Maternal and Fetal Outcomes of Motor Vehicle-Related Trauma in Pregnancy: A Trauma Center Study
Avis L Chan, Kristina Roloff, Michael Neeki, Jessica Sparks, Guillermo J Valenzuela

TL;DR
This study examines how motor vehicle collisions affect pregnant women, finding that higher car speeds are linked to more severe injuries, but most injuries were minor due to seat belt use.
Contribution
The study identifies car speed as a key predictor of injury severity in pregnant trauma patients, while highlighting the protective role of seat belts.
Findings
Higher car speed was significantly associated with intra-abdominal injury and skin lacerations.
Most patients had no or minor injuries, likely due to high seat belt usage.
Pregnant individuals with higher parity tended to be involved in crashes at lower speeds.
Abstract
Objective The main objective of this study is to examine immediate outcomes, and the incidence of severe intra-abdominal injury after motor vehicle collisions (MVCs) in the pregnant population. Methods We conducted a retrospective cohort study. From 2015 to 2021, all pregnant patients who presented to a level I trauma center within 24 hours of MVC were included. Data on patient characteristics, collision details, hospital workup, and trauma-related injuries were extracted from their charts using ICD-10 code O9A.21. Descriptive statistics were used to summarize data. General linear models and univariate logistic regression models were used to analyze the relationship between variables. Results The study included 157 pregnant patients. Most were in their mid-20s, overweight to obese, multiparous, Hispanic, and in the second trimester. The median reported car speed was 30 mph (IQR…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
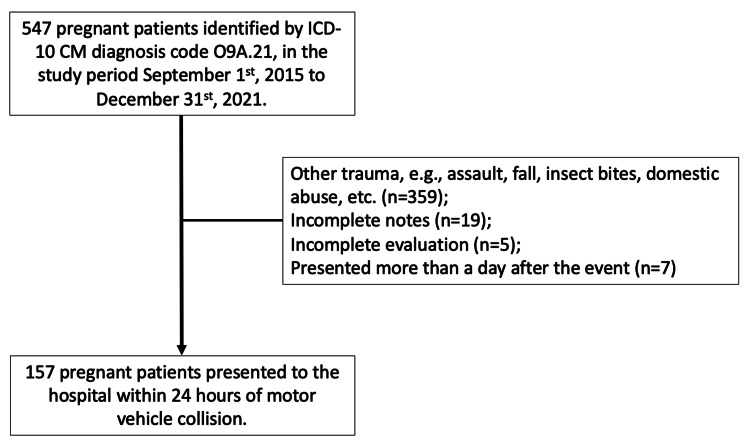 Figure 1
Figure 1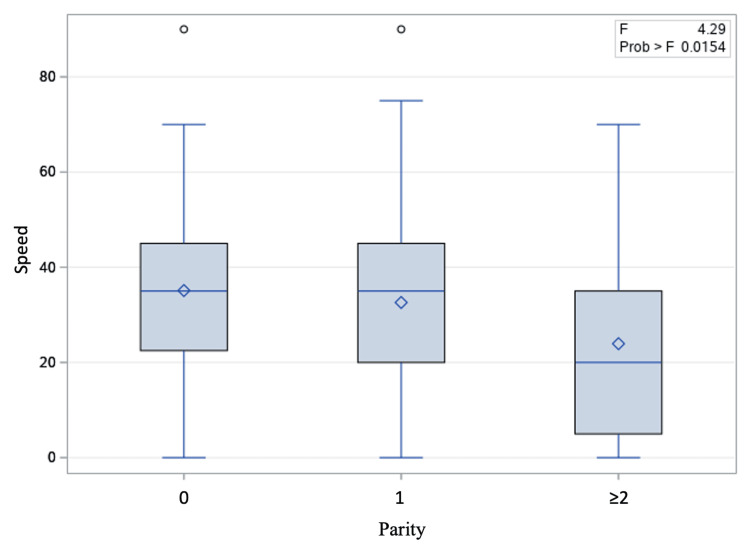 Figure 2
Figure 2| Patient characteristics | Value |
| Maternal age (years), mean ± SD | 27.0 ± 5.8 |
| Gestational age (weeks), mean ± SD | 24.4 ± 8.7 |
| Gravidity, median ± IQR | 2.0 ± 1.0 |
| Parity, median ± IQR | 1.0 ± 2.0 |
| BMI (kg/m2), mean ± SD | 31.1 ± 7.1 |
| Maternal height (inches), mean ± SD | 63.9 ± 2.6 |
| Race/ethnicity, N (%) | |
| Non-Hispanic White | 17 (10.8) |
| Hispanic | 117 (74.5) |
| Non-Hispanic Black | 18 (11.5) |
| Asian/Pacific Islander | 3 (1.9) |
| Others | 2 (1.3) |
| Collision characteristics | |
| Speed (mph), median ± IQR | 30.0 ± 35.0 |
| Use of seat belt, N (%) | 155/157 (98.7) |
| Occupant position at the time of collision, N (%) | |
| Front driver seat | 111/157 (70.7) |
| Front passenger seat | 41/157 (26.1) |
| Rear seat | 5/157 (3.2) |
| Collision point on the car, N (%) | |
| Front of the car | 34/157 (21.7) |
| Side of the car | 70/157 (44.6) |
| Back of the car | 50/157 (31.8) |
| Multiple areas | 3/157 (1.9) |
| Car rollover, N (%) | 8/157 (5.1) |
| Deployment of airbag, N (%) | 104/157 (66.2) |
| Hospital workup | |
| Seat belt sign, N (%) | 20/157 (12.7) |
| Peritoneal sign, N (%) | 2/157 (1.3) |
| Stated history of substance/alcohol use, N (%) | 4 (2.6) |
| Positive serum alcohol test, N (%) | 5/107 (4.7) |
| Positive urine toxicology screening, N (%) | 3/67 (4.4) |
| Ultrasound abdomen and pelvis, N (%) | 138/157 (87.9) |
| CT abdomen and pelvis, N (%) | 9/157 (5.7) |
| Maternal and fetal outcomes | Value |
| No obvious injury, N (%) | 133 (84.7) |
| Skin lacerations, N (%) | 24 (15.3) |
| Fractures, N (%) | 6 (3.8) |
| Hemoperitoneum, N (%) | 2 (1.3) |
| Intra-abdominal visceral organ injury, N (%) | 2 (1.3) |
