Severe Permanent Visual Decline After Hypotony-Induced Retinal Pigment Epithelial Changes
Konstantinos Benekos, Konstantina Gorgoli, Panagiotis Laspas, Panagiotis A Konstas, Andreas Katsanos

TL;DR
A rare case shows how short-term low eye pressure after surgery can lead to permanent vision loss due to retinal damage.
Contribution
This case report highlights a rare but severe complication of glaucoma surgery involving irreversible retinal pigment epithelium changes.
Findings
Short-term hypotony after glaucoma surgery can cause permanent subfoveal RPE changes.
Choroidal detachment and hypotony maculopathy may lead to irreversible visual loss.
Fundus autofluorescence is effective in detecting subtle RPE changes.
Abstract
Postoperative hypotony accompanied by choroidal effusions and maculopathy are well-recognized complications following glaucoma shunt surgery. We report a rare case of an elderly patient with irreversible visual loss in his left eye (OS) caused by retinal pigment epithelium (RPE) changes secondary to short-term hypotony maculopathy and choroidal detachment after a Paul glaucoma drainage device implantation. An 83-year-old man presented with recurrent episodes of transient loss of vision in his OS. Examination of his OS revealed high intraocular pressure (IOP), a one-piece in-the-bag posterior chamber intraocular lens (IOL) with pseudophacodonesis and hyphema, pointing toward the diagnosis of uveitis-glaucoma-hyphema (UGH) syndrome. Despite the urgent extraction of the IOL-capsular bag complex, pars plana vitrectomy, and implantation of a retro-pupillary iris-claw lens, the IOP was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
