Purulent Pericardial Abscess Caused by Escherichia coli in an Immunocompromised Patient Presenting With Mixed Septic and Cardiogenic Shock
António L Pessoa, Ana Teixeira Reis, Ana Santos Costa, Miguel Rodrigues, Carolina de Almeida Robalo

TL;DR
An immunocompromised patient developed a rare pericardial abscess caused by Escherichia coli, requiring urgent surgery and targeted treatment to survive.
Contribution
This case report highlights the importance of early imaging and surgical intervention in managing purulent pericarditis in immunocompromised patients.
Findings
A large pericardial abscess with air-fluid level was diagnosed in a 76-year-old woman with multiple myeloma.
Escherichia coli was identified as the causative agent through cultures of pericardial fluid, blood, and urine.
Targeted antimicrobial therapy and pericardiectomy improved the patient's condition after a complicated clinical course.
Abstract
Purulent pericarditis and pericardial abscess are rare yet life-threatening complications of bacterial infection, particularly among immunocompromised individuals. We report the case of a 76-year-old woman with multiple myeloma undergoing chemotherapy who presented with lumbar pain, fever, hypotension, and acute kidney injury. Imaging revealed a large pericardial abscess with a distinct air-fluid level. Despite broad-spectrum antibiotics, fluid resuscitation, and high-dose vasopressor therapy, she progressed to mixed septic and cardiogenic shock. Urgent pericardiectomy drained purulent material that later cultured Escherichia coli, consistent with blood and urine culture results. Her clinical course was complicated by mediastinitis but improved with targeted antimicrobial therapy. She was discharged after 38 days. This case highlights the diagnostic challenges and the critical role of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
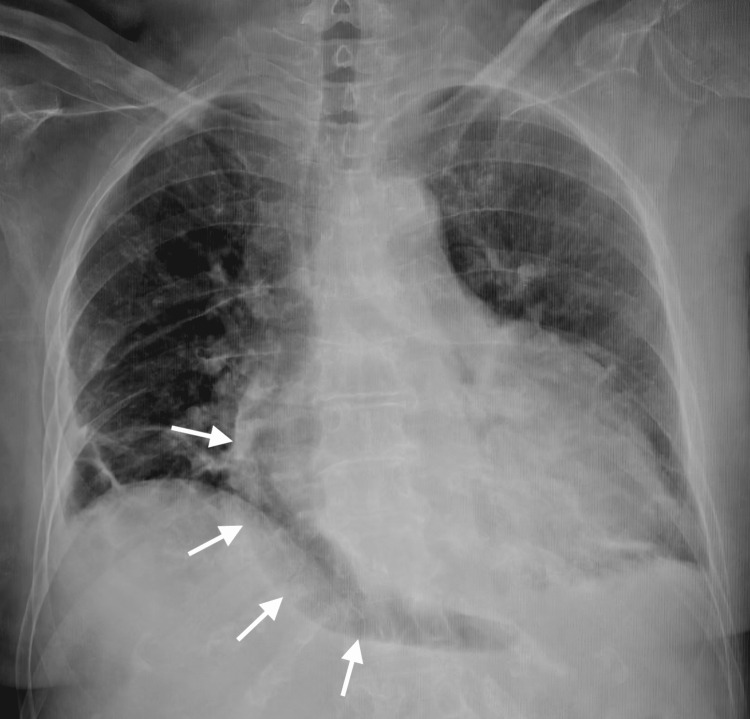 Figure 1
Figure 1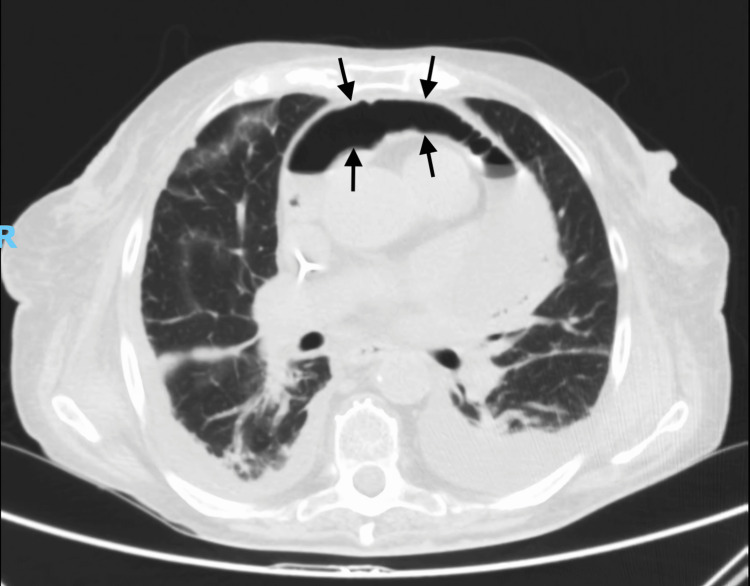 Figure 2
Figure 2 Figure 3
Figure 3| Parameters | Result | Reference range |
| Hemoglobin | 8.9 g/dL | 11.5-15 g/dL |
| Hematocrit | 26.5 % | 36-46 % |
| Leukocytes | 3800 μL | 4500-11400 μL |
| Neutrophils | 90.8 % | 41-75 % |
| Lymphocytes | 4.7 % | 20-48 % |
| Platelets | 73000 μL | 150000-350000 μL |
| BUN | 132 mg/dL | 21-43 mg/dL |
| Creatinine | 2.37 mg/dL | 0.6-1.1 mg/dL |
| Troponin I | 346.3 pg/mL | 13.8-17.5 pg/mL |
| C-reactive protein | 26.16 mg/dL | < 0.5 mg/dL |
| pH | 7.274 | 7.35-7.45 |
| HCO₃⁻ | 10.3 mEq/L | 22-26 mEq/L |
| Lactate | 7.8 mmol/L | 0.5-2.0 mmol/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Pneumothorax, Barotrauma, Emphysema · Takotsubo Cardiomyopathy and Associated Phenomena
Introduction
