The Impact of Sleep Dysfunction on Inflammatory Skin Diseases: A Systematic Review
Tahani A Moafa, Mohammed E Mojiri, Khlood K Alattas, Ali M Sumayli, Esra H Alnujaidi, Maha O Alharbi, Ramis M Manni, Nawal H Hibili, Faris A Alomir, Faris M Almutairi, Saleh M Alhusayni

TL;DR
Poor sleep worsens skin conditions like eczema and psoriasis, and both conditions can also disrupt sleep, creating a harmful cycle.
Contribution
This systematic review establishes a bidirectional relationship between sleep dysfunction and inflammatory skin diseases, emphasizing the role of pruritus and emotional distress.
Findings
Poor sleep in atopic dermatitis correlates with higher disease severity and itch intensity.
In psoriasis, sleep disturbance is linked to disease severity and worsened quality of life, mediated by depression.
Genetic evidence supports a causal link between insomnia and increased risk of atopic dermatitis and psoriasis.
Abstract
Sleep disturbance is increasingly recognized as a major comorbidity in chronic inflammatory skin diseases, driven by altered sleep architecture, circadian disruption, and pruritus-related nocturnal symptoms that exacerbate disease activity and reduce quality of life. This systematic review of 13 studies (N ≈ 189,000) identified the prevalence, correlates, and clinical implications of sleep disturbance across major dermatologic conditions, focusing on atopic dermatitis (AD) and psoriasis. In AD, poor sleep showed strong associations with higher Scoring Atopic Dermatitis (SCORAD) and Patient-Oriented Eczema Measure (POEM) scores and greater pruritus intensity, with itch emerging as the primary predictor of sleep disruption. In psoriasis, poor sleep was closely linked to higher Psoriasis Area and Severity Index (PASI) and Dermatology Life Quality Index (DLQI) scores and more severe…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
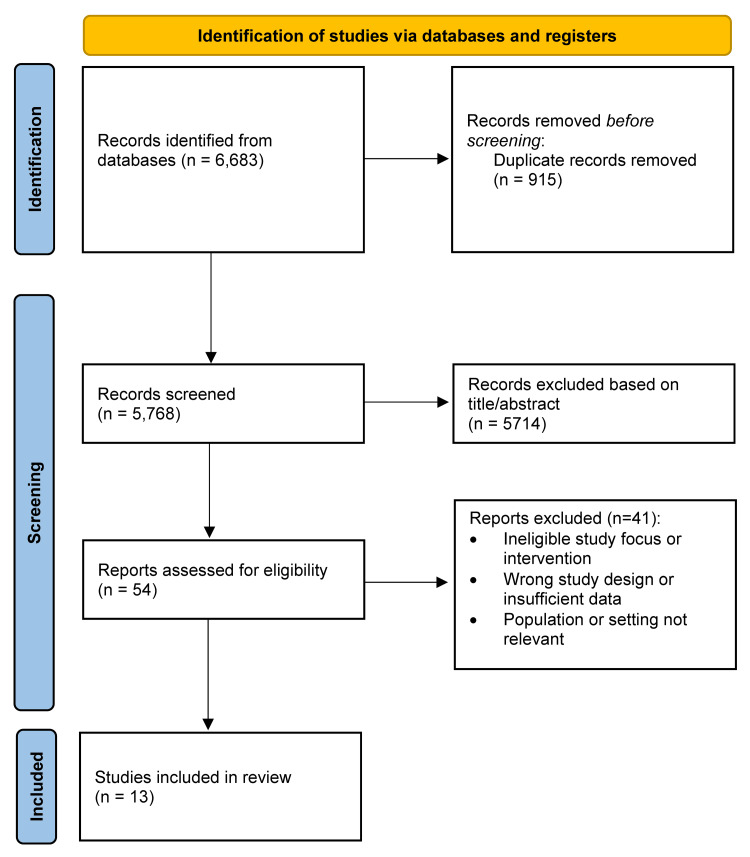 Figure 1
Figure 1| Study (Author) | Country | Study Design | Sample Size | Age (Mean ± SD / Range) | Sex (% Female) | Dermatologic Condition | Sleep Assessment Tool | Disease Severity Measure | Main Outcomes | Statistical Association (r / OR / β / p-value) | Adjustment Variables | Key Findings |
| Fishbein et al. [ | United States | Cross-sectional national survey (PROMIS-based) | 180 children with AD (5–17) | 10.9 ± 3.6 | 44–47% | Atopic dermatitis (physician-diagnosed, stratified by severity) | PROMIS Sleep Disturbance and Sleep-Related Impairment Scales | POEM: mild, moderate, severe | Weighted prevalence of sleep disturbance: 66.9%; severe sleep disturbancee 46.1%; sleep-related impairment 61.2% | OR severe AD = 8.68 (1.82–41.49, p = 0.007); moderate AD = 2.03 (1.00–4.10, p = 0.05); itch β = 1.33 (0.62–2.04, p = 0.003); depression β = 0.67 (0.46–0.88, p < 0.01) | Adjusted for itch intensity, disease severity, age, sex, race, parental income, education | Sleep disturbance is highly prevalent (~3 million U.S. children); severity and itch independently predicted sleep disturbance; associated with depression, anxiety, fatigue, inattention, and impulsivity |
