Impact of Primary Care Mental Health Management on Emergency Psychiatric Presentations: A Systematic Review
Anas E Ahmed, Rahf A Hakami, Atyaf M Alrajhi, Bayan A Buhulaigah, Laura M Damanhouri, Wejdan A Majrashi, Hanouf H Alhamyani, Lujain A Alamer, Asim H Alanazi, Fatimah H Fageehi

TL;DR
This paper reviews how managing mental health in primary care may reduce emergency psychiatric visits, but more research is needed to confirm effectiveness.
Contribution
The study systematically evaluates the impact of primary care mental health interventions on emergency psychiatric presentations across diverse populations.
Findings
Integrated primary care mental health interventions show trends toward fewer psychiatric emergency visits.
Higher-quality studies found moderate reductions in emergency use, while others showed mixed or modest effects.
Methodological limitations like confounding and selection bias limit strong conclusions.
Abstract
Primary care-based mental health management has been proposed as a strategy to reduce preventable psychiatric crises and lessen reliance on emergency departments, yet its impact remains uncertain across different populations and health systems. This review synthesized evidence from observational and quasi-experimental studies evaluating integrated, collaborative, or behavioral health home interventions within primary care and their association with emergency psychiatric utilization. Nine eligible studies were identified from a comprehensive search, most involving co-located or integrated behavioral health services aimed at improving continuity and outpatient engagement. Overall, interventions demonstrated consistent trends toward fewer psychiatric emergency visits, enhanced follow-up care, and better support for individuals with serious mental illness, although effect sizes varied and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
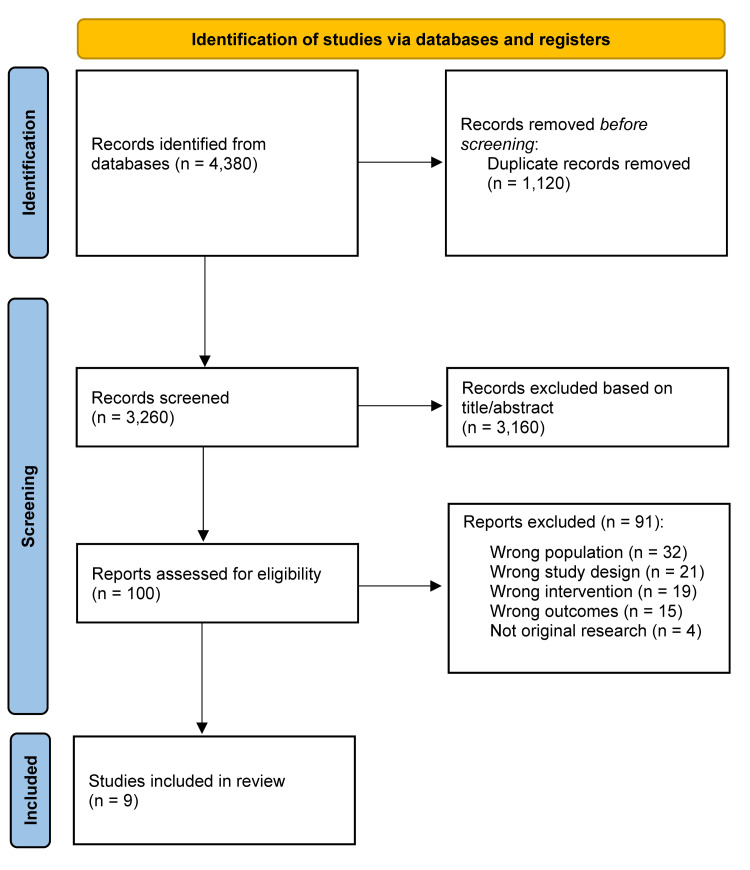 Figure 1
Figure 1| Study ID | Country/Setting | Study Design | Population | Intervention Type | Intervention Description | Comparator | Primary Outcomes | Effect on ED Utilization | Effect on Inpatient Use | Key Findings | Conclusion |
| Serrano et al. [ | USA - 4 primary care medical homes, Dane Co., WI | Retrospective quasi-experimental pre-post | Adults ≥18 with ≥1 primary care visit linked to mood/anxiety disorders; N=10,150. | PCBH | BHCs embedded in primary care; brief consults; shared EMR; 1-4 visits/year | One non-integrated clinic | Total ED visits; ED/PC ratio | Wingra clinic: ED/PC ratio ↓ −0.11; other clinics: trend improvement | Not assessed | High baseline ED rates; post-PCBH: leveling/downward trends | PCBH may reduce ED use in some clinics; effects vary by site |
| Waters et al. [ | USA - CMHC with Integrated Health Clinic | Retrospective pre-post | N=370 adults with SMI; ≥6 months pre/post enrollment | Integrated Primary Care within CMHC | Physical health services inside CMHC; co-located teams; separate EMRs | Pre-post | Physical health ED, inpatient admissions/days; ACS conditions | ED visits ↑ 0.073 → 0.603; OR 10.15 | Inpatient admissions/days ↑ | Very low chronic disease utilization; data gaps possible | CMHC integrated care did not reduce ED/inpatient use; trends increased; findings limited by low comorbidity capture |