Purulent pericarditis is an uncommon but severe form of pericardial disease, accounting for less than 1% of all cases in the antibiotic era [1,2]. It is most frequently caused by Gram-positive organisms, whereas Gram-negative pathogens such as *Escherichia coli *are rare but increasingly recognized in immunocompromised individuals or in the setting of bacteremia [3,4,5]. Clinical manifestations are often nonspecific, and delayed diagnosis carries a high risk of morbidity and mortality. Early imaging with CT and echocardiography plays a critical role in establishing an accurate diagnosis and guiding treatment [6,7].
Case presentation
A 76-year-old woman with IgG-λ multiple myeloma (Revised International Staging System Stage III (R-ISS III)), undergoing chemotherapy, presented with a 24-hour history of lumbar pain, fever, asthenia, and hypotension. Her medical history included chronic kidney disease (Kidney Disease: Improving Global Outcomes (KDIGO) G4), hypertension, paroxysmal atrial fibrillation, and anxiety-depressive disorder. Ten days earlier, she had been evaluated for fever and hypotension and started empirically on ciprofloxacin.
Upon arrival to the emergency department, she was somnolent but arousable, with blood pressure of 71/47 mmHg, mean arterial pressure (MAP) 55 mmHg, heart rate of 96 bpm, respiratory rate of 25 breaths/min, temperature of 35.4°C, and oxygen saturation of 96% on room air. Physical examination revealed muffled heart sounds, marked peripheral mottling, lower-limb edema, and anuria.
Laboratory tests showed leukopenia, thrombocytopenia, normocytic anemia, elevated inflammatory markers, metabolic acidosis, and hyperlactatemia (Table 1).
Chest X-ray revealed a globular enlargement of the cardiac silhouette, an indirect radiographic sign suggestive of pericardial effusion (Figure 1).
Anteroposterior (AP) chest radiograph. The image demonstrates a region of increased pericardial silhouette hypotransparency, an indirect radiographic sign suggestive of pericardial effusion.
CT imaging revealed a large pericardial abscess with an air-fluid level (Figures 2, 3). Transthoracic echocardiography demonstrated heterogeneous pericardial collections suggestive of purulent content and impending constrictive physiology. Despite broad-spectrum antibiotics and vasopressor support, the patient progressed to mixed septic and cardiogenic shock.
Axial contrast-enhanced CT of the chest in a pulmonary window setting (lung window).The image shows a large pericardial abscess with a distinct air–fluid level, causing partial compression of adjacent cardiac structures.
Coronal reconstruction of a contrast-enhanced CT scan in a pulmonary (lung) window.The image demonstrates an extensive purulent pericardial collection enveloping the heart, with a clear air–fluid interface.