| Placental abruption, N (%) | 1 (0.6) |
| Delivery at the admission episode, N (%) | 1 (0.6) |
| Fetal demise, N (%) | 1 (0.6) |
| Maternal death in hospital, N (%) | 0 |
| Length of hospital stay (days), median ± IQR | 1.0 ± 1.0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPregnancy-related medical research · Occupational Health and Performance · Gestational Diabetes Research and Management
Introduction
Motor vehicle collision (MVC) is a significant cause of trauma in pregnancy, leading to adverse maternal and fetal outcomes [1,2]. Three percent of pregnant individuals were involved in at least one MVC [3,4]. Maternal death occurred in 3.6 per 1,000, and fetal death or stillbirth in 6.76 per 1,000, based on a meta-analysis of 19 population-level studies [5]. The effects of blunt abdominal trauma can lead to a host of complications, including visceral organ injuries, bony fractures, placental abruption, preterm birth, low birth weight, exposure to multiple radiological examinations, and non-obstetric surgery [4-8]. Pregnant individuals are vulnerable to adverse consequences following MVC as a result of physiological, hemodynamic, and anatomical changes, which may hamper correct and timely diagnosis of visceral organ injury.
Much of the evidence on outcomes following MVC in pregnancy originates from national databases, such as the National Trauma Data Bank, National Automotive Sampling System/Crashworthiness Data System (NASS/CDS), Fatality Analysis Reporting System (FARS), Nationwide Inpatient Sample (NIS) database, and National Vital Statistics System (NVSS). Although these databases provide population-level data on over 10,000 subjects, they are prone to limitations in miscoding, over-generalization of diagnoses and conditions, and missing data [9]. Many studies appropriately conclude the need to study additional variables, such as collision characteristics, severity and type of trauma, car speed, occupant position, seat belt use, airbag deployment, demographics of occupants, and clinical data related to pregnancy, to better understand the relationship between MVC and injury outcomes in pregnant individuals [5].
This study, at a single trauma center, examines the immediate outcomes and the incidence of severe intra-abdominal injury, involving visceral organ laceration or rupture, after different types of MVC in the pregnant population.
Materials and methods
We performed a retrospective observational cohort study using a convenience sample, from September 1, 2015, to December 31, 2021, at a level-one trauma center and the second-busiest Emergency Department in Southern California. This study was approved by the Institutional Review Board (protocol #22-25). Patient consent was waived for retrospective chart reviews.
To reduce misclassification bias, we extracted all cases at the institution with the World Health Organization ICD-10-CM diagnosis code O9A.21 (injury, poisoning, and certain other consequences of external causes complicating pregnancy) from the electronic medical record [10]. Patient charts were then reviewed by trained investigators, and the final study cohort included cases that met the following inclusion criteria: (1) pregnancy of any gestational age, and (2) presentation to the institute within 24 hours of MVC. Cases were excluded if the charts were significantly incomplete or if the type of documented trauma was not an MVC. In a few cases in which patients had more than one encounter following MVC, we only included the first encounter.