| Arima et al. [ | Japan | Cross-sectional (2013 National Health and Wellness Survey, propensity-matched) | 634 AD patients vs 1,268 non-AD controls | 38.5 ± 12.9 | 0.52 | Atopic dermatitis (physician-diagnosed) | Self-reported physician-diagnosed “sleep disorder” (past 12 months) | Self-rated severity (mild, moderate, severe) | Sleep disorder prevalence in AD vs non-AD and relation to severity | 12.9% vs 4.6%, p < 0.001; no difference between mild and moderate/severe AD | Propensity-score matched on age, sex, marital status, income, BMI, smoking, education, insurance, and comorbidities | AD is significantly associated with higher sleep-disorder prevalence; severity is not predictive of sleep disturbance. |
| Ahn et al. [ | South Korea | Cross-sectional (Korean National Health Insurance Database, 2015) | 182,127 total (42,641 AD; 139,486 non-AD) | Infants to elderly (0–>65) | 0.429 | Atopic dermatitis (AD) compared with nonatopic eczema, urticaria, and psoriasis | ICD-10 diagnostic code G47.9 for sleep disorder | AD severity classified by treatment type: mild (topical), moderate (antihistamines), severe (systemic immunosuppressive therapy) | Prevalence and adjusted odds of sleep disorder by AD status and severity | Overall AD vs non-AD: OR = 0.85 (95% CI: 0.79–0.92, p < 0.001); mild AD OR = 0.88 (p = 0.0237); moderate AD OR = 1.31 (p = 0.0267); severe AD OR = 2.56 (p < 0.0001) | Adjusted for age, gender, economic status, AD history, and concomitant allergic diseases | Severe AD significantly increased the odds of sleep disorder; mild AD was slightly protective |
| Girolomoni et al. [ | EU5 (France, Germany, Italy, Spain, UK) | Cross-sectional analysis (2017 National Health and Wellness Survey) | 1,014 adults with moderate-to-severe AD | Mean 40–42 | 54–72% | Atopic dermatitis (self-reported, physician-diagnosed) | Self-reported insomnia or “sleep difficulties” (mild, moderate, severe) | Dermatology Life Quality Index (DLQI ≥ 6: moderate–extremely large effect) | Sleep difficulties were reported by 61.7% (moderate/severe in 37.8%); associated with poorer HRQoL and work impairment | Moderate/severe sleep difficulty linked with lower SF-36 MCS (36.4–33.1 vs 42.9, p < 0.05), lower EQ-5D (0.52–0.46 vs 0.66, p < 0.05), and higher work impairment (61.7–69.7% vs 52.3%, p < 0.05) | Controlled for age, sex, country, income, employment, BMI, comorbidities, and other atopic diseases | Over 60% of adults with moderate-to-severe AD experience sleep disturbance; severity correlated with worse QoL, work impairment, and higher healthcare utilization |
| Hamid & Qurtas [ | Iraq (Erbil City, Kurdistan) | Cross-sectional clinical study | 100 children (≤18) | 6.84 ± 1.8 (1–18) | 0.46 | Atopic dermatitis (clinically diagnosed, SCORAD-based) | Sleep disturbance recorded by questionnaire (yes/no) | SCORAD index (mild 23%, moderate 69%, severe 8%) | 73% reported sleep disturbance; nearly all severe AD had disturbed sleep (87.5%) | Negative correlation: SCORAD–weight centile r = –0.38, p < 0.001; SCORAD–height centile r = –0.39, p < 0.001 | None reported | Sleep disturbance is prevalent in 73% of AD children; severity is inversely correlated with height and weight; poor sleep likely contributed to impaired growth |
