CARE-DN: An Extension of the CARE Guidelines for Dry Needling Case Reports
Giorgos Tzigkounakis, Katerina Simati, Konstantinos Georgiadis, Vasileia Kostaridou, Paul Battersby, Sandra Calvo, Pablo Herrero, Adrian Kuzdzal, Johnson McEvoy, Zacarías Sánchez Milá, Jorge Velázquez Saornil, Michael Voight, Tianjun Wang, Manos Stefanakis

TL;DR
This paper introduces CARE-DN, a new reporting guideline for dry needling case reports to improve consistency and clarity in research.
Contribution
CARE-DN is the first consensus-based extension of the CARE guidelines tailored specifically for dry needling case reports.
Findings
16 DN-specific items were added to the CARE guidelines through a Delphi process with international experts.
The online CARE-DN tool received positive usability ratings for clarity and navigation.
CARE-DN aims to enhance the transparency and reproducibility of dry needling case reports.
Abstract
Background Dry needling (DN) is widely used in musculoskeletal and pain management, yet published DN case reports vary substantially in structure, terminology, and completeness, limiting reproducibility and interpretation. The objective of this study was to develop a consensus-based reporting guideline extension for DN case reports, as an extension of the CARE (CAse REport) guidelines. Methods A protocol was registered a priori on the Open Science Framework (OSF). A two-round modified electronic Delphi process was conducted with an international multidisciplinary panel of clinicians, researchers, and educators experienced in DN and acupuncture. Proposed DN-specific reporting items were generated through structured mapping of the CARE checklist and relevant literature. In Round 1, panellists rated item relevance and provided qualitative feedback. In Round 2, revised items were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
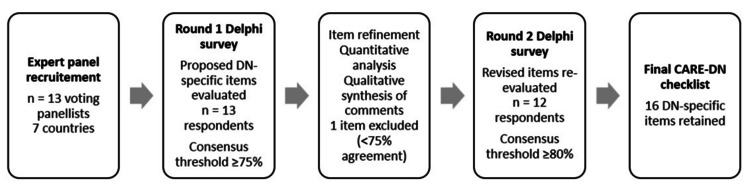 Figure 1
Figure 1| Characteristic | Value |
| Voting Delphi panellists | 13 |
| Countries represented | 7 |
| Highest academic qualification (all project contributors, n = 14) | PhD, 8 (57%) |
| PhD(c), 2 (14%) | |
| DPT, 1 (7%) | |
| MSc, 3 (21%) | |
| Academic appointment (university-based) | 8 (62%) |
| Clinical practice background | 13 (100%) |
| ≥10 years of experience with dry needling | 9 (69%) |
| 5-9 years of experience with dry needling | 3 (23%) |
| Does not practice dry needling, senior Traditional Chinese Medicine (TCM) acupuncture expert | 1 (8%) |
| Primary discipline: Physiotherapy | 11 |
| Primary discipline: Medicine | 1 |
| Primary discipline: Acupuncture/TCM | 1 |
| Non-clinical technical contributor (non-voting) | 1 |
| CARE domain | Scope of CARE-DN additions |
| Title | Explicit identification of the intervention as dry needling to improve specificity and indexing |
| Keywords | Inclusion of “dry needling” among keywords to enhance discoverability |
| Abstract | Clear specification of the dry needling intervention and, where relevant, the primary target or technique |
| Timeline | Reporting of the number of dry needling sessions delivered and the interval between sessions |
| Diagnostic assessment | Clinical rationale for selecting dry needling and reporting of imaging or objective assessments when used |
| Therapeutic intervention | Detailed description of targeted muscles or tissues, anatomical landmarks, needle specifications, number of needles, needling technique, depth and angle when relevant, imaging guidance if used, and duration of needle retention |
| Practitioner factors | Reporting of clinician profession, dry needling training or certification, and experience relevant to the intervention |
| Topic | Item | Checklist item description |
| Title | 1a | The diagnosis or intervention of primary focus followed by the words “case report.” |
| 1b | Include “dry needling” in the title | |
| Keywords | 2 | 2 to 5 key words that identify diagnoses or interventions in this case report, including "case report" |
| 2b | Include “dry needling” | |
| Abstract (no references) | 3a | Introduction: What is unique about this case and what does it add to the scientific literature? |
| 3b | Main symptoms and/or important clinical findings | |
| 3c | The main diagnoses, therapeutic interventions, and outcomes | |
| 3d | Conclusion - What is the main “take-away” lesson(s) from this case? | |
| 3e | Specify DN intervention clearly | |
| Introduction | 4 | One or two paragraphs summarising why this case is unique (may include references) |
| Patient Information | 5a | De-identified patient specific information |
| 5b | Primary concerns and symptoms of the patient | |
| 5c | Medical, family, and psycho-social history including relevant genetic information | |
| 5d | Relevant past interventions with outcomes | |
| Clinical Findings | 6 | Describe significant physical examination (PE) and important clinical findings |
| Timeline | 7a | Historical and current information from this episode of care organised as a timeline |