Maternal age, gestational age, gravidity, parity, body mass index on hospital admission, body height, body weight, race/ethnicity, and self-reported substance or alcohol use prior to the MVC were extracted from the medical records. Race/ethnicity, as self-reported data, was combined into five major groups: non-Hispanic White, Hispanic, non-Hispanic Black, Asian/Pacific Islander, and others. Car speed, use of a lap and shoulder seat belt, occupant’s position within the car (driver, front passenger, and rear passenger) at the time of collision, collision point on the car, car rollover, and deployment of airbags were reported and extracted during chart review. Significant findings included the presence or absence of a seat belt sign, peritoneal signs, serum alcohol or urine toxicology screening, ultrasound, computed tomography (CT) scan, abdominal surgery, injury details, and length of hospital stay.
Descriptive statistics were used for patient characteristics, collision characteristics, and maternal and fetal outcomes. Chi-squared test or Fisher's exact test was used, where appropriate, for categorical variables, while Student’s t-test was used for continuous variables. General linear models were performed to examine the relationship between two continuous variables. In addition, univariate logistic regression models were run to explore the association between intra-abdominal visceral organ injury and other patient or collision characteristics. Data were analyzed using SAS® version 9.3 (SAS Institute, Cary, NC, USA). A p-value less than 0.05 was considered statistically significant.
Results
A total of 157 pregnant occupants were presented to the institute within 24 hours of an MVC for evaluation, from September 1, 2015, to December 31, 2021, in Figure 1.
Inclusion and exclusion chart for the motor vehicle collision study in pregnant individualsWorld Health Organization: ICD-10-CM diagnosis code O9A.21 [10].
Twenty-four patients were excluded due to incomplete documentation or incomplete evaluation. The majority of the patients were in their mid-20s, at least overweight to obese, with maternal height more than five feet, multiparous, Hispanic, and in their second trimester (Table 1). The median reported car speed was 30 mph (interquartile range (IQR) 10-45 mph). Of the total, 99% (N = 155) of patients reported use of seat belts, while 70% (N = 111) were drivers. Most collisions involved side impacts to the car. Only 5% (N = 8) of collisions involved rollover of the car, and there was no observed association between car rollover and speed (p = 0.1135). Airbags were deployed in 66% (N = 104) of the MVCs, and airbag deployment was statistically associated with car speed (p < 0.0001).
When patients presented to the hospital, 13% (N = 20) had seat belt signs, and only 1% (N = 2) had peritoneal signs, which led to exploratory laparotomy. Nearly 85% (N = 133) of patients had no or minor injuries (Table 2); 15% (N = 24) had skin lacerations; 4% (N = 6) had fractures; and 1% (N = 2) suffered intra-abdominal visceral organ injuries with hemoperitoneum.
The first of the two patients was 23 years old, gravida 2, para 1, eight weeks pregnant, and was brought in by ambulance after a head-on MVC at a speed of 90 mph. She was the restrained front-seat passenger. The airbag was deployed. She lost consciousness and suffered multiple extremity open fractures and lacerations. Hemoperitoneum was noted on focused assessment with sonography in trauma (FAST) and CT scans. An exploratory laparotomy was performed 33 minutes after arrival; findings revealed 150 mL of blood in the peritoneal cavity, a serosal tear over the cecum, a mesenteric hematoma, and hepatic lacerations on segments 4, 5, and 8. She subsequently had a miscarriage two days after surgery, which was managed medically.
The second patient with visceral organ injury was 27 years old, gravida 3, para 1, 18 weeks and one day pregnant, and was brought in after her car hit the center divider of a freeway at a speed of 70 mph and was then struck from the rear. She was a restrained front-seat passenger. The airbags were deployed. Free fluid was observed on abdominal ultrasound and CT. An exploratory laparotomy was performed 60 minutes after presentation, revealing 1500 mL of hemoperitoneum. A 5-cm fundal uterine laceration was noticed and repaired with hemostatic stitches. She eventually underwent emergency cesarean delivery for severe abdominal pain and suspected uterine rupture three months after the MVC. This case was reported in another article [11].