Given worsening hemodynamic instability, she underwent urgent pericardiectomy with drainage of copious purulent material. Cultures from pericardial fluid, blood, and urine yielded E. coli demonstrating resistance to ampicillin and trimethoprim-sulfamethoxazole and susceptibility to amoxicillin-clavulanate, cefuroxime, cefotaxime, and piperacillin-tazobactam, the latter of which was used for prolonged postoperative therapy due to mediastinitis. She recovered and was discharged after 38 days.
Discussion
Purulent pericarditis and pericardial abscess carry high mortality if not promptly diagnosed and treated. Although Gram-positive organisms remain the most common etiologies, Gram-negative pathogens are increasingly recognized in immunocompromised or bacteremic patients. Escherichia coli is an especially uncommon cause, with only scattered case reports-typically in patients with hematologic malignancies, postoperative thoracic infections, or urinary-tract-related bacteremia [4,5,8,9-12]. Our patient shared several classical risk factors, including advanced multiple myeloma, chemotherapy-induced immunosuppression, and urinary infection as the likely portal of entry.
Symptoms often mimic septic shock of non-cardiac origin, contributing to significant diagnostic delay. Several authors highlight that early manifestations are nonspecific and that cardiac involvement may remain unrecognized until imaging is performed [3,13,14]. CT is particularly valuable for identifying pericardial air-fluid levels, loculated collections, or mediastinal involvement, findings strongly suggestive of purulent infection, while echocardiography provides essential information regarding hemodynamic compromise and evolving constrictive physiology [7,8,14]. In our patient, the presence of a pericardial abscess with a well-demarcated air-fluid interface mirrors radiologic findings described in a minority of previously reported E. coli cases [9,11-13].
Definitive management requires directed antimicrobial therapy and drainage of the infected pericardial space. Although pericardiocentesis may be adequate for simple effusions, several retrospective series have demonstrated higher recurrence rates and inadequate source control with percutaneous drainage alone in cases of bacterial pericarditis [6,10,15]. Surgical drainage or pericardiectomy is preferred in cases involving loculated, thickened, or adherent pericardium, as seen in our patient. Early surgical intervention, combined with targeted antimicrobial therapy, led to successful recovery despite complications. This outcome aligns with recent reports indicating that timely and aggressive drainage remains the strongest predictor of survival in purulent pericarditis, particularly in immunocompromised hosts [9,10,14].
Conclusions
Pericardial abscess due to E. coli is exceedingly rare but should be considered in immunocompromised patients presenting with shock and sepsis. Early CT imaging, prompt antimicrobial therapy, and surgical drainage are critical for favorable outcomes. This case highlights the need for high clinical suspicion and early multidisciplinary management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1[Purulent pericarditis: a rare diagnosis]Rev Port Cardiol Ferreira dos Santos L Moreira D Ribeiro P 7217273220132401166710.1016/j.repc.2013.07.003 · doi ↗ · pubmed ↗
- 2Pericardial diseases Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine Lewinter MM Cremer CP Klein LA 16151634 Saunders 862005 https://www.clinicalkey.com/#!/content/book/3-s 2.0-B 9780323722193000864
- 3Clinical clues to the causes of large pericardial effusions Am J Med Sagristà-Sauleda J MercéJ Permanyer-Miralda G 9510110920001096714910.1016/s 0002-9343(00)00459-9 · doi ↗ · pubmed ↗
- 4A case of Escherichia coli purulent pericarditis Am J Crit Care Shiber JR Santana J 309312152006
- 5E. coli purulent pericarditis: case report and review Scand J Infect Dis Alrajhi AA Al-Barrak A Aldrete JS 227229342002
- 62015 ESC Guidelines for the diagnosis and management of pericardial diseases: the task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS)Eur Heart J Adler Y Charron P Imazio M 29212964362015 https://doi.org/10.1093/eurheartj/ehv 3182632011210.1093/eurheartj/ehv 318PMC 7539677 · doi ↗ · pubmed ↗
- 7Diagnosis and management of pericardial diseases Nat Rev Cardiol Imazio M Brucato A Trinchero R Adler Y 743751620091985906810.1038/nrcardio.2009.185 · doi ↗ · pubmed ↗
- 8Consecutive 1127 therapeutic echocardiographically guided pericardiocenteses: clinical profile, practice patterns, and outcomes spanning 21 years Mayo Clin Proc Tsang TS Enriquez-Sarano M Freeman WK 4294367720021200499210.4065/77.5.429 · doi ↗ · pubmed ↗