| 7b | Report the number of DN sessions delivered and the interval between sessions. If intervals changed during care, report what changed and why | |
| Diagnostic Assessment | 8a | Diagnostic testing (such as PE, laboratory testing, imaging, surveys) |
| 8b | Diagnostic challenges (such as access to testing, financial, or cultural) | |
| 8c | Diagnosis (including other diagnoses considered) | |
| 8d | Prognosis (such as staging in oncology) where applicable | |
| 8e | Rationale for DN: clinical reasoning behind selecting DN over other treatments | |
| 8g | Report any imaging or objective assessments used (if any) to guide diagnosis or dry needling (e.g. ultrasound, EMG, dynamometry) | |
| Therapeutic Intervention | 9a | Types of therapeutic intervention (such as pharmacologic, surgical, preventive, self-care) |
| 9b | Administration of therapeutic intervention (such as dosage, strength, duration) | |
| 9c | Changes in therapeutic intervention (with rationale) | |
| 9d | Report targeted muscles/tissues (name each muscle treated) | |
| 9e | Report anatomical landmarks used for localisation | |
| 9f | Report needle specifications (brand, material, gauge, length) | |
| 9g | Number of needles used | |
| 9h | Report depth and angle when relevant and include patient position and the approach path. Numeric depths are not required. | |
| 9i | Report the needling technique employed (e.g., static retention, pistoning, rotation) and the duration of active manipulation and, if recorded, number of bouts or frequency | |
| 9j | Report imaging guidance if used and include the modality, brand, model, and key settings | |
| 9k | Report whether a local twitch response was elicited (yes/no) and, if recorded, the approximate number and location | |
| 9l | Duration of needle retention | |
| 9m | Clinician credentials/experience | |
| Follow-Up and Outcomes | 10a | Clinician and patient-assessed outcomes (if available) |
| 10b | Important follow-up diagnostic and other test results | |
| 10c | Intervention adherence and tolerability (How was this assessed?) | |
| 10d | Adverse and unanticipated events | |
| Discussion | 11a | A scientific discussion of the strengths AND limitations associated with this case report |
| 11b | Discussion of the relevant medical literature with references | |
| 11c | The scientific rationale for any conclusions (including assessment of possible causes) | |
| 11d | The primary “take-away” lessons of this case report (without references) in a one-paragraph conclusion | |
| Patient Perspective | 12 | The patient should share their perspective in one to two paragraphs on the treatment(s) they received |
| Informed Consent | 13 | Did the patient give informed consent? Please provide if requested |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMyofascial pain diagnosis and treatment · Tendon Structure and Treatment · Shoulder Injury and Treatment
Introduction
Case reports contribute valuable clinical insights, particularly in fields where individualised assessment and manual procedures shape treatment outcomes. Dry needling (DN) is increasingly used in physiotherapy, sports medicine, pain rehabilitation, and musculoskeletal care. Despite growing research, there is no DN-specific guidance to standardise how interventions should be reported. This gap may result in variability in naming conventions, anatomical descriptors, needle specifications, procedural techniques, and documentation of responses. Such inconsistency affects clinical reproducibility and limits the integration of case findings into practice and research. A recent umbrella review further highlighted substantial heterogeneity in DN protocols across the literature and emphasised the need for greater standardisation to strengthen the clinical evidence base [1].
Reporting guidelines help promote completeness, transparency, and methodological rigour. The CARE (CAse REport) guidelines provide a widely adopted framework for clinical case reports across healthcare domains [2]. Extensions and adaptations to CARE have been developed for specific disciplines, including surgery [3], acupuncture [4], radiology [5], and COVID-19 [6], demonstrating the value of domain-focused specifications. To our knowledge, no reporting guideline has previously addressed DN, despite the intervention’s distinctive procedural, anatomical, and technical characteristics. Although DN shares the use of filiform needles with acupuncture, it is commonly delivered within an anatomically based biomedical framework and under different training and regulatory scopes, supporting the need for a dedicated reporting guideline.
CARE-DN was developed to fill this gap by identifying the minimum DN-specific information that should accompany a clinical case report. Our objective was to supplement the original CARE checklist with consensus-based DN-specific reporting items created through a rigorous Delphi process. The resulting checklist aims to support clinicians, authors, reviewers, and editors in improving the quality and reproducibility of DN case reports.
