Knowledge and Preventive Practices Regarding Diabetes Mellitus Among Non-Diabetic Adults in Kamrup Rural District of Assam: A Cross-Sectional Study
Darshana Hazarika, Imran Khan, Mangala Lahkar

TL;DR
This study examines the knowledge and preventive practices of diabetes among non-diabetic adults in rural Assam, finding a significant gap between knowledge and behavior.
Contribution
The study highlights the need for targeted health interventions to bridge the knowledge-practice gap in diabetes prevention.
Findings
52% of adults had adequate knowledge of diabetes, while 45% showed poor preventive practices.
A moderate, statistically significant correlation was found between knowledge and preventive practices.
Knowledge was significantly related to age, but no demographic factors influenced practices.
Abstract
Background: Diabetes mellitus (DM) is a chronic condition that is distinguished by abnormally elevated blood glucose levels. Aim and objective: The aim of this present study is to determine the knowledge and preventive practices regarding diabetes mellitus among non-diabetic adults in Kamrup Rural (R) District of Assam Methodology: Descriptive, cross-sectional design was adopted in the present study to evaluate knowledge and preventive practices regarding diabetes mellitus among non-diabetic adults. The data was collected using a structured questionnaire. Spearman’s correlation, Fisher’s exact test and Chi-square tests were employed for analyzing the data. Results: Of the adults surveyed, 52% demonstrated adequate knowledge of diabetes mellitus, 47% had moderately adequate knowledge, and only 1% had inadequate knowledge.. The preventive practices were found to be good in 55% of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
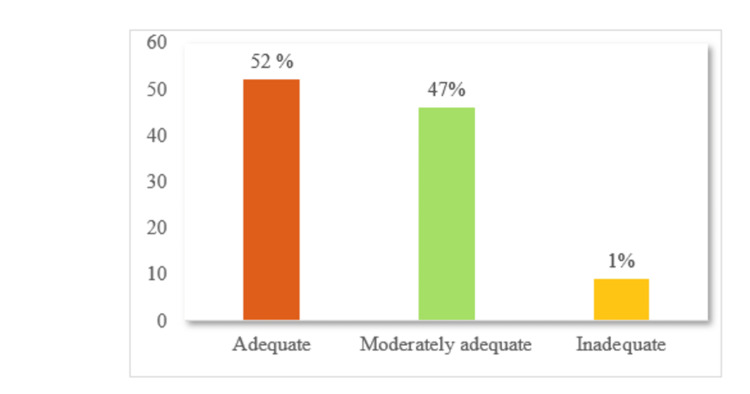 Figure 1
Figure 1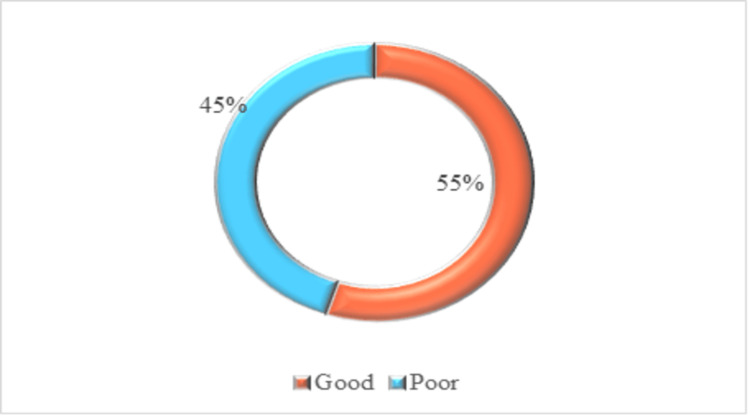 Figure 2
Figure 2| Demographic characteristics | Frequency (%) |
| Age | |
| 30-40 years | 82 (37) |
| 41-50 years | 98 (45) |
| 51-60 years | 40 (18) |
| Gender | |
| Male | 131 (60) |
| Female | 89 (40) |
| Marital status | |
| Married | 108 (49) |
| Unmarried | 98 (44) |
| Widow | 10 (5) |
| Divorced | 4 (2) |
| Educational qualification | |
| No formal education | 6 (3) |
| Primary school | 79 (36) |
| Middle school | 16 (7) |
| High school | 104 (47) |
| Higher secondary | 9 (4) |
| Graduation and above | 6 (3) |
| Family history of DM | |
| Yes | 167 (76) |
| No | 53 (24) |
| Food habit | |
| Vegetarian | 60 (27) |
| Nonvegetarian | 160 (73) |
| Attended training/programme on management of DM | |
| Yes | 58 (26) |
| No | 162 (74) |
| Items | Frequency (%) | |
| Yes | No | |
| Q1 DM is a condition of insufficient insulin production | 194 (88) | 26 (12) |
| Q2 Eating too much sugar can cause DM | 184 (84) | 36 (16) |
| Q3 DM is not curable | 125 (57) | 95 (43) |
| Q4 DM is hereditary | 115 (52) | 105 (48) |
| Q5 Sedentary lifestyle can lead to diabetes | 158 (72) | 62 (28) |
| Q6. Frequent urination is the symptoms of DM | 184 (84) | 36 (16) |
| Q7 Diabetic is manageable by diet & exercise | 196 (89) | 24 (11) |
| Q8 DM can be treated by medication | 114 (52) | 106 (48) |