| Breslau et al. [ | USA - 7 NYC CMHCs (PBHCI) | Quasi-experimental; DID with propensity score | Adults 18-64 with SMI; Wave 1: N=6,716 PBHCI, 13,039 controls; Wave 2: N=1,887 PBHCI, 11,542 controls | PBHCI | Primary care inside mental health clinics; chronic disease monitoring; wellness programs | Specialty mental health clinics without integration | (1) ED visits; (2) Frequent ED (≥4/yr); (3) Inpatient stays; (4) Frequent inpatient (≥3/yr) | Wave 1: Behavioral-health ED visits ↓ (OR=0.89); Wave 2: no effect | Medical inpatient stays ↑ (Wave1 OR=1.21; Wave2 OR=1.33) | Integration uncovered unmet medical needs; reduction in BH ED use only in Wave 1 | PBHCI increases medical admissions but modestly reduces BH ED visits; overall mixed effects |
| Krupski et al. [ | USA - 2 safety-net CMHCs, King Co., WA | Retrospective cohort study; DID with propensity score matching | Adults with SMI; Clinic1: N=373; Clinic2: N=389; matched controls | PBHCOn-site | The integrated primary care; nurse care managers; wellness programs; referrals | Matched non-integrated mental health patients | (1) ED visits/costs; (2) Inpatient admissions/costs; (3) Outpatient medical visits/costs | No significant difference | Clinic1: inpatient ↓18%→12%; Clinic2: no change | Outpatient utilization ↑: early integration sites may uncover unmet needs | Mature integration reduces inpatient admissions; ED use remains unchanged; integration is promising, but takes time |
| Adaji et al. [ | USA - Mayo Clinic ED; PCMH primary care system | Retrospective cohort (2 yrs) | Behavioral health ED patients; N=3,815; 5,398 ED visits; age 4-93 | PCMH | Integrated primary care with collocated IBH team, shared EHR, care coordination, and follow-up calls | Non-PCMH patients | (1) Hospital admission; (2) 72-hr ED revisit | Hospital admission reduced (OR=0.83, 95% CI 0.74-0.93); no effect on 72-hr returns | Less likely to be hospitalized | Strong integration may reduce admissions and improve continuity | PCMH reduces hospitalizations for BH ED patients; no effect on 72-hr revisits |
| Breslau et al. [ | USA - PBHCI clinics, 3 states | Multistate quasi-experimental; matched comparison | Adults with SMI and/or co-occurring substance use; >30 PBHCI clinics | PBHCI | Integration of primary care and preventive services; nurse management; chronic disease monitoring; team-based care | Matched non-PBHCI clinics | ED utilization, inpatient stays, Medicaid costs, and preventive care quality | Frequent ED use ↓ (mainly physical health) | Inpatient stays for physical health ↓; hospitalization costs ↓ | PBHCI increases outpatient care and preventive service use; variable chronic disease monitoring | PBHCI reduces ED/inpatient use for physical health, lowers costs; preventive care improvements are inconsistent |
| Chen et al. [ | USA - Urban medical center, Queens | Retrospective pre-post (2 yrs) | Older adults ≥50; N=920 intervention, N=341 comparison; low-income, racially diverse | Low-intensity integrated primary care + BH | 45-min integrated visit: psychiatric screening, lifestyle counseling, med review, referral support | Non-intervention patients | (1) ED use; (2) Cost per visit | ED visits decreased 5.66% → 3.01% of visit-days (p<0.001) | Not assessed | Cost per visit decreased; effect consistent across subgroups | Minimal BH integration within primary care reduces ED use and costs |
| Belson et al. [ | USA - UNC WakeBrook Primary Care, NC | Retrospective cohort | N=101 SMI adults with ≥1 ED visit; subset N=50 with chronic comorbidity | Enhanced PC Model for SMI (PCMH-based) | Co-located PCMH; broad primary care; behavioral counseling; peer support; chronic disease monitoring | Pre- and post- within the same patients | Annual ED visits/person | Physical-health ED visits ↓ (Years 3-4: 3.23→1.83; Rate Ratio=0.57) | Not assessed | High baseline ED; decline required ≥3 yrs stable care | Enhanced PC integrated with BH reduces ED use after long-term engagement |
| Bandara et al. [ | USA - Maryland Medicaid; BHH in PRPs | Longitudinal cohort; marginal structural modeling | N=12,232 adults with SMI; 3,319 BHH, 8,913 non-BHH | Behavioral Health Home (BHH) | Care management, physical health coordination, social support | PRP patients not enrolled in BHH | (1) All-cause ED; (2) Physical-health ED; (3) BH ED; (4) Inpatient admissions | All-cause ED probability ↓0.26→0.23; driven by physical-health ED ↓ | No effect on inpatient admissions | Longer BHH exposure strengthened ED reduction; BHH inpatients may need extra coordination. | BHH slightly reduces ED visits but not admissions; suggests improved physical health coordination |
| Study ID | Confounding | Selection Bias | Classification of Intervention | Deviations From Intended Intervention | Missing Data | Outcome Measurement | Selective Reporting | Overall ROBINS-I Risk |
| Serrano et al. [ | Serious - quasi-experimental design with partial adjustment | Moderate - clinic assignment | Low | Low | Moderate | Low | Moderate | Serious risk of bias |
| Waters et al. [ | Serious - high confounding; no control; self-selection | High | Low | Low | High - missing claims data | Moderate | High | Critical risk of bias |
| Breslau et al. [ | Serious - DID + propensity methods used, but waves differ; residual confounding remains | Moderate - clinic-level assignment | Low | Low | Moderate | Low | Moderate | Serious risk of bias |
| Krupski et al. [ | Moderate to Serious - DID + matching helps, but baseline SMI severity differences remain | Moderate | Low | Low | Moderate | Low | Low | Serious risk of bias |
| Adaji et al. [ | Serious - baseline imbalance; non-random PCMH membership; residual confounding | Moderate - PCMH membership self-selected | Low - PCMH classification clear | Low - no active deviations | Moderate - incomplete reporting of missingness | Low - objective EHR outcomes | Moderate - limited outcomes reported | Serious risk of bias |
| Breslau et al. [ | Moderate - large dataset and matched groups, yet confounding still likely | Moderate | Low | Low | Moderate | Low | Low | Moderate risk of bias |
| Chen et al. [ | Serious - no control group; pre-post only | Moderate - voluntary participation | Low | Low | Moderate | Low | Serious - outcomes limited to available billing data | Serious risk of bias |
| Belson et al. [ | Serious - no control; long pre-post design; multi-year lag | Moderate | Low | Low | Moderate-High | Low | Serious - no protocol and selective analyses | Serious risk of bias |
| Bandara et al. [ | Moderate - MSM weighting strong but residual confounding possible | Low-Moderate | Low | Low | Low-Moderate | Low | Low | Moderate risk of bias |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPsychiatric care and mental health services · Emergency and Acute Care Studies · Schizophrenia research and treatment
Introduction and background
Mental health-related emergency department (ED) visits have increased substantially worldwide. This trend places growing pressure on acute care systems. Individuals experiencing crises related to depression, anxiety, psychosis, substance use, or suicidal ideation often turn to the ED. Fragmented outpatient services and limited community mental health capacity contribute to this pattern [1-3]. The rising demand leads to ED overcrowding, prolonged wait times, psychiatric boarding, higher healthcare costs, and disrupted continuity of care [1-3]. Reducing preventable psychiatric ED presentations has become a priority for health systems and policymakers [1-3].
Primary care plays a critical role in the early detection and ongoing management of mental health conditions. It is the most accessible point of contact for many individuals with emerging or chronic symptoms [3-5]. However, traditional primary care models often face challenges. These include limited mental health expertise, insufficient collaboration with behavioral health specialists, and structural barriers that hinder proactive follow-up [3-5]. Such limitations can create gaps in care, increasing the likelihood of clinical deterioration and crisis-driven ED use [3-5]. Strengthening mental health capacity within primary care is a key strategy for improving outcomes and reducing unnecessary reliance on acute services [1-5].
Integrated primary care mental health models, including patient-centered medical homes (PCMHs), primary care behavioral health (PCBH) models, behavioral health homes, and various co-located or collaborative approaches, have gained traction as potential solutions [1-6]. These models commonly incorporate embedded mental health professionals, structured care coordination, shared electronic health records, routine screening, and systematic follow-up [1-6]. By enhancing continuity and supporting earlier intervention, integrated care aims to prevent escalation of symptoms that lead to ED presentations [1-6]. Emerging evidence suggests that such models may reduce psychiatric ED visits and improve psychosocial outcomes, although findings vary across settings and populations [1-9].
Despite growing interest in integration, the literature assessing its direct impact on psychiatric ED utilization remains fragmented and methodologically diverse. Studies differ in their definitions of integration, the populations they evaluate, and the outcomes they measure [1-9]. Some report meaningful reductions in ED use, while others find modest or inconsistent effects [1-9]. Individuals with serious mental illness represent a particularly high-risk population, yet research focused on this group remains limited and often susceptible to confounding [2,6,8,9]. These gaps highlight the need for a systematic synthesis of existing evidence [1-9].
This systematic review aims to evaluate the impact of primary care mental health management on reducing psychiatric ED presentations across diverse integration models and healthcare environments [1-9]. By clarifying the effectiveness of these interventions, the review seeks to inform policy, guide resource allocation, and support the development of more effective pathways that reduce crisis-driven utilization of ED services for individuals with mental health conditions [1-9].
Review
Methods
Literature Search Strategy
A systematic search was conducted in PubMed, the Cochrane Library, Web of Science, and Scopus to identify studies evaluating primary care mental health integration and its impact on ED psychiatric or behavioral health presentations. Searches covered all publication years through December 2025 and used combinations of subject headings and free-text terms related to primary care models, mental health conditions, emergency services, and healthcare utilization. Search strategies were adapted for each database. Only English-language human studies using observational or quasi-experimental designs were included.
Eligibility Criteria
Eligibility was defined using the Population-Exposure-Comparator-Outcome (PECO) framework [10]. Eligible studies examined adults or mixed-age populations with mental health conditions receiving services in primary care settings, or individuals with psychiatric or behavioral health-related ED presentations. Exposures included any model of integrated or enhanced primary care mental health-such as co-located behavioral health services, collaborative care, the PCMH model, the PCBH model, behavioral health homes, or similar interventions. Eligible studies used a comparator group or a pre-post design and reported at least one ED-related outcome, including total ED visits, psychiatric ED visits, frequent ED use, ED-to-primary care ratios, or psychiatric admissions. Exclusion criteria included pediatric-only studies, ED-based interventions lacking a primary care component, non-original research, case reports, editorials, non-English publications, conference abstracts, and studies without ED utilization outcomes.
Study Selection
All records were imported into a reference management system, and duplicates were removed. Two reviewers independently screened titles and abstracts, excluding studies that did not meet population, exposure, design, or outcome criteria. Full texts of potentially eligible studies were reviewed by both reviewers, with disagreements resolved through discussion or a third reviewer. The screening process followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and is summarized in the PRISMA flow diagram [11].
Data Extraction and Quality Appraisal
Two reviewers independently extracted study characteristics, including setting, design, sample demographics, type of integrated care model, comparator group, and ED-related outcomes such as total visits, psychiatric visits, and high-utilization patterns. Disagreements were resolved by consensus. Risk of bias was assessed using the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool across domains, including confounding, participant selection, intervention classification, deviations from intended interventions, missing data, outcome measurement, and selective reporting [12]. Most studies showed moderate to serious risk of bias due to observational designs, baseline imbalances, self-selection, and reliance on administrative datasets. These assessments informed the narrative synthesis.
Results
Study Selection
The search yielded 4,380 records from PubMed (n = 1,432), Scopus (n = 1,534), Web of Science (n = 884), and the Cochrane Library (n = 530). After removing duplicates, 3,260 records were screened, with 3,160 excluded due to irrelevance, lack of ED outcomes, non-psychiatric focus, or non-original study design. One hundred full texts were reviewed, and 91 were excluded for reasons including wrong population, wrong design, wrong intervention type, or absence of ED-related outcomes. Nine studies [1-9] met all inclusion criteria and were included for qualitative synthesis. None were suitable for meta-analysis due to substantial heterogeneity. The selection process is summarized in the PRISMA diagram (Figure 1).
PRISMA flow diagramPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Baseline Characteristics
The nine included studies represented diverse U.S. healthcare environments, including safety-net systems and community mental health centers [2-4], urban primary care clinics [7], tertiary hospital EDs [5], PCMHs [1,8], and statewide behavioral health home programs [9]. Most studies used retrospective or quasi-experimental designs, including pre-post comparisons, difference-in-differences analyses, and marginal structural models. Sample sizes ranged from small cohorts of approximately 100 adults with serious mental illness [8] to Medicaid datasets exceeding 12,000 individuals [9]. Populations commonly included adults with serious mental illness, multimorbidity, or high ED utilization (Table 1).
Integrated care models varied widely. Some studies evaluated comprehensive behavioral health integration within mental health settings using the Primary and Behavioral Health Care Integration (PBHCI) model [2-4,6], while others examined behavioral health integration within primary care via the PCMH framework [1,5,8] or the PCBH model using embedded behavioral health consultants [1]. Low-intensity models included screening and referral interventions [7], while enhanced primary care programs located on psychiatric campuses provided intensive chronic disease management [8]. Comparator groups included usual care clinics, non-integrated programs, or pre-intervention periods. Outcomes included ED visit frequency (psychiatric, behavioral, medical, or all-cause), return visits, high ED use, primary care engagement, inpatient admissions, and healthcare costs.
Quality Assessment
Risk of bias was generally serious due to limitations of observational designs. Confounding was the most common concern, as most studies lacked randomization and showed baseline imbalances or self-selection into integrated programs. Serious confounding was noted in Adaji et al. [5], Breslau et al. [3], Chen et al. [7], and Serrano et al. [1]. Selection bias was typically moderate because clinic assignment or participation was voluntary. Intervention classification and deviations from intended interventions were generally low risk (Table 2).
Missing data and selective reporting contributed to further concerns. Some studies lacked detailed reporting on missingness [5], while others relied on administrative datasets with limited variables [7,8]. Outcome measurement was generally reliable due to the use of electronic health records or claims data, but showed moderate concerns in Waters et al. [2] due to incomplete data linkage. Selective reporting was graded moderate to serious in studies lacking predefined protocols. Overall, most studies were judged at serious risk of bias, while Bandara et al. [9] and Breslau et al. [6] showed moderate overall risk.
Synthesis of Findings
Across the nine studies, the impact of primary care mental health integration on ED utilization varied widely, reflecting differences in program intensity, patient characteristics, and implementation quality. Three overarching patterns were observed.
First, the maturity and depth of integration strongly influenced outcomes. High-intensity, well-established models such as PCMH-based integrated care [5], PBHCI programs [4], and statewide health homes [9] generally reported reductions in psychiatric or all-cause ED visits. PBHCI programs showed early reductions in behavioral ED visits [3], and statewide health homes improved care coordination, reducing ED reliance [9]. In contrast, early-stage, low-intensity, or poorly implemented integration models showed limited or adverse effects. PCBH implementation reduced ED visits only in clinics with strong organizational readiness [1], while early-phase PBHCI programs increased ED and inpatient visits [2].
Second, patient complexity and unmet medical needs modified the impact of integrated care. In some settings, ED visits increased initially because integrated care uncovered unaddressed medical conditions. PBHCI models reported higher medical inpatient admissions across multiple waves [3], and the Enhanced Primary Care model showed delayed reductions in ED use following sustained engagement [8]. Similarly, Waters et al. [2] observed increased ED visits likely due to newly identified medical conditions. Conversely, integrated care was most effective for patients with complex multimorbidity. Chen et al. [7] and Bandara et al. [9] found greater reductions among individuals with multiple chronic medical conditions. These findings indicate that integrated care is particularly effective when programs are equipped to manage both physical and behavioral health needs.
Third, multiple mechanisms explained reductions in ED use in mature integrated programs. Improved continuity of care, supported by shared electronic records, alert systems, and structured follow-up, helped prevent crises and reduced psychiatric ED recidivism [5,6]. Enhanced access to medical and behavioral health services within the same clinic allowed earlier intervention and improved chronic disease management, contributing to reductions in physical ED visits [9]. Team-based care coordination enabled providers to jointly address medical, psychiatric, and psychosocial drivers of ED use, particularly in clinics with cohesive workflows [1]. Stabilizing high utilizers through consistent follow-up further reduced ED reliance [8]. When these mechanisms were weak or inconsistently implemented, ED use remained unchanged or increased, as seen in Waters et al. [2].
Limitations
This systematic review has several limitations that should be considered when interpreting the findings. First, the included studies were predominantly observational and quasi-experimental in design, which introduces a moderate to serious risk of bias due to confounding, selection bias, and unmeasured differences between intervention and comparator groups. Second, the heterogeneity of integrated care models, populations, settings, and outcome measures limited the ability to perform a quantitative meta-analysis and may reduce the generalizability of results. Third, most studies were conducted in the United States, often within specific healthcare systems such as Medicaid, community mental health centers, or academic medical centers, which may limit applicability to other countries or healthcare contexts. Fourth, several studies relied on administrative data, electronic health records, or claims data, which may underreport clinical nuances, mental health severity, or social determinants affecting ED utilization. Fifth, publication bias is possible, as studies reporting significant reductions in ED use may be more likely to be published than those with null or negative findings. Finally, the review was restricted to English-language publications, which could exclude relevant research from non-English-speaking regions.
Conclusions
This review indicates that primary care-based mental health management can help reduce psychiatric emergency presentations by improving access to timely care, enhancing symptom stabilization, and supporting continuity across services. Integrated models generally demonstrate greater benefit than coordinated or co-located approaches, although outcomes may vary in settings with limited resources or workforce constraints. Reducing psychiatric crises and easing ED burden requires not only strong primary care integration but also broader system-level support, including sufficient staffing and expanded community mental health capacity. When effectively designed and implemented, integrated primary care can play a critical role in reducing emergency psychiatric utilization.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Does the primary care behavioral health model reduce emergency department visits?Health Serv Res Serrano N Prince R Fondow M Kushner K 452945425320182965899310.1111/1475-6773.12862 PMC 6232427 · doi ↗ · pubmed ↗
- 2Evaluating the impact of integrated care on service utilization in serious mental illness Community Ment Health J Waters HC Furukawa MF Jorissen SL 110111085420182994863110.1007/s 10597-018-0297-x · doi ↗ · pubmed ↗
- 3Impact of a mental health based primary care program on emergency department visits and inpatient stays Gen Hosp Psychiatry Breslau J Leckman-Westin E Han B 8135220182947501010.1016/j.genhosppsych.2018.02.008PMC 5936476 · doi ↗ · pubmed ↗
- 4Integrating primary care into community mental health centers: Impact on utilization and costs of health care Psychiatr Serv Krupski A West II Scharf DM 123312396720162736481510.1176/appi.ps.201500424 · doi ↗ · pubmed ↗
- 5Patient-centered medical home membership is associated with decreased hospital admissions for emergency department behavioral health patients Popul Health Manag Adaji A Melin GJ Campbell RL Lohse CM Westphal JJ Katzelnick DJ 1721792120182848606110.1089/pop.2016.0189 · doi ↗ · pubmed ↗
- 6Primary and behavioral health care integration program: impacts on health care utilization, cost, and quality Rand Health Q Breslau J Sorbero MJ Kusuke D 3Rand Health Q 92021 https://pmc.ncbi.nlm.nih.gov/articles/PMC 8383834/34484875 PMC 8383834 · pubmed ↗
- 7Reducing emergency department visits among older adults: a demonstration project evaluation of a low-intensity integrated care model J Integr Care Chen D Torstrick AM Crupi R Schwartz JE Frankel I Brondolo E 3749272019 https://www.emerald.com/jica/article-abstract/27/1/37/220105/Reducing-emergency-department-visits-among-older?redirected From=fulltext
- 8The effects of an enhanced primary care model for patients with serious mental illness on emergency department utilization Community Ment Health J Belson C Sheitman B Steiner B 131113175620203246839110.1007/s 10597-020-00645-0PMC 7438252 · doi ↗ · pubmed ↗