Materials and methods
Study design and registration
The CARE-DN project followed a predefined protocol registered on the Open Science Framework (OSF) [7] prior to data collection (the protocol is available at: https://doi.org/10.17605/OSF.IO/PT3RJ). The methodological approach was based on established principles for guideline development and Delphi methodology [8,9], and aligned with best practices for reporting Delphi studies [10]. The design, conduct, and reporting of this Delphi study align with the Guidance on Conducting and REporting of DElphi Studies (CREDES) [10].
A separate protocol article was not published, but all methodological steps, including Delphi materials, item refinement, consensus decisions, and amendments, were prospectively documented on OSF, which serves as the public protocol record. The accompanying Explanation and Elaboration document, which provides item-level rationale, clarifications, and illustrative examples, is provided as supplementary material (see Appendix, Supplementary File S1). Patients and members of the public were not involved in the design, conduct, reporting, or dissemination plans of this Delphi-based guideline development study, which focused on expert consensus and did not include patient data.
Overview of development process
The development of CARE-DN followed a predefined, multi-phase process aligned with established principles for reporting guideline development and modified Delphi methodology. The process consisted of four sequential stages: (1) project initiation and panel formation, (2) initial item generation, (3) Delphi consensus and refinement, and (4) usability evaluation and implementation considerations. The online CARE-DN tool was developed only after consensus was finalised and did not influence item generation or retention.
Project initiation and panel composition
An international multidisciplinary Delphi panel was assembled using purposive sampling. In total, 13 panellists from seven countries participated, including academic and clinical staff affiliated with seven universities, and representatives from professional associations and specialist practices. Of these, 12 panellists had established expertise in DN through advanced practice, teaching, and peer-reviewed publications. One senior academic with expertise in Traditional Chinese Medicine (TCM) acupuncture was intentionally included to broaden disciplinary representation and provide a complementary perspective on needle-based interventions. One panellist held dual qualifications in physiotherapy and TCM acupuncture, contributing integrative expertise spanning both biomedical and traditional East Asian medical paradigms. In addition, one non-clinical medical information systems auditor supported tool development and preliminary usability testing and was not involved in Delphi voting. Table 1 summarises the characteristics of the CARE-DN Delphi panel and project contributors.
Initial item generation
The initial pool of DN-specific items was generated by the core research team prior to the Delphi process through structured mapping of the CARE checklist against published DN case reports and relevant clinical and methodological literature. Existing reporting guidance for needling and complex non-pharmacological interventions, including the CARE-Acupuncture extension and TIDieR (Template for Intervention Description and Replication) principles, also informed item generation, with emphasis on domains not adequately covered by CARE. The development group reviewed the preliminary list to remove redundancy and improve clarity. No voting occurred at this stage. The resulting item set was submitted unchanged to Round 1 for independent panel evaluation.
Delphi consensus process
A two-round modified electronic Delphi process was implemented using anonymised online surveys. In Round 1, panellists rated each proposed DN-specific checklist item on a five-point scale of relevance and provided free-text comments. Responses were analysed quantitatively and qualitatively. Free-text comments were examined using a simple descriptive content approach, in which similar remarks were grouped into recurring themes and used to refine item wording, remove redundancies, and clarify examples for the next round. Consistent with the preregistered protocol, items with at least 75% of ratings at 4 or 5 were considered to have met the preliminary consensus threshold. These items were refined on the basis of comments and carried forward to Round 2, whereas the single item that did not reach this threshold was excluded. Feedback-informed wording adjustments, removal of redundancies, and greater use of direct, action-oriented phrasing were applied.
In Round 2, the revised items were re-evaluated using the same five-point relevance scale. Consensus for final inclusion was defined a priori as at least 80% of panellists rating an item 4 or 5. Descriptive statistics were calculated for each item, including means, standard deviations, and interquartile ranges. All 16 items reached the predefined Round 2 threshold and were therefore retained in the final CARE-DN checklist. Figure 1 summarises the process.
Flow diagram of the CARE-DN modified Delphi processAn international expert panel participated in a two-round electronic Delphi survey to evaluate proposed dry needling-specific reporting items for inclusion in the CARE-DN checklist.In Round 1, items meeting a predefined preliminary consensus threshold of ≥75% agreement (ratings 4-5) were retained and refined based on quantitative ratings and qualitative feedback, while one item was excluded.In Round 2, revised items were re-evaluated using a predefined consensus threshold of ≥80% agreement (ratings 4-5). All 16 items meeting this threshold were retained in the final CARE-DN checklist.
Usability evaluation
After the Delphi process, the usability of the online CARE-DN tool was assessed. Prior to structured testing, one medical doctor, one senior physiotherapist, and one IT specialist informally tested the tool and provided feedback on clarity, navigation, and workflow. Delphi panellists then used the online version of the tool for 10 days and completed a brief online questionnaire with five-point Likert items and optional free-text comments on usability, item clarity, navigation, and PDF export. The usability evaluation focused on online implementation and did not lead to changes in checklist content.
Ethical considerations
Participation in the CARE-DN Delphi was voluntary. All panellists provided electronic informed consent via an online enrolment and authorship form before the commencement of the study. No patients were involved, and no identifiable personal data were collected. Survey responses were analysed in aggregate and without individual attribution. Given the expert-only nature of the study and the absence of patient involvement, formal research ethics committee approval was not required.
Results
Consensus outcomes
In total, 12 of 13 panellists completed Round 2. All 16 DN-specific items achieved at least 80% agreement at ratings of 4 or 5. Items demonstrated strongly positive distributions, narrow interquartile ranges, and high mean relevance scores. Panel comments supported the final item set and highlighted the need for clarity, standardisation, and practical usability.
Informal preliminary testing of the online tool by a medical doctor, a senior physiotherapist, and an IT specialist in medical systems auditing suggested that both the checklist items and the online interface were clear in practice. In a separate structured usability evaluation focused on the online implementation, Delphi panellists completed a brief questionnaire after using the tool. Ratings addressed navigation, layout, and PDF export rather than the checklist content, and were consistently favourable, with respondents describing the tool as clear, concise, and quick to use, which supports its feasibility for routine academic and clinical use. Overall, these findings indicate that the tool operationalises CARE-DN by structuring checklist completion and generating an exportable checklist file suitable for journal submission.
Final CARE-DN items
The final CARE-DN checklist supplements the original CARE guideline by adding 16 DN-specific reporting items across the domains of Title, Keywords, Abstract, Timeline, Diagnostic Assessment, and Therapeutic Interventions. These items cover essential aspects of anatomical targeting, procedural description, needle characteristics, clinician expertise, and optional imaging guidance. Together, they strengthen the specificity and reproducibility of DN descriptions in clinical case reporting. Table 2 summarises the domains and scope of the DN-specific reporting elements added to the original CARE framework. Table 3 presents the full CARE-DN checklist in an integrated format, combining the original CARE items with the DN-specific extension items. An accompanying Explanation and Elaboration document is available as Supplementary File S1.
Summary of panel feedback
Panellists emphasised clear definitions, objective measures, and explicit reporting of adverse events. Adverse events remain covered under CARE item 10d, and no DN-specific adverse event items were added. One panellist proposed hygiene and sterile-field practices. These were not included as checklist items because CARE-DN is a reporting guideline, not a practice standard, so such details are treated as optional contextual information in the Explanation and Elaboration document. Suggestions to improve clarity through action-oriented wording were incorporated. Recommendations related to exemplars, dissemination, and implementation were noted for post-publication work. All quantitative ratings and qualitative comments from both Delphi rounds were archived on OSF.
Discussion
The CARE-DN extension represents the first consensus-based reporting guideline tailored specifically to DN case reports. Existing DN literature demonstrates wide variation in how key procedural elements are described, which limits reproducibility, comparability, and synthesis across studies. The final DN-specific items address domains repeatedly identified as clinically influential in the DN literature, including targeted anatomical structures, needling parameters, and manipulation techniques, as well as the clinician’s professional background and DN-specific training [11-13]. In this way, CARE-DN responds to an established gap by offering a structured, transparent, and clinically relevant framework for reporting DN interventions.
By building on the existing CARE framework, CARE-DN enhances reporting specificity for DN without modifying the foundational, well-accepted structure of CARE. As with other extensions, such as CARE-Acupuncture, the goal is to complement rather than replace the parent guideline. The emphasis on clarity, reproducibility, and procedural transparency aligns with recent recommendations for strengthening case report quality and supports more consistent clinical interpretation and future evidence synthesis [2].
Methodological rigour was strengthened through prospective registration, predefined consensus thresholds, and transparent reporting of participation. We obtained 12 of 13 responses (92%) in Round 2. Methodological guidance for Delphi surveys has long suggested ~70% per-round response as adequate for rigour [9], while published health-Delphi applications have regarded 61%-70% response rates as acceptable [14,15]. Current guidance emphasises the importance of transparently reporting participation and attrition to enable appraisal of methodological quality [10]. In this context, our 92% retention indicates excellent panel stability and engagement [10].