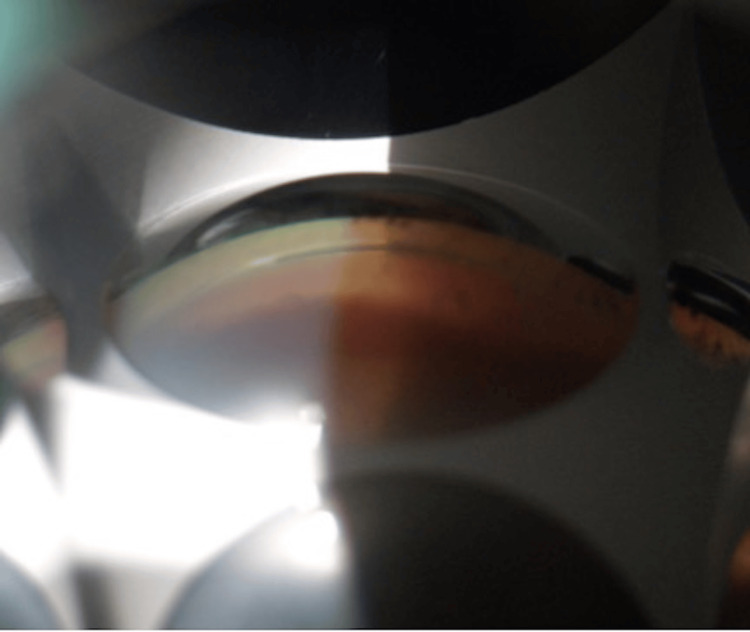 Figure 1
Figure 1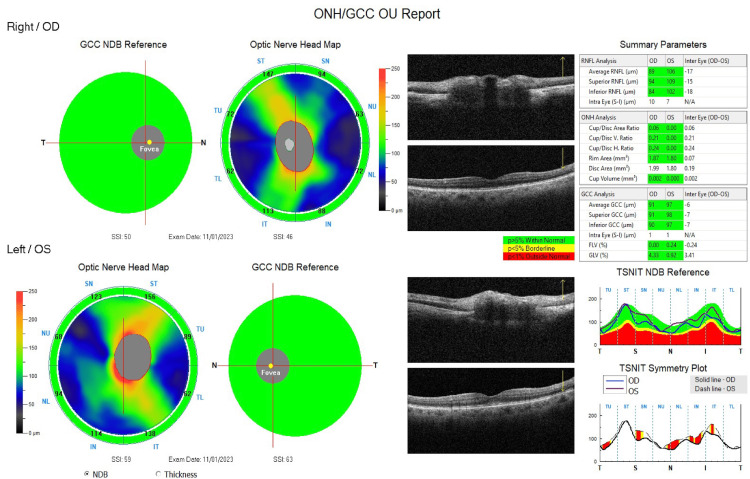 Figure 2
Figure 2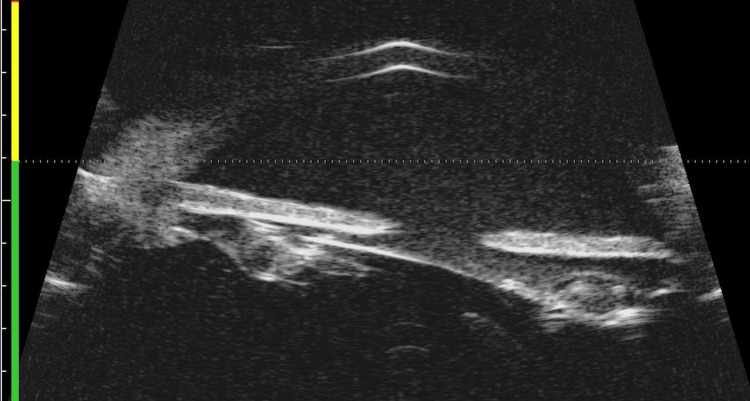 Figure 3
Figure 3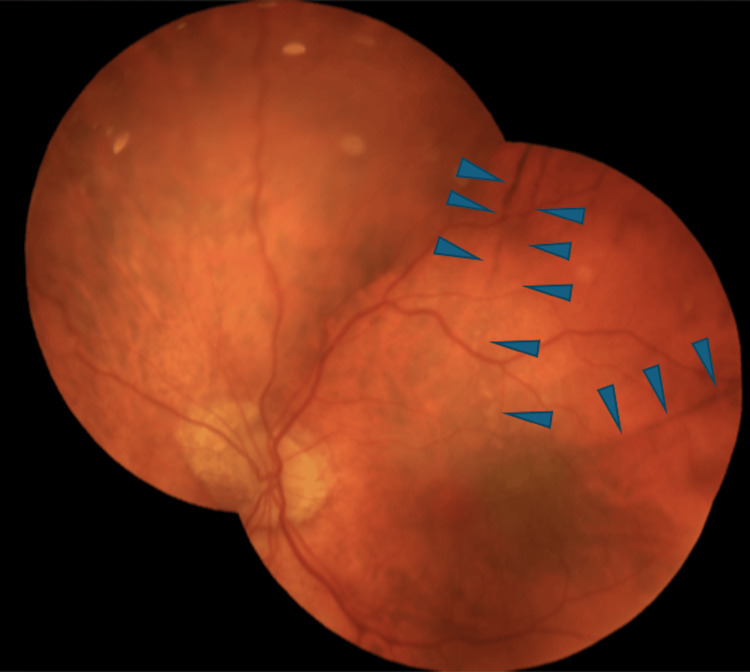 Figure 4
Figure 4 Figure 5
Figure 5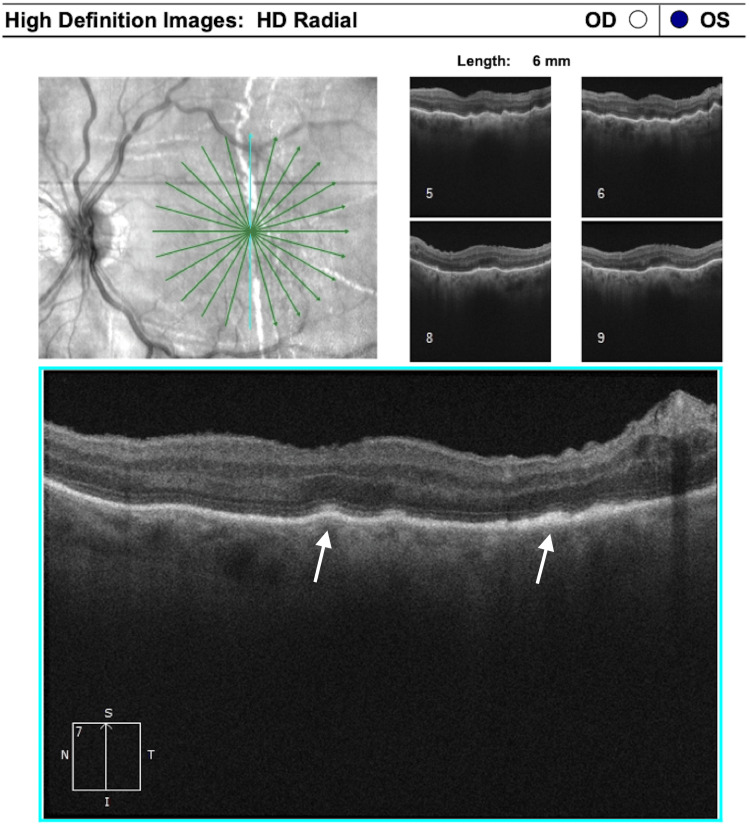 Figure 6
Figure 6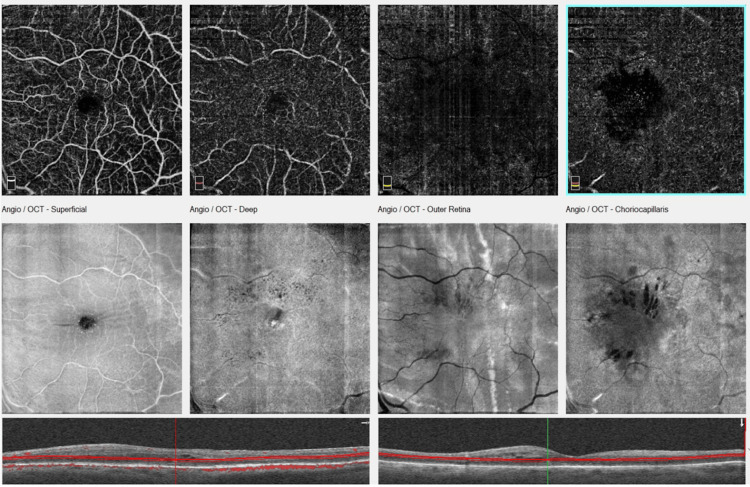 Figure 7
Figure 7| Time point | BCVA of the left eye (logMAR) | IOP of the left eye (mmHg) | Treatment |
| Initial presentation | 0.40 | 54 | Topical latanoprost and dorzolamide/timolol |
| One day before pars plana vitrectomy, and implantation of a retro-pupillary iris-claw lens | 0.40 | 38 | Topical latanoprost, dorzolamide/timolol, and dexamethasone, per os tab acetazolamide |
| One day after pars plana vitrectomy, and implantation of a retro-pupillary iris-claw lens | Hand movement | 26 | Topical latanoprost, dorzolamide/timolol, and dexamethasone, per os tab acetazolamide |
| One day before Paul implantation | 0.70 | 40 | Topical latanoprost, dorzolamide/timolol, per os tab acetazolamide |
| 1 day after Paul implantation | Hand movement | 2 | Topical atropine and dexamethasone |
| 7 days after Paul implantation/kissing choroidals observed | Hand movement | 7 | Topical atropine and dexamethasone |
| 17 days after Paul implantation/resolution phase | Counting fingers at 2 m | 12 | Topical atropine and dexamethasone |
| 28 days after Paul implantation/complete resolution of choroidals | Counting fingers at 2 m | 22 | Topical atropine and dexamethasone |
| 5 months after Paul implantation/permanent RPE changes | 1.00 | 14 | No treatment |
| 6 months after Paul implantation/cystoid macular edema | 1.00 | 12 | Topical nepafenac |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetinal and Macular Surgery · Glaucoma and retinal disorders · Intraocular Surgery and Lenses
Introduction
Glaucoma drainage implants are indicated when standard medical and surgical approaches, such as trabeculectomy, are likely to fail [1]. These devices reduce intraocular pressure (IOP) by draining the aqueous humor from the eye into an external reservoir. The valveless Paul glaucoma drainage device has been increasingly used in recent years for the management of elevated IOP in patients with refractory glaucoma [2]. Although glaucoma drainage implants constitute vital options in a number of patients, their use is sometimes plagued with serious complications [3].
Postoperative hypotony, often accompanied by choroidal effusions and maculopathy, is a well-recognized complication after plate-based shunt surgery, especially when non-valved implants, such as a Paul or Baerveldt device, are used. In plate-based shunt surgery, the reported rates of this complication range from 2% to 35.4% [2,4,5]. These complications are most commonly observed during the early postoperative period, before the implant endplate is adequately encapsulated [6]. Notably, the simultaneous occurrence of choroidal effusions and maculopathy has been reported to be rather uncommon, especially in the elderly [7]. While most cases with hypotony accompanied by choroidal effusions and maculopathy are self-limiting and resolve within a short period with conservative measures, long-lasting hypotony, particularly when accompanied by hypotony maculopathy, can lead to permanent central visual loss and irreversible RPE changes [8].