In addition to the two cases with visceral injury, we noted a patient with placental abruption after an MVC. She was 38 years old, gravida 2, para 1, 35 weeks and 6 days pregnant, and was brought in after a head-on car collision at a speed of 40 mph. She was a restrained driver. The airbags were not deployed. Severe hypertension was noted (maximum blood pressure 175/113), and she was admitted for preeclampsia with severe features. Six hours later, she developed heavy vaginal bleeding with recurrent late decelerations on continuous fetal heart monitoring. An emergency cesarean delivery was performed. During delivery, 10% of the placenta was found to have abrupted. It was unclear if the MVC, preeclampsia, or both caused the placental abruption.
There were no maternal deaths in this study. Since most patients had no or minor injuries, the median length of hospital stay was one day (IQR 1-2).
On univariate logistic regression, car speed was found to be significantly associated with intra-abdominal visceral organ injury (p = 0.0204). Car speed also independently predicted skin lacerations (p = 0.0001) and length of hospital stay (p < 0.0001), but not bony fractures (p = 0.1504). Car speed did not vary with gestational age or maternal age. However, there was a trend that pregnant individuals with parity of two or greater were involved in MVCs at lower car speeds (Figure 2). No associations or trends were observed for other factors, including gestational age and maternal age. Of note, we did not observe any differential preference for abdominal and pelvic imaging (CT scan or ultrasound) based on race/ethnicity after adjusting for car speed, gestational age, and maternal age (OR 1.667, 95% CI, 0.633-4.394, p = 0.3010).
Box plots showing the relationship between parity and car speed in pregnant individuals involved in motor vehicle collisions
Discussion
Our retrospective cohort study provides additional information on patient and collision characteristics of MVCs involving pregnant individuals at a high-volume level I trauma center. In our study cohort, most pregnant patients were in their mid-20s and in the second or early third trimester. The racial distribution in our study cohort was comparable with that of the county population [12]. Our patients had very high self-reported seat belt use - up to 99% - which was much higher than the 73% reported by another academic institution in the proximal neighborhood [7]. Airbags were also deployed more frequently in our study cohort (66% vs. 6%) [7]. The differences in airbag deployment could be explained by the direction of force in the crash, car speed, car model, recall bias, and other factors. Due to insufficient data in both studies, direct comparison was not feasible. Our study also noted no or minor injuries in the majority of patients. Only 15% of patients had skin lacerations, open wounds, or bony fractures. Intra-abdominal visceral organ injury, placental abruption, immediate baby delivery, and fetal demise were uncommon (N = 3, 2%).
The study attempted to explore predictive factors for intra-abdominal visceral organ injury but found this difficult due to the low number of cases in the study cohort. We observed that intra-abdominal visceral organ injury was more likely with high car speeds (p = 0.0204, univariate logistic regression). This finding was consistent with another Japanese national study, which showed increasing odds ratios for moderate to severe injuries with higher car speeds (21-40 km/h: OR, 3.03; 41-60 km/h: OR, 13.47; ≥61 km/h: OR, 44.56) [13].
In the field of impact mechanics, a parameter termed delta V - the change in speed that a vehicle undergoes as a consequence of crashing - is widely used as an indicator of crash severity [14,15]. Klinich et al. analyzed crashes involving 57 pregnant occupants and found that higher crash severity, more severe maternal injury, and lack of proper seatbelt use were associated with an increased risk of adverse fetal outcomes [16]. Tanaka et al. recently developed a computer model of a pregnant occupant using a mathematical approach known as the finite element method to quantify the predicted area of placental abruption at different collision velocities [17].
It was reported that for simulations of unrestrained pregnant drivers, doubling the collision velocity increased the area of placental abruption tenfold. They also found that when the placenta was located at the uterine fundus, simulated steering wheel contact to the abdomen 30 mm above the umbilicus led to a smaller placental abruption area than contact at or 30 mm below the umbilicus. However, the authors noted that for simulations involving the higher contact location 30 mm above the umbilicus, deformations of the maternal abdominal organs may correspond to severe liver damage or rupture, possibly leading to fatal hemorrhage and fetal loss. Taken together, these findings support that lower collision speed and the use of properly positioned seatbelts are important to protect pregnant individuals and their fetuses in MVCs [16,17].
Controversies exist in the literature regarding airbag safety in maternal and fetal outcomes, especially because the distance between the gravid uterus and the airbag is usually less than 10 inches - the minimum distance recommended by the National Highway Traffic Safety Administration. A number of case reports were published in the 1990s about complications such as fetal skull and brain injuries and uterine rupture [18-21]. A state-level study in Washington concluded that there was no evidence of more adverse pregnancy outcomes with the deployment of airbags [22]. Our study also did not show any statistically significant increase in the risk of severe abdominal injury with airbag deployment, occupant seat position, or collision point on the car.