Consensus at the final round was defined a priori as ≥80% agreement (ratings 4-5). This approach follows the ACCORD (ACcurate COnsensus Reporting Document) guideline, which recommends pre-specifying and reporting consensus criteria [16]. In ACCORD’s Delphi process, consensus was ≥80% agreement among at least 20 respondents; although our panel was smaller, we adopted the same threshold and report participation and retention in full. This threshold is also consistent with recent field-specific precedent in the CARE-Acupuncture extension, which retained items at ≥80% agreement [4].
The international composition of the panel and the inclusion of clinicians, educators and researchers with substantial DN experience contribute to the external validity of the final checklist. At the same time, panel recommendations that extended beyond reporting, such as developing exemplars or providing implementation and dissemination tools, were recognised as important but were intentionally reserved for post-publication development. These components will be addressed in subsequent dissemination stages. Preliminary tool testing included review by an IT specialist in medical systems auditing, whose combined technical and usability input strengthened confidence in both the platform’s functionality and its practical applicability.
The inclusion of a usability evaluation distinguishes CARE-DN from many existing reporting guideline extensions and supports its implementation beyond publication, particularly through integration into an online, journal-ready reporting tool.
Limitations
Limitations include the modest sample size inherent to expert-based Delphi methodology and the predominantly English-speaking expertise represented. However, this panel size and composition are consistent with expert consensus development for reporting guideline extensions, and all elements required for transparent appraisal under CREDES were explicitly reported. Although we did not conduct a full pilot in published case reports or measure inter-rater reliability, preliminary clinician testing and a structured usability evaluation with the Delphi panel provide initial evidence of online tool usability, and highlight the need for future empirical assessment. Further research should evaluate the checklist’s usability and performance in real-world submissions and across different clinical and educational settings. In parallel, we plan targeted dissemination, translations, and implementation studies to support and monitor the adoption of CARE-DN in published DN case reports. Nonetheless, CARE-DN already provides a robust, consensus-based reporting structure that supports more transparent communication of DN case findings and strengthens the methodological foundation for future work in the field. As an initial implementation step, we have developed and tested a freely accessible online tool that hosts the CARE-DN and related CARE checklists and generates journal-ready PDF checklists, which may facilitate uptake by authors and editors.
Conclusions
CARE-DN provides a consensus-based extension of the CARE guidelines for accurate, transparent, and reproducible reporting of DN case reports. The checklist was developed through a structured Delphi process and reflects international expert agreement on essential DN-specific reporting elements. CARE-DN is intended to support authors, clinicians, educators, and journal editors in enhancing the clarity and interpretability of DN case literature. The checklist and Explanation and Elaboration document will be disseminated through professional networks and submitted for registration with the EQUATOR Network to promote widespread adoption.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical effectiveness of dry needling in patients with musculoskeletal pain - an umbrella review J Clin Med Chys M De Meulemeester K De Greef I 12051220233676985210.3390/jcm 12031205 PMC 9917679 · doi ↗ · pubmed ↗
- 2The CARE guidelines: consensus-based clinical case reporting guideline development Headache Gagnier JJ Kienle G Altman DG Moher D Sox H Riley D 154115475320132426633410.1111/head.12246 · doi ↗ · pubmed ↗
- 3The SCARE 2020 guideline: updating consensus Surgical C Ase R Eport (SCARE) guidelines Int J Surg Agha RA Franchi T Sohrabi C Mathew G Kerwan A 2262308420203318135810.1016/j.ijsu.2020.10.034 · doi ↗ · pubmed ↗
- 4CARE extension guideline for acupuncture case reports BMJ Evid Based Med Duan Y Xu Z Zhang Y 1136412025202510.1136/bmjebm-2025-11364140562435 · doi ↗ · pubmed ↗
- 5CARE-radiology statement explanation and elaboration: reporting guideline for radiological case reports BMJ Evid Based Med Wang M Luo X Xiao X 39940829202410.1136/bmjebm-2023-112695 PMC 1167204738458654 · doi ↗ · pubmed ↗
- 6Care for COVID- 19: a checklist for documentation of coronavirus disease 2019 case reports and case series Perm J Werthmann PG Riley D Kienle GS 12724202010.7812/TPP/20.127PMC 749786732956034 · doi ↗ · pubmed ↗
- 7CARE-DN: Development of a Consensus-Based Reporting Guideline for Dry Needling Case Reports Using a Modified e-Delphi Process Tzigkounakis G OSF 2025
- 8Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies J Clin Epidemiol Diamond IR Grant RC Feldman BM Pencharz PB Ling SC Moore AM Wales PW 4014096720142458129410.1016/j.jclinepi.2013.12.002 · doi ↗ · pubmed ↗