washing total score. Multiple models (linear, quadratic, cubic, power, logarithmic, and exponential) were tested, and model fit was compared using adjusted R². Notably, the regression analysis examining the relationship between PHAID scores and handwashing was conducted for exploratory purposes to investigate the form of this relationship, rather than to build a predictive model.
Item Response Theory (IRT) analysis was conducted to inform the development of a short form (PHAID-S). A Graded Response Model (GRM, 37) was fitted to the data. For each item, two parameters were estimated: a discrimination parameter (a) and three difficulty parameters (b1, b2, b3), corresponding to the thresholds between the four ordered response categories (0-3). Test Information Curves (TIC) and Item Information Curves (IIC) were also calculated to evaluate the measurement precision of the scale and its individual items across the latent trait of health anxiety. A ROC analysis was also conducted to establish a cutoff of PHAID-S.
Results
3
Exploratory factor analysis
3.1
The data were suitable for EFA, as indicated by a significant Bartlett’s test of sphericity (p <.001) and a high Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy (0.945). Parallel analysis supported the extraction of two factors, with the actual eigenvalues for the first two factors exceeding the 95th percentile eigenvalues from simulated random data (see Supplementary Table S2 in supplementary material). Item 4 was removed due to a factor loading below 0.30, and Items 17, 15, and 3 were subsequently removed due to excessive cross-loadings. The final solution, presented in Table 1, consisted of two factors that collectively accounted for 61.93% of the total variance. All retained items demonstrated strong loadings, ranging from 0.51 to 0.89. Negative cross-loadings are a known artifact of oblique rotation and should be interpreted in the context of the strong primary loadings and the inter-factor correlation. Based on the content of the items, Factor 1 was labeled Catastrophic Thinking, and Factor 2 was labeled Infection Worries.
Confirmatory factor analysis
3.2
The original SHAI factor structure showed all standardized factor loadings were statistically significant (p <.01 for item 4; p <.001 for all others); however, model fit was poor: χ²/df = 10.04, p <.001, CFI = .843, TLI = .821, RMSEA = .104, SRMR = .061. The two-factor EFA-derived structure required the removal of Items 8 and 16 due to loadings below 0.50. All remaining items loaded significantly (p <.001), and model fit improved substantially: χ²/df = 7.94, p <.001, CFI = .941, TLI = .927, RMSEA = .091, SRMR = .046. Moreover, error covariances were added for three pairs: item 12 and 9 (self-diagnosis), item 13 and 10 (misinterpretation of bodily sensations), and item 5 and 2 (core fear of infection). The modified model (see Figure 1) demonstrated excellent fit: χ²/df = 6.53, p <.001, CFI = .956, TLI = .942, RMSEA = .082, SRMR = .040.
Path diagram of the revised two-factor structure from confirmatory factor analysis (CFA) of the PHAID, showing standardized factor loadings. ct, Catastrophic Thinking; iw, Infection Worries. Standardized coefficients were shown.
Internal consistency
3.3
As presented in Table 2, Pearson correlation analyses revealed strong and statistically significant positive associations (all p <.001). The correlations between the total score and the two subscales were very high, ranging from 0.619 to 0.975. Similarly, all items showed strong correlations with the total score (r = 0.634 to 0.821), and with their respective subscales (r = 0.756 to 0.835 for Catastrophic Thinking; r = 0.874 to 0.888 for Infection Worries). The Cronbach’s alpha and McDonald’s omega were excellent: α = 0.931 and ω = .947 for the total scale, α = 0.928 and ω = .939 for the Catastrophic Thinking subscale, and α = 0.851 and ω = .856 for the Infection Worries subscale.
Test–retest reliability
3.4
One-month test–retest correlations were high for the total score (r = 0.826, p <.001), as well as for the Catastrophic Thinking (r = 0.780, p <.001) and Infection Worries (r = 0.821, p <.001) subscales.
Convergent and discriminant validity
3.5
The PHAID total score and its subscales showed significant, moderate-to-strong positive correlations with the HADS anxiety subscale, supporting convergent validity (PHAID total: r = 0.622, Catastrophic Thinking: r = 0.617, Infection Worries: r = 0.454; all ps <.01). In contrast, correlations with the HADS depression subscale were weaker (PHAID total: r = 0.263, Catastrophic Thinking: r = 0.267, Infection Worries: r = 0.175; all ps <.01). The association between the PHAID total score and anxiety was significantly greater than with depression (ZH = 15.45, p <.001), supporting the convergent and discriminant validity of the PHAID.