| Q9 DM can be treated by insulin injection | 154 (70) | 66 (30) |
| Q10 DM effect many body parts | 198 (91) | 22 (10) |
| Q11 DM increase the risk of other disease | 121 (55) | 99 (45) |
| Q12 DM reduces life expectancy | 157 (71) | 63 (27) |
| Items | Frequency (%) | |
| Yes | No | |
| 1. Do you try to avoid fatty foods? | 194 (88) | 26 (12) |
| 2. Do you try to maintain a healthy body weight? | 184 (84) | 36 (16) |
| 3. Do you perform 30-60-minute physical exercise daily? | 124 (57) | 95 (43) |
| 4. Do you smoke? | 115 (52) | 105 (47) |
| 5. Do you check your blood sugar regularly (at least annually)? | 158 (72) | 62 (28) |
| 6.. Do you take food containing fibres, vegetables and fruits everyday | 196 (89) | 24 (11) |
| Knowledge score | Practice score | ||
| Knowledge score | Spearman’s rho | 1 | 0.496 |
| Sig (2-tailed) | - | 0.000 | |
| Practice score | Spearman’s rho | 0.496 | 1 |
| Sig (2-tailed) | 0.000 | - |
| Demographic characteristics | Adequate | Moderately adequate | Inadequate | Fisher’s exact | p-value |
| Age | 9.75 | 0.021* | |||
| 30-40 years | 53 | 29 | 0 | ||
| 41-50 years | 43 | 54 | 1 | ||
| 51-60 years | 19 | 20 | 1 | ||
| Gender | 4.14 | 0.972 | |||
| Male | 69 | 61 | 1 | ||
| Female | 46 | 42 | 1 | ||
| Marital status | 4.49 | 0.822 | |||
| Married | 58 | 49 | 1 | ||
| Unmarried | 48 | 49 | 1 | ||
| Widow | 7 | 3 | 0 | ||
| Divorced | 2 | 2 | 0 | ||
| Educational qualification | 8.66 | 0.731 | |||
| No formal education | 49 | 54 | 1 | ||
| Primary school | 45 | 33 | 1 | ||
| Middle school | 8 | 8 | 0 | ||
| High school | 3 | 3 | 0 | ||
| Higher secondary | 7 | 2 | 0 | ||
| Graduation and above | 3 | 3 | 0 | ||
| Family history of DM | 3.58 | 0.511 | |||
| Yes | 89 | 77 | 1 | ||
| No | 26 | 26 | 1 | ||
| Food habit | 0.428 | 0.937 | |||
| Vegetarian | 31 | 29 | 0 | ||
| Non vegetarian | 84 | 74 | 2 | ||
| Attended training/programme on management of diabetes mellitus | 8.87 | 0.066 | |||
| Yes | 29 | 39 | 1 | ||
| No | 86 | 64 | 1 |
| Demographic characteristics | Good | Poor | χ² | p-value |
| Age | 4.56 | 0.102 | ||
| 30-40 years | 38 | 44 | ||
| 41-50 years | 61 | 37 | ||
| 51-60 years | 22 | 18 | ||
| Gender | 0.826 | 0.662 | ||
| Male | 72 | 59 | ||
| Female | 49 | 40 | ||
| Marital status | 3.23 | 0.357 | ||
| Married | 60 | 48 | ||
| Unmarried | 55 | 43 | ||
| Widow | 3 | 7 | ||
| Divorced | 3 | 1 | ||
| Educational qualification | 5.95 | 0.311 | ||
| No formal education | 61 | 43 | ||
| Primary school | 45 | 34 | ||
| Middle school | 8 | 8 | ||
| High school | 2 | 4 | ||
| Higher secondary | 2 | 7 | ||
| Graduation and above | 3 | 3 | ||
| Family history of DM | 0.192 | 0.909 | ||
| Yes | 91 | 76 | ||
| No | 30 | 23 | ||
| Food habit | 0.370 | 0.543 | ||
| Vegetarian | 31 | 29 | ||
| Non vegetarian | 90 | 70 | ||
| Attended training/programme on management of diabetes mellitus | 0.825 | 0.662 | ||
| Yes | 38 | 31 | ||
| No | 83 | 68 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes, Cardiovascular Risks, and Lipoproteins · Diabetes Management and Education · Pharmacology and Nanomedicine Research
Introduction