In this report, we present the case of a patient with permanent severe visual decline due to retinal pigment epithelium (RPE) changes as a consequence of hypotony-induced choroidal detachment and hypotony maculopathy following the implantation of a Paul drainage device. Remarkably, in our case, a relatively brief period of hypotony was sufficient to cause both choroidal effusions and hypotony maculopathy. This led to profound and apparently permanent RPE damage with severe visual loss.
Case presentation
An 83-year-old man presented in the ophthalmic emergency service with his third episode of recurrent transient blurred vision in the left eye (OS) within the past year. For the previous two episodes, he did not seek medical assistance. His past medical history involved systemic hypertension, dyslipidemia, and benign prostatic hyperplasia. His ophthalmic history included exfoliative syndrome and ocular hypertension treated with latanoprost once per day, along with a fixed combination of dorzolamide and timolol twice daily. His OS had uncomplicated phacoemulsification with posterior chamber intraocular lens (IOL) implantation in the capsular bag five years ago.
On clinical examination, distance best corrected visual acuity (BCVA) was logMAR 0.52 in the right eye (OD) and logMAR 0.40 in the OS, while the IOP was measured at 16 mmHg (OD) and 54 mmHg (OS). The slit-lamp examination in the OS revealed a one-piece in-the-bag posterior chamber IOL with pseudophacodonesis, exfoliative material on the pupillary border with absence of any iris neovascularization or transillumination, and hyphema < 1 mm, accompanied by scattered red blood cells in the anterior chamber (Figure 1). The examination in the OD was unremarkable, with the exception of nuclear and cortical cataracts. In fundoscopy, a small parafoveal choroidal nevus of the left fundus was observed, with no evidence of glaucomatous optic nerve damage in any eye (Figure 2). Ultrasound biomicroscopy in the OS detected anterior dislocation of the IOL-capsular bag complex with iris-IOL contact, likely secondary to the exfoliation syndrome (Figure 3), pointing toward the diagnosis of the uveitis-glaucoma-hyphema (UGH) syndrome. The patient’s treatment was escalated with the addition of acetazolamide 125 mg every eight hours per os and topical dexamethasone drops five times per day. Urgent extraction of the IOL-capsular bag complex, pars plana vitrectomy, and implantation of a retro-pupillary iris-claw lens were performed. On the day of the surgery, the preoperative IOP of the OS was 32 mmHg, while BCVA was stable at logMAR 0.40, and the IOL-capsular bag complex was still in place.
Hyphema observed in the inferior angle of the left eye
Optical coherence tomography of the retinal nerve fiber layer of both eyes within normal limits, without any glaucomatous damage
Ultrasound biomicroscopy of the left eye showing iris-intraocular lens contact
The surgery was completed without any intraoperative complications. On the first postoperative day, the IOP was 26 mmHg, and BCVA was hand movement. Despite the complete resolution of the signs of the UGH syndrome and BCVA of logMAR 0.7, 20 days after surgery, the IOP remained uncontrolled and increased to approximately 40 mmHg on maximal medical treatment. Therefore, the placement of a Paul drainage device was undertaken 10 days later.
One day before the tube shunt surgery, the clinical examination revealed no unknown abnormalities, and the IOP and BCVA of the OS were again 40 mmHg with maximum medical treatment and logMAR 0.7, respectively, with the iris-claw lens well placed behind the iris. The Paul implant was placed on the upper temporal quadrant between the superior and lateral rectus muscles, and one Vicryl 7.0 strangulation suture was placed around the tube so as to reduce the aqueous flow. No viscoelastic was placed in the anterior chamber during the operation, and a scleral patch was utilized to prevent conjunctival erosion. On the first postoperative day, the IOP was equal to 2 mmHg, with a deep anterior chamber along with Descemet membrane folds and corneal edema, while kissing choroidals were observed after seven days. The hypotony and choroidal effusions were treated conservatively with topical atropine instillation along with topical dexamethasone.
Even though the IOP increased to 22 mmHg and the choroidal detachment was resolved with intensive steroid and atropine administration in the following three weeks, the BCVA remained low (counting fingers at 2 m) 28 days after the drainage device placement. Fundoscopy revealed RPE changes extending beyond the macula toward the periphery and the optic nerve head, observed as dark and white lines (Figure 4). Importantly, autofluorescence clearly revealed the true extent of these hyperautofluorescent RPE lines radiating in a stellate pattern from the macula (Figure 5). High-definition optical coherence tomography demonstrated chorioretinal folds accompanied by RPE thickening at the areas corresponding to the RPE lines (Figure 6). Fluorescein angiography was not performed because the patient did not consent to intravenous fluorescein injection.
Fundus photograph of the left eye after choroidal detachment remission. Arrowheads point to the most prominent retinal pigment epithelium lines
Fundus autofluorescence of the left eye after choroidal detachment remission
Optical coherence tomography after choroidal detachment remission showing retinal pigment epithelium hypertrophy (arrows) and persistent choroidal folds (panels 5 and 6, top right)OD: right eye, OS: left eye.
These colored streaks appeared stable and did not change in size or shape over a six-month follow-up period. Visual acuity slightly increased to logMAR 1.0, and mild postoperative cystoid macular edema (CME) was observed in the six-month follow-up (Figure 7). The patient was prescribed topical nepafenac drops, and further follow-up was planned.
Optical coherence tomography (OCT) angiography and en face optical coherence tomography at six months of follow-up showing cystoid macular edema. Notice the appearance of the retinal pigment epithelium lines in the outer retina in en face optical coherence tomography imaging
Table 1 shows the clinical course of the patient.
Discussion
This is a case in which unusual RPE changes were identified after choroidal detachment and hypotony maculopathy following the implantation of a Paul glaucoma drainage device. While early postoperative hypotony is a well-recognized complication of non-valved glaucoma drainage implants [1], the appearance of long-lasting or permanent RPE alterations of this type after a short hypotony period is barely described in the literature. It is estimated that hypotony after a Paul drainage device implantation ranges from 2% [5] to 35.4% [4]. This wide range may reflect differences in the surgical techniques, including the use of 6.0 intraluminal suture or strangulation sutures, which both appear to offer some protection against hypotony. Although postoperative hypotony is usually transient and self-limiting [4,5,9], in our case, persistent changes in the RPE were observed, despite the quick recovery of the IOP to higher values.
In 1996, Schubert [10] defined postoperative hypotony as low pressure (of about 5 mmHg), whether acute, temporary, or permanent, eventually leading to functional and structural changes in the affected eye. Two of these structural changes are choroidal detachment [10] and hypotony maculopathy [11]. The latter is characterized by chorioretinal folds caused by the collapse of the scleral wall, resulting in the redundancy of the choroidal and retinal layers and their wrinkling [8]. These changes are usually noticed around the fovea in a linear, parallel pattern and are the underlying cause of the alternating dark and light streaks in the posterior pole. In cases of prolonged hypotony, these streaks usually become more prominent, as they are associated with changes in the structure of RPE [8].
It is noteworthy that choroidal effusions rarely occur simultaneously with hypotony maculopathy, especially in the elderly, in whom the sclera is more rigid and less prone to collapse, and thus, transscleral fluid outflow is expected to be reduced [7,12]. Interestingly, in such patients, the effusions could also play a protective role against the development of macular folds, as the suprachoroidal fluid that is accumulated helps maintain the scleral contour and counteract the sclera collapse during the hypotony period. However, this rare coexistence was indeed observed in our case, making it an exceptional finding.
Another noteworthy finding in the fundus of our patient is the unusual hypotony-related RPE changes that were observed just after the complete resolution of the kissing choroidal detachment. Their pattern, distribution, and thickness differ from what is usually observed, as the RPE changes extended radially beyond the macula, toward the temporal area, superiorly, and toward the optic nerve head without a uniform pattern. In addition, they were observed at the base and along the edges of the choroidal effusions, suggesting a topographical relationship between the area of detachment and the subsequent RPE remodeling. We postulate that the underlying mechanism is similar to that described in RPE changes caused by hypotony maculopathy. On the one hand, the mechanical stretching and the thinning of the RPE produce the light areas in the fundus, which appear as dark lines in the autofluorescence. On the contrary, the dark lines observed in fundoscopy correspond to the bright lines in autofluorescence and are probably the result of RPE thickening. As fundus autofluorescence can demonstrate the full extent of RPE lesions more clearly than color photography, it is a valuable tool when assessing cases with suspected RPE damage.
There is no exact definition of long-term, chronic, or persistent hypotony. In most studies, it is defined as IOP ≤ 5-6 mmHg sustained over three months or more [13,14], and as described above, hypotony of this duration can cause permanent RPE damage [8]. However, it seems that duration is not the only important factor. The magnitude of hypotony, even over a shorter than three-month period, may be sufficient to cause RPE lesions, as in our case.
As for the initial management, the definitive treatment of UGH syndrome includes IOL exchange, and in fact, the UGH represents one of the most common indications for IOL exchange [15]. In our case, the direct contact of the IOL-capsular bag complex with the iris led to UGH, which was likely secondary to zonular weakness associated with exfoliation syndrome. Although one might speculate that exchanging the lens for an iris-claw IOL, given its position close to the iris, could similarly provoke irritation, there is no robust evidence that iris-claw lenses should be avoided in UGH syndrome, as they are generally considered to be a safe option [16]. Despite the complete resolution of UGH-related signs after iris-claw IOL implantation, the IOP remained elevated and resistant to medical therapy, likely due to irreversible trabecular damage caused by high intraocular pressure and blood infiltration.
Last but not least, CME was observed in the affected eye of our patient in the last follow-up, six months after the drainage device implantation. It is well known that intraocular inflammation and surgery increase the risk of postoperative CME. This is particularly true in cases with capsular compromise, vitreous surgery, and/or iris tissue manipulation [17].
To the best of our knowledge, this case is perhaps the first of an adult patient in which this type of apparently permanent dark and light-colored hypotony-related RPE changes are described after a short period of hypotony complicated by choroidal effusion. In 2018, Osigian et al. [18] described similar hypotony-related RPE lesions in newborns, though without preceding choroidal detachments. In our case, the prior vitrectomy may have compromised the internal support of the vitreous body, thus allowing a greater mechanical stretch of the RPE at the edge of the choroidal detachment. Furthermore, this lack of internal support could also explain the simultaneous occurrence of both choroidal detachment and hypotony maculopathy, suggesting that a history of vitrectomy may be a risk factor for hypotony-related retinal complications. In such cases, early detection and management of hypotony might be beneficial, although this cannot be ascertained based on the currently available evidence.
Conclusions
This case highlights the fact that even transient episodes of ocular hypotony complicated by choroidal detachment and hypotony maculopathy can lead to irreversible RPE damage. The location of these RPE changes is inextricably intertwined with the area of the choroidal detachment. In the unfortunate event of such RPE alterations involving the area close to or underneath the macula, permanent visual handicap might occur. Therefore, clinicians should maintain a high level of clinical suspicion for such RPE changes in cases where the visual acuity cannot be fully restored after the resolution of the hypotony-related complications. Notably, even in the absence of clinically prominent lesions following the hypotony resolution, autofluorescence can be particularly useful for the assessment of these subtle but vision-threatening RPE changes. The early recognition of hypotony and the appropriate adjustment of aqueous flow after glaucoma surgery may be important in order to avoid permanent damage to the RPE. However, more similar cases are needed to corroborate our observations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Glaucoma drainage implants Int J Ophthalmol Agrawal P Bhardwaj P 131813281320203282168810.18240/ijo.2020.08.20PMC 7387917 · doi ↗ · pubmed ↗
- 2The Paul Glaucoma implant: a systematic review of safety, efficacy, and emerging applications Graefes Arch Clin Exp Ophthalmol CarlàMM Gambini G Boselli F 2447245926320254043472110.1007/s 00417-025-06861-2PMC 12513900 · doi ↗ · pubmed ↗
- 3A review on glaucoma drainage devices and its complications Cureus Gupta S Jeria S 014202210.7759/cureus.29072 PMC 955495336249639 · doi ↗ · pubmed ↗
- 4Three-year outcomes of the Paul glaucoma implant for treatment of glaucoma J Glaucoma Tan MC Ong CW Aquino MC 4784853320243850674910.1097/IJG.0000000000002369 PMC 11210944 · doi ↗ · pubmed ↗
- 5Surgical technique, perioperative management and early outcome data of the PAUL® glaucoma drainage device Eye (Lond) Vallabh NA Mason F Yu JT 190519103620223454520610.1038/s 41433-021-01737-1PMC 8450714 · doi ↗ · pubmed ↗
- 6Control and optimisation of fluid flow in glaucoma drainage device surgery Eye (Lond) Lim KS 2302343220182935069210.1038/eye.2017.316PMC 5811747 · doi ↗ · pubmed ↗
- 7Hypotony maculopathy: clinical presentation and therapeutic methods Ophthalmol Ther Thomas M Vajaranant TS Aref AA 7988420152625385410.1007/s 40123-015-0037-z PMC 4675727 · doi ↗ · pubmed ↗
- 8Hypotony maculopathy Acta Ophthalmol Scand Costa VP Arcieri ES 5865978520071754297810.1111/j.1600-0420.2007.00910.x · doi ↗ · pubmed ↗