ROC analysis for cutoff determination
3.6
The ROC curve for the PHAID, using the HADS anxiety subscale (cutoff ≥ 8) as the criterion, yielded an area under the curve (AUC) of 0.83 (p <.001, 95% CI [0.81, 0.85]; see Figure 2). The optimal cutoff score was 24 on the PHAID total, corresponding to the maximum Youden’s index of 0.550. At this threshold, sensitivity was 0.760 and specificity was 0.790. Sensitivity, specificity, and Youden’s index values for additional cutoff scores are presented in Supplementary Table S3 in supplementary material.
ROC curves for PHAID. PHAID, Peking Health Anxiety Scale for Infectious Diseases.
The relationship between PHAID total scores and hand washing total score was best described by a cubic regression model (adjusted R² = .02), as shown in Figure 3. The cubic model demonstrated a significant overall fit, F(3, 1656) = 13.81, p <.001. All predictors were statistically significant: linear term (b = 1.39, t = 5.91, p <.001), quadratic term (b = −0.05, t = −5.60, p <.001), and cubic term (b = 0.0006, t = 5.30, p <.001). Compared to the cubic model, the quadratic, power, logarithmic, exponential, and linear models accounted for less variance (adjusted R² = .007,.005,.005,.002, and.002, respectively). The cubic regression curve indicated that hand washing total score increased with PHAID scores up to a total score of 24, plateaued between scores of 24 and 36, and increased again at higher scores. It is important to note that this regression analysis was exploratory in nature. The low adjusted R² confirms that health anxiety is just one of many factors influencing handwashing, and the PHAID is not intended to predict this behavior. The key finding is the significant non-linear pattern itself, which provides preliminary construct validity by aligning with the theoretical model of adaptive versus maladaptive anxiety.
Cubic regression of PHAID scores on hand washing total score. PHAID, Peking Health Anxiety Scale for Infectious Disease. The red dashed line indicates the PHAID cutoff point of 24.
Item Response Theory analysis for short-form development
3.7
All items showed discrimination parameters greater than 2.87. For Catastrophic Thinking, Items 9 (a = 3.21, b1 = -0.08, b2 = 0.74, b3 = 1.63), 13 (a = 2.89, b1 = -0.39, b2 = 0.66, b3 = 1.72), and 7 (a = 2.87, b1 = -0.43, b2 = 0.65, b3 = 1.63) had the highest discrimination and provided the most information according to the Item Information Curves. For Infection Worry, Items 5 (a = 3.68, b1 = -1.39, b2 = -0.03, b3 = 0.98) and 1 (a = 3.38, b1 = -1.67, b2 = -0.16, b3 = 0.96) had the highest discrimination and information values. These five items were selected for the PHAID-S. The 5 selected items adequately represent the core content of the original factors: the Catastrophic Thinking factor is represented by three high-discrimination items covering difficulty disengaging from thoughts, self-diagnosis, and persistent rumination, while the Infection Worries factor is represented by its two most central items (general worry and fear).
Confirmatory factor analysis was conducted to evaluate the two-factor structure of the 5-item PHAID-S. The model demonstrated an excellent fit to the data: χ²/df = 9.55, p <.001, CFI = .981, TLI = .953, RMSEA = .102, SRMR = .026. All standardized factor loadings were statistically significant (p <.001) and substantial, ranging from 0.79 to 0.81 for the Catastrophic Thinking factor (Items 7, 9, 13) and from 0.80 to 0.81 for the Infection Worries factor (Items 2, 5), as shown in Figure 4.
Path diagram of the two-factor structure from confirmatory factor analysis (CFA) of the PHAID-S, showing standardized factor loadings. ct, Catastrophic Thinking; iw, Infection Worries. Standardized coefficients were shown.
Test Information Curves showed maximum measurement precision for Catastrophic Thinking in the latent trait range of -0.5 to 1.5, and for Infection Worry in the range of -1.5 to 1.0 for both PHAID and PHAID-S, indicating that the PHAID-S covers a similar range of the latent trait as the full PHAID, although with a lower peak information. The short form demonstrated internal consistency of Cronbach’s α = 0.85. Detailed parameter estimates and information curves are presented in Supplementary Table S4 and Supplementary Figures S1–S4 in the supplementary materials.
For the PHAID-S, ROC analysis (criterion: HADS anxiety subscale ≥ 8) yielded an AUC of 0.81 (p <.001, 95% CI [0.81, 0.85]; see Supplementary Figure S3). The optimal cutoff score for the PHAID-S was 11, corresponding to the maximum Youden’s index of 0.470. However, considering the utility of a short form for efficient screening, a cutoff of 12 may also be considered, as it offers substantially higher specificity (0.845 vs. 0.744) for a moderate decrease in sensitivity (0.653 vs. 0.727), which could be preferable in settings where minimizing false positives is a priority. The cutoff of 11 is recommended for maximum sensitivity. Additional cutoff statistics are provided in Supplementary Table S5 in the supplementary material.
Discussion
4
This study developed and validated the Peking Health Anxiety Scale for Infectious Diseases (PHAID), a domain-specific screener designed to identify clinically significant anxiety related to transmissible illnesses. Through psychometric evaluation in a large sample primarily recruited via an online platform MTurk (n = 1,660), we established a stable two-factor structure (Catastrophic Thinking and Infection Worries) with excellent reliability (total scale α = 0.931, test-retest r = 0.826) and validity (stronger correlation with anxiety than depression). Although developed during the COVID-19 pandemic, the PHAID’s focus on common respiratory symptoms (e.g., cough, fever, dyspnea) allows for its adaptation to similar infectious disease contexts, including H1N1 influenza and SARS (38, 39). The PHAID offers a practical framework for assessing infection-focused cognitions and worries during public health emergencies.
The PHAID is the first measure specifically adapted and validated during the COVID-19 pandemic to assess the distinct construct of health anxiety within an infectious disease context. The research landscape has seen the rapid development of various tools to capture pandemic-related distress, including scales for fear (fear of COVID-19 scale, FCV-19S; 40), unidimensional anxiety (COVID-19 anxiety scale, CAS; 41, 42), maladaptive coping syndromes (COVID-19 anxiety syndrome scale, C-19ASS; 43), and broader stress responses (COVID Stress Scales, CSS; 44). (a) lack specificity for its defining cognitive features (e.g., the FCV-19S); (b) focus on the behavioral manifestations and coping strategies rather than the core health-related fears (e.g., the C-19ASS); (c) are often impractical for rapid screening due to their length and complexity (e.g., the CSS); and crucially, (d) are not theoretically grounded in the cognitive-behavioral model of health anxiety. The PHAID directly addresses these gaps by providing a concise, theoretically grounded tool that specifically targets and dissects the core cognitions (Catastrophic Thinking) and health-related fears (Infection Worries) characteristic of infectious disease health anxiety, thereby enabling precise identification and intervention (45).
The screening utility and clinical relevance of the PHAID were strengthened by establishing an empirically derived cutoff score of 24. ROC analysis demonstrated a favorable balance between sensitivity (76%) and specificity (79%), with performance characteristics comparable to established psychiatric screening tools, such as the State-Trait Inventory for Cognitive and Somatic Anxiety (STICSA; 46) and the General Health Questionnaire (GHQ; 47). The clinical significance of this cutoff was supported through behavioral validation examining the relationship between PHAID scores and handwashing frequency. An exploratory cubic regression analysis revealed a significant, theoretically meaningful pattern: scores approaching the cutoff were associated with increasing hand hygiene, consistent with adaptive health vigilance (22). Beyond this threshold, protective behaviors plateaued, while severely elevated scores (around 36) showed renewed increases—a pattern potentially indicating a shift toward compulsive responding (48). Although this preliminary finding requires further validation, it suggests the PHAID may help differentiate adaptive vigilance from potentially excessive anxiety responses, supporting its construct validity as a tool to identify individuals who could benefit from further assessment during outbreaks.
The study also developed a 5-item short form (PHAID-S) that maintains good reliability (α = 0.85) despite substantial length reduction. Derived through Item Response Theory, the PHAID-S retains high discrimination power in the low-to-moderate severity range, making it well-suited for rapid screening in time-sensitive clinical settings, large-scale public health surveys, and repeated monitoring during treatment. This brief format provides an efficient alternative for initial screening, while the full scale remains preferable for comprehensive assessment requiring finer gradations, particularly at higher severity levels.