The prevalence of non-communicable diseases (NCDs) has continued to be a global issue over the years. Regardless of their developmental stage, diabetes is one of the NCDs that are progressively presenting challenges to countries [1,2]. Diabetes mellitus (DM) is a chronic condition characterised by significantly elevated blood glucose levels. Type 2 diabetes mellitus (T2DM) and type 1 diabetes mellitus (T1DM) are the most common variants of diabetes. Hyperglycemia, insulin resistance, and relative insulin secretion deficit are the hallmarks of T2DM [3,4].
Since T2DM is the most widespread type of the disease, 90-95% of people with diabetes have it. Its association with morbidity and mortality, which has an impact on the person’s general health and well-being, makes it a serious public health concern. This disease is more common in younger age groups, affecting both adults and adolescents [5]. Due to the fast changes in way of living brought about by urbanisation, the risk factors for diabetes, hypertension and obesity have grown [6]. Approximately 537 million adults in the age group of 20-79 years around the world had diabetes in 2021 (global prevalence, 10.5%), which is anticipated to rise to 783 million (12.2%) by 2045 [7]. Among these, 45% were undiagnosed, with the greatest prevalence in low and middle-income countries [8]. Sedentary lifestyles, cigarette smoking, alcohol consumption, stressful situations, and a high-fat diet are also recognised as contributing factors to the development of Diabetes Mellitus.
Several individuals with DM are more susceptible to variety of short, as well as long term complications, which frequently result in permanent deaths [9]. Prolonged hyperglycaemia can lead to severe complications and organ dysfunction, specifically in the kidney, blood vessels, and eyes. Peripheral neuropathy, nephropathy, retinopathy, and autonomic neuropathy are significant long-term complications of diabetes [10]. According to a study done by Misra et al., a rapid surge in obesity across developing countries correlates with the rise in diabetes and cardiovascular issue-related deaths [11].
Assessment of an individual’s understanding of their illness has a beneficial effect on health education interventions. As a result, it is imperative to evaluate the knowledge and practices of persons with diabetes mellitus. Sufficient knowledge does not necessarily result in effective self-management practices or insufficient knowledge that leads to inadequate self-care practices [12,13]. Knowledge is the most formidable weapon in the fight against DM. Research proved that knowledge is a contributing factor for one to have a good attitude and proper practise to prevent DM [14].
A study carried out by Herath et al. revealed that most of the participants (77%) had moderate knowledge, while (39%) had above moderate knowledge regarding diabetes mellitus. The level of education demonstrated a significant and positive association with knowledge (p=0.001); however, the associations of gender and age with knowledge were statistically not significant. In terms of practices majority (80%) did not engage in regular exercise activities [15].
Research has shown that individuals who are knowledgeable regarding diabetes self-care achieve greater prolonged glycemic control. This awareness of glycemic control enables individuals to recognise risk factors that have been linked to diabetes and encourages them to pursue proper medical care, thus enabling the effective management of the disease. Emphasising knowledge and preventive strategies among non-diabetic adults is fundamental to public health initiatives aimed at combating diabetes. By providing adults with the appropriate information and resources before disease onset, we can avert significant human suffering, mitigate substantial economic burdens, and promote longer, healthier lives. Therefore, the study intended to evaluate the knowledge and preventive practice regarding diabetes mellitus among the adult who are not diabetic.
Materials and methods
Research design
A descriptive, cross-sectional design was adopted in the present study to evaluate knowledge and preventive practices regarding diabetes mellitus among non-diabetic adults
Ethical consideration
Ethical permission was obtained from the Institutional Ethics Committee (NGI/Ethics/PhD/2025/002) of the NEMCARE group of institutions, Mirza, Kamrup. The subjects were informed about the purpose and method used in the present study. Oral and written consent was taken from the subjects.
Study setting, sample size and sampling technique
Data were collected between July and August 2025. This study involved 220 non-diabetic adults who resided in the Sarpara and Kochpara villages of Kamrup, Rural district, Assam. The total number of eligible adults available in the selected two villages (Sarpara and Kochpara) during the data collection period was identified through local community records. Out of this population, 220 participants were selected based on their willingness to participate, accessibility, and suitability according to the inclusion-exclusion criteria.
Inclusion criteria
This study recruited participants who were non diabetic, willing to participate and who were in the age group between 30 and 60 years
Exclusion criteria
Unwilling participants, adults with diabetes mellitus, pregnant women and individuals with a history of mental illness, psychiatric issues or any serious health issues were excluded from this study.
Data collection methods and instruments used
Researchers developed a structured questionnaire organised in English and later translated into the local language (Assamese) to collect data from the participants. The questionnaire was divided into three sections. Section I consist of a total of seven questions regarding demographic characteristics of the samples; Section II includes 12 questions to evaluate the knowledge about diabetes mellitus; and Section III includes six questions to evaluate the practice on prevention of diabetes mellitus among non-diabetic adults. Each correct answer in the questionnaire carries 1 mark, and an incorrect answer is marked as 0 points. For the knowledge questions, scoring was categorised as 1-4 as inadequate knowledge, 5-8 as moderately adequate knowledge and 9-12 as adequate knowledge. Regarding practice questions, scoring was categorised as 0-3 as poor practice and 4-6 as good practice (Appendix A, B, C).
Validity and reliability
The questionnaire was distributed among seven experts for establishing content validity. Reliability of the baseline demographic proforma was calculated by intra ratter method (r=1). Reliability of the knowledge and practice questionnaire was determined using the split-half technique, and the 'r' value was determined using the Spearman formula (r=0.7 and 0.8, respectively).
Statistical analysis
The statistical analyses were performed using SPSS software (IBM Corp., 2011. IBM SPSS Statistics for Windows, Version 20.0). Descriptive statistics, including frequencies and percentages, were used to analyse demographic characteristics and levels of knowledge and preventive practices regarding diabetes mellitus. Spearman’s rank correlation coefficient was applied to assess the relationship between knowledge and preventive practices among non-diabetic adults. Fisher’s exact test and the Chi-square test were used to determine the association between knowledge and preventive practices and selected demographic characteristics.
Results
Table 1 presents that the majority of the 220 individuals in the study were middle-aged or older. Males made up a larger percentage, and about half of them were married, but a sizable portion were single. While most participants had only completed elementary or high school, a tiny percentage had higher education, indicating a variety of educational backgrounds among the participants. The majority of respondents were non-vegetarians, and the majority had a family history of diabetes. The percentage who had ever participated in any diabetes management course or program was quite small.
Table 2 indicates that most participants established good awareness of the basic aspects of diabetes. A large majority correctly identified diabetes as a condition of inadequate insulin production and recognised that excessive sugar intake can contribute to its development. Awareness of genetic risk, however, was comparatively lower, with only about half acknowledging this factor.