Many studies have investigated the modification in driving behaviors and habits during pregnancy. A study in North Carolina and a survey in France both found that pregnant individuals were at lower risk of being drivers in the last few weeks of gestation [23,24]. We did not notice this pattern in our study cohort, probably because only two patients presented at term pregnancy. However, we observed that the car speed involved in MVC was associated with parity, especially with two or more prior livebirths. This might reflect the experience of people driving more safely after having children [25]. Further research is needed to elaborate on driving habits and behavioral modification during pregnancy and the peripartum period.
The strength of this study included a detailed chart review of 157 patients presenting in a busy level I trauma center in California. We included patient and collision characteristics that were not generally available in population-level datasets. This study, however, had several limitations. First, collision data were mostly self-reported, with some input from emergency medical services summoned to the scene. This type of data may be subject to recall bias. It is possible that pregnant occupants may avoid reporting violations against traffic law, such as speeding, lack of seat belt use, identity switch between drivers and passengers, or use of illicit drugs or alcohol. Second, we did not have information about seat belt types and car models. Differences in their features might impose differential mechanical impact on occupants, which could potentially lead to different extents of injuries. Third, 24 patients were excluded due to incomplete documentation or incomplete evaluation, which could lead to selection bias. These patients either left against medical advice or were asymptomatic after a minor MVC. Fourth, lack of follow-up after discharge might result in underestimation of maternal and fetal complications. Lastly, intra-abdominal visceral organ injury was uncommon, and, therefore, adjustment for confounding factors was impossible. Multi-center studies or a longer study period might be able to resolve this issue.
Conclusions
MVCs are the most life-threatening type of trauma in pregnancy. Our study showed a very high usage of seat belts in pregnant individuals, a low proportion of airbag deployment, and no or minor injuries in most accidents, with only 1% leading to severe intra-abdominal injury.
A higher car speed was associated with intra-abdominal visceral organ injury, skin lacerations, and longer hospital stay, but not with the deployment of airbags. The parity of a pregnant woman may modify her driving habits, including reduced car speed. We did not observe any differential preference for abdominal and pelvic imaging (ultrasound and CT) based on race/ethnicity, after adjustment for car speed, maternal age, and gestational age. More studies involving multiple centers, a longer study period, and behavioral psychology are needed to better understand the effects of MVC on pregnant individuals and to identify other potential risk factors for severe intra-abdominal injury.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Traumatic injuries to the pregnant patient: a critical literature review Eur J Trauma Emerg Surg Petrone P Jiménez-Morillas P Axelrad A Marini CP 3833924520192891687510.1007/s 00068-017-0839-x · doi ↗ · pubmed ↗
- 2Trauma in pregnancy: an updated systematic review Am J Obstet Gynecol Mendez-Figueroa H Dahlke JD Vrees RA Rouse DJ 11020920132333354110.1016/j.ajog.2013.01.021 · doi ↗ · pubmed ↗
- 3Trauma and pregnancy Am J Perinatol Connolly AM Katz VL Bash KL Mc Mahon MJ Hansen WF 331336141997921795310.1055/s-2007-994155 · doi ↗ · pubmed ↗
- 4Adverse pregnancy outcomes following motor vehicle crashes Am J Prev Med Vladutiu CJ Marshall SW Poole C Casteel C Menard MK Weiss HB 6296364520132413977710.1016/j.amepre.2013.06.018PMC 3859429 · doi ↗ · pubmed ↗
- 5Maternal trauma due to motor vehicle crashes and pregnancy outcomes: a systematic review and meta-analysis BMJ Open Amezcua-Prieto C Ross J Rogozińska E 010202010.1136/bmjopen-2019-035562 PMC 753745033020077 · doi ↗ · pubmed ↗
- 6The epidemiology of pregnancy-associated emergency department injury visits and their impact on birth outcomes Accid Anal Prev Weiss HB Sauber-Schatz EK Cook LJ 108810954020081846037710.1016/j.aap.2007.11.011 · doi ↗ · pubmed ↗
- 7Motor vehicle crashes in pregnancy: maternal and fetal outcomes J Trauma Acute Care Surg Owattanapanich N Lewis MR Benjamin ER Wong MD Demetriades D 8618659020213349655010.1097/TA.0000000000003093 · doi ↗ · pubmed ↗
- 8Effect of motor vehicle crashes on adverse fetal outcomes Obstet Gynecol Hyde LK Cook LJ Olson LM Weiss HB Dean JM 27928610220031290710010.1016/s 0029-7844(03)00518-0 · doi ↗ · pubmed ↗