Limitations & future directions
4.1
Several limitations of this study should be acknowledged. First, participants were recruited via Amazon Mechanical Turk (MTurk). While this platform enabled the collection of a geographically diverse sample, the participant pool may overrepresent. White, middle-class individuals with higher education levels and computer literacy. Moreover, while our sample included participants from multiple countries, its online nature and Western predominance warrant caution regarding cultural generalizability. Second, the data were collected during the early stages of the COVID-19 pandemic (August-November 2020). The psychological impact and associated health anxiety may have evolved as the pandemic progressed, and public health policies varied across regions. Consequently, the results might underestimate the potential severity of such anxiety in later phases of the pandemic or in regions experiencing severe outbreaks. Third, the test-retest reliability assessment was limited by the sample size, and attrition analysis revealed that the dropout was not completely random but was influenced by age, nationality, and baseline health anxiety scores. Future studies should collect more unbiased longitudinal data to further examine the scale’s temporal stability. Fourth, while the PHAID demonstrates good convergent validity with general anxiety (HADS-A) and discriminant validity from depression (HADS-D), its direct convergent validity with a measure of health anxiety itself (e.g., the full Short Health Anxiety Inventory) was not assessed in this study. Fifth, the interpretation of the significant cubic relationship with handwashing is exploratory and requires validation in studies specifically designed to test this behavioral pattern.
Future research can focus on several key areas to extend the utility of the PHAID. First, validating the PHAID and its short form across more diverse populations—including varied cultural, socioeconomic, and clinical groups—would help establish its broader applicability and stability across different contexts. Second, future studies could explore how factors such as media exposure, health literacy, and pre-existing vulnerabilities influence PHAID. Third, future studies could investigate how varying levels of PHAID scores correlate with a spectrum of health behaviors, from appropriate vigilance to excessive actions. Fourth, the clinical and public health utility of the PHAID cutoff scores could be evaluated in real-world settings to assess their effectiveness in identifying individuals who might benefit from targeted support.
Conclusion
5
The PHAID demonstrates good psychometric properties through its validated two-factor structure, excellent reliability, and empirically derived cutoff score, addressing a critical measurement gap in infectious disease-related health anxiety. As an early-stage tool, the PHAID shows potential to provide researchers and clinicians with an evidence-based instrument for identifying individuals who may benefit from targeted support during public health emergencies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abramowitz JS Braddock A . Psychological treatment of health anxiety and hypochondriasis: A biopsychosocial approach. Göttingen, Germany: Hogrefe publishing (2008).
- 2Bailer J Kerstner T Witthoft M Diener C Mier D Rist F . Health anxiety and hypochondriasis in the light of DSM-5. Anxiety Stress Coping. (2016) 29:219–39. doi: 10.1080/10615806.2015.1036243, PMID: 25846805 · doi ↗ · pubmed ↗
- 3Jungmann SM Witthoft M . Health anxiety, cyberchondria, and coping in the current COVID-19 pandemic: Which factors are related to coronavirus anxiety? J Anxiety Disord. (2020) 73:102239. doi: 10.1016/j.janxdis.2020.102239, PMID: 32502806 PMC 7239023 · doi ↗ · pubmed ↗
- 4Taylor S Asmundson GJ . Treating health anxiety: A cognitive-behavioral approach. New York, USA: Guilford Press New York (2004).
- 5Marcus DK Gurley JR Marchi MM Bauer C . Cognitive and perceptual variables in hypochondriasis and health anxiety: a systematic review. Clin Psychol Rev. (2007) 27:127–39. doi: 10.1016/j.cpr.2006.09.003, PMID: 17084495 · doi ↗ · pubmed ↗
- 6Salkovskis PM Warwick HM . Morbid preoccupations, health anxiety and reassurance: a cognitive-behavioural approach to hypochondriasis. Behav Res Ther. (1986) 24:597–602. doi: 10.1016/0005-7967(86)90041-0, PMID: 3753387 · doi ↗ · pubmed ↗
- 7Stenning NJ . A meta-analytic investigation of the psychometric properties of the Health Anxiety Questionnaire and the Health Anxiety Inventory University of Leeds. (2017).
- 8Liu B Yang X Kong L . Classification of the infectious diseases. In: Li H , editor. Radiology of infectious diseases: volume 1. Philadelphia, USA: Springer Netherlands (2015). p. 29–30. doi: 10.1007/978-94-017-9882-2_5 · doi ↗