Figure 1 shows that just over half of the adults demonstrated adequate knowledge of diabetes mellitus, while nearly an equal proportion had moderately adequate knowledge. Only a very small fraction of participants exhibited inadequate knowledge, indicating generally favorable awareness levels in the study population.
Percentage distribution of knowledge regarding diabetes mellitus.
Table 3 indicates that most of the participants engaged themselves in several recommended preventive practices for diabetes. A large percentage stated that they avoid fatty foods, try to maintain a healthy weight and regularly consume fibre-rich foods, vegetables and fruits. More than half reported checking their blood sugar at least annually, although fewer participants engaged in daily physical exercise.
Figure 2 shows that slightly more than half of the adults demonstrated good preventive practices toward diabetes mellitus, while the remaining participants exhibited poor practice levels, indicating scope for improvement in overall health-promoting behaviours.
Percentage distribution of practice regarding prevention of diabetes mellitus.
Table 4 demonstrates a moderate, statistically significant correlation between knowledge and preventive practice regarding diabetes mellitus (Spearman’s ρ=0.496, p< 0.001). This suggests that individuals with higher knowledge about diabetes tend to engage in better preventive practices.
Table 4: Correlation between knowledge and preventive practice regarding diabetes mellitus among non-diabetic adults.Significant at p< 0.001.
Table 5 shows the association between participants’ knowledge regarding diabetes mellitus and their demographic characteristics. The analysis exposed a significant association between age and knowledge level (p=0.021), indicating that knowledge varied meaningfully across different age groups. Participants in the younger and middle-aged categories appeared more likely to have adequate knowledge compared to older adults.
*Table 5: Association between knowledge regarding diabetes mellitus with their selected demographic characteristics.Indicates significant at p< 0.05
No significant associations were found for gender, marital status, educational qualification, family history of diabetes, food habits, or attendance in diabetes-related training programmes (p> 0.05). These findings suggest that, except for age, the other demographic factors did not have a measurable influence on participants’ knowledge levels regarding diabetes mellitus.
Table 6 presents the association between participants’ preventive practices for diabetes mellitus and their demographic characteristics. The results show that none of the demographic variables, including age, gender, marital status, educational qualification, family history of diabetes, food habit or attendance in diabetes-related training, were significantly associated with preventive practice levels (p> 0.05).
Table 6: Association between preventive practice regarding diabetes mellitus with their selected demographic characteristics.Significant at p< 0.05.
These findings indicate that preventive behaviors related to diabetes were comparable across all demographic groups, suggesting that factors such as age, education, and lifestyle habits did not significantly influence engagement in good or poor preventive practices.
Discussion
These findings of the current investigation indicate that 115 (52%) of the adults had adequate, 103 (47%) had moderately adequate, and 2 (1%) had inadequate knowledge regarding diabetes mellitus. This finding is comparable with the study reported by Baig M et al wherein 66.86% of non-diabetic adults had a good knowledge and 33.14% had poor knowledge regarding diabetes mellitus [16]. Results of the investigation are also comparable with the research carried out by Dinesh et al., in which only 24% of the participants had good knowledge regarding diabetes [17].
The present study showed that out of 220 participants (88%), respondents actively try to avoid fatty foods. 184 (84%) reported that they try to maintain a healthy weight. 124 (57%) of respondents perform 30-60 minutes of physical exercise daily. Notably, 115 (52%) reported that they do not smoke. Most participants (158, 72%) do not check their blood sugar regularly (at least annually). The majority (196, 89%) of participants consumed fibre-rich foods, vegetables and fruits daily. These findings were consistent with the research study done by Baig M et al, in which 459 individuals (38%) consumed oily foods less frequently, while only 338 individuals (28%) and 153 individuals (12.7%) engaged in physical activities for 30-60 minutes per day on a frequent or very frequent basis, respectively. The majority of participants, 890 (73.7%), were tobacco smokers and received their blood pressure checks frequently (704, 58.3%).
Additionally, these findings are comparable to those reported by Alsous et al., in which only 62.3% of participants engaged in regular physical exercise. More than half of the participants had not undergone blood glucose testing in the preceding year, and approximately 45.3% reported consuming refined sugar [18].
In the present study, among the 220 non-diabetic adults, 121 (55%) demonstrated good preventive practices, while 99 (45%) exhibited poor practices regarding diabetes mellitus prevention. These findings contrast with those reported by Wolde W. et al., in which 64.6% of participants had poor practices, and only 35.4% had good practices related to diabetes prevention [19]. The current study demonstrates a moderate positive and statistically significant correlation between knowledge and preventive practice regarding diabetes mellitus (Spearman’s ρ=0.496, p< 0.001).
The result of this study is comparable with the findings reported by Vrinda et al., where a weak but significant positive correlation was found between knowledge and practice (r=0.349) [20]. The current study shows the association between participants’ knowledge regarding diabetes mellitus and their demographic characteristics. The analysis exposed a significant association between age and knowledge level (p=0.021). This study’s outcome contrasts with the findings reported by Herath et al., who observed that diabetes knowledge was not significantly associated with age or gender but showed a significant association with educational level (p=0.001) [15].
Limitations
This study’s limitations is its reliance on a purposive sampling method to select 220 participants from only two villages in the Kamrup (R) district of Assam. This substantially restricts the applicability of the findings to the general populace of adults.
Conclusions
The presentation showed that a majority of adults exhibited sufficient knowledge about diabetes mellitus, but a substantial proportion of adults failed to practice preventive strategies effectively. Despite differences in preventive knowledge among different age groups, no variation in preventive practices was found among different demographic groups. A discrepancy between knowledge and practice stipulates the need for strategies that enhance not only awareness but also sustainable lifestyle changes. Overall, the findings emphasise the importance of community-focused interventions that strengthen both understanding and preventive actions to reduce the future burden of diabetes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Increasing prevalence of diabetes mellitus in a developing country and its related factors P Lo S One Animaw W Seyoum Y 012201710.1371/journal.pone.0187670 PMC 567540229112962 · doi ↗ · pubmed ↗
- 2Knowledge, attitude and practice toward diabetes among the public in the Kingdom of Saudi Arabia: a cross-sectional study Front Public Health Al-Wagdi BE Al-Hanawi MK 13266751220243869498210.3389/fpubh.2024.1326675 PMC 11061416 · doi ↗ · pubmed ↗
- 3Knowledge, attitude, practice and associated factors among patients with type 2 diabetes in Cotonou, Southern Benin BMC Public Health AlaofèH Hounkpatin WA Djrolo F Ehiri J Rosales C 3392120213357924310.1186/s 12889-021-10289-8PMC 7881446 · doi ↗ · pubmed ↗
- 4Knowledge, attitude, and practice toward diabetes mellitus and their association with socioeconomic status among patients with type 2 diabetes mellitus in Saudi Arabia Cureus Almousa AY Hakami OA Qutob RA 015202310.7759/cureus.39641 PMC 1030625537388615 · doi ↗ · pubmed ↗
- 5Knowledge, attitudes, and quality of life of type 2 diabetes patients in Riyadh, Saudi Arabia J Pharm Bioallied Sci Al-Aboudi IS Hassali MA Shafie AA 195202820162741334710.4103/0975-7406.171683 PMC 4929958 · doi ↗ · pubmed ↗
- 6Knowledge on importance of yoga therapy among type II diabetic adults of Mirza, Kamrup (R), Assam: a descriptive study Imran Khan Hazarika D Khan I Lahkar M 142025 https://www.jneonatalsurg.com/index.php/jns/article/view/2604
- 7IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045 Diabetes Res Clin Pract Sun H Saeedi P Karuranga S 10911918320223487997710.1016/j.diabres.2021.109119 PMC 11057359 · doi ↗ · pubmed ↗
- 8IDF diabetes Atlas: Global estimates of undiagnosed diabetes in adults for 2021 Diabetes Res Clin Pract Ogurtsova K Guariguata L Barengo NC 10911818320223488318910.1016/j.diabres.2021.109118 · doi ↗ · pubmed ↗