| Ziyab et al. [ | Kuwait | School-based cross-sectional epidemiological study | 3,864 adolescents (11–14) | Median 12 | 0.561 | Eczema (AD, per ISAAC criteria) | Self-reported frequency of nocturnal sleep disturbance due to an itchy rash | Current eczema and “severe eczema” (≥1 night/week sleep disturbance) | 34.4% reported nocturnal sleep disturbance; 12.7% ≥1 night/week; severe eczema prevalence 1.7% | Frequent nocturnal sleep disturbance associated with cesarean delivery (aPR = 1.98, 95% CI 1.37–2.85), ETS exposure (aPR = 1.70, 95% CI 1.18–2.47), dog-keeping (aPR = 1.93, 95% CI 1.06–3.52) | Adjusted for age, mode of birth, ETS exposure, and dog-keeping | One-third of adolescents with eczema experienced nocturnal sleep disturbance; ETS and dog exposure worsened sleep; cesarean section and eczema severity increased night awakenings; antihistamine use rose with more disturbed sleep |
| Melikoğlu [ | Turkey | Case-control study | 58 psoriasis patients vs 58 controls | 41.3 ± 12.4 (18–76) | 0.45 | Plaque psoriasis | Pittsburgh Sleep Quality Index (PSQI) | Psoriasis Area and Severity Index (PASI) | 60.3% of psoriasis patients had poor sleep vs 10.3% of controls | Global PSQI correlated with PASI (p = 0.033); subjective sleep quality (p = 0.048), habitual sleep efficiency (p = 0.044), daytime dysfunction (p = 0.012) correlated | None reported | Psoriasis patients had worse overall and component sleep quality; disease severity was positively associated with poor sleep; sleep disturbance may aggravate psoriasis via immune-inflammatory mechanisms |
| Yang et al. [ | China (Genetic data from UK Biobank & FinnGen) | Two-sample Mendelian randomization study | 4 skin diseases: psoriasis (12,760), acne (4,617), AD (31,245), urticaria (13,990) | Median 24.6–51.4 (varied) | Mixed | Psoriasis, acne, AD, urticaria | GWAS-derived genetic proxies for 8 sleep traits | ICD-10 diagnostic codes for disease classification | Frequent insomnia increased the risk of psoriasis and AD; long sleep duration was protective for acne and urticaria | Psoriasis OR = 1.114 (1.011–1.227, p = 0.029); AD OR = 1.081 (1.003–1.164, p = 0.042); Acne OR = 0.972 (0.948–0.996, p = 0.029); Urticaria OR = 0.988 (0.976–1.000, p = 0.0497) | Adjusted via MR assumptions; pleiotropy tested with MR-Egger and MR-PRESSO | MR confirmed a causal link between insomnia and increased risk of psoriasis and AD; longer sleep is protective against acne and urticaria |
| Sahin et al. [ | Poland | Cross-sectional clinical study with hierarchical regression and mediation analysis | 42 adults with chronic plaque psoriasis | 44.48 ± 17.57 (21–82) | 0.405 | Chronic plaque psoriasis | Pittsburgh Sleep Quality Index (PSQI) | PASI and DLQI | 64.3% reported poor sleep (PSQI > 6); higher PASI, DLQI, itch intensity, and depression associated with worse sleep | PASI–PSQI r = 0.52, p < 0.01; DLQI–PSQI r = 0.68, p < 0.01; hierarchical regression: PASI β = 0.41, DLQI β = 0.37, depression β = 0.37, p < 0.01 | Adjusted for age, gender, BMI, pruritus, and depression | Poorer sleep strongly correlated with disease severity and QoL impairment; depression mediated the relationship between DLQI and sleep; female sex, younger age, and higher BMI predicted worse sleep outcomes |
| Zaky et al. [ | Egypt | Cross-sectional correlational clinical study | 200 psoriasis patients | 38.9 ± 17.8 (6–75) | 0.5 | Psoriasis (plaque, palmoplantar, scalp) | Pittsburgh Sleep Quality Index (Arabic version) | PASI, Pruritus Severity Scale (PSS), Psoriasis Disability Index (PDI) | Poor sleep in 16%; 50% of severe cases; PASI correlated with PSQI | PASI–PSQI p = 0.004; PSS–PSQI r = 0.687, p < 0.001; PDI–PSQI r = 0.571, p < 0.001; regression: Global sleep score = –10.09 + 0.067 × duration + 0.242 × PSS + 0.150 × PDI (R² = 0.648, p < 0.001) | Adjusted for disease duration | Poor sleep is strongly associated with higher pruritus severity and reduced QoL; disease duration, pruritus, and disability predicted sleep impairment; 50% of severe psoriasis cases are affected |
| Atefi et al. [ | Iran | Cross-sectional study in dermatology clinics (Tehran, 2017) | 95 children and adolescents (4–18) | Median 9 (4–18) | 0.505 | Atopic dermatitis (diagnosed clinically and by the 2003 National Survey of Children’s Health criteria) | Pittsburgh Sleep Quality Index (PSQI) | Not specified by score; clinical features (flexor and cheek involvement) used for disease characterization | Sleep disturbance prevalence: 32.6%; relationship with ADHD components | Sleep problem associated with hyperactivity OR = 2.91 (95% CI: 1.04–8.16, p = 0.04); attention deficit OR = 3.68 (95% CI: 1.45–9.33, p = 0.01) | Adjusted for gender and asthma status | Sleep disturbance inADHDD children predicted both hyperactivity and attention deficit; flexor involvement predicted hyperactivity, cheek involvement predicted attention deficit |
| Kong et al. [ | South Korea | Cross-sectional clinical study | 100 total (50 children, 50 adults) | Children: 4.9 ± 3.23; Adults: 26.4 ± 9.56 | Children: 40%; Adults: 56% | Atopic dermatitis (Hanifin & Rajka criteria) | Children: CSHQ; Adults: PSQI | SCORAD index (mild <20; moderate 20–40; severe ≥40) | Children: SCORAD correlated with sleep disturbance; Adults: only certain PSQI components correlated | Children: SCORAD–CSHQ r = 0.28, p < 0.005; Adults: subjective sleep quality r = 0.387, p = 0.007; sleep latency r = 0.318, p = 0.005 | None specified | Sleep quality significantly correlated with disease severity in children; in adults, specific aspects correlated; pruritus was strongly related to poor sleep; sleep problems were linked to reduced QoL |
| Yamaguchi et al. [ | Japan | Population-based cross-sectional survey in nurseries | 468 preschool children (2–6) | 4.5 ± 1.2 | 0.459 | Atopic dermatitis (parent-reported, physician-diagnosed) | Mouth Breathing Daytime (MBD) and Mouth Breathing Sleep (MBS) behavioral scales | No formal AD severity scale | MBD prevalence 35.5%, MBS 45.9%; AD is more prevalent among mouth breathers | MBD–AD OR = 2.4 (95% CI: 1.4–4.2, p = 0.001); MBS–AD OR = 2.4 (95% CI: 1.3–4.2, p = 0.002); adjusted MBD OR = 2.6 (1.3–5.4, p = 0.010); MBS OR = 4.1 (1.8–9.2, p = 0.001) | Adjusted for asthma, allergic rhinitis, family history (AD, asthma, rhinitis), and nasal congestion | Mouth breathing—daytime and during sleep—is associated with a higher prevalence of AD; risk increased with the greater extent of mouth breathing; this suggests that breathing-related sleep disturbance may contribute to AD pathogenesis |
| Study (Author) | Design | Quality Tool | Score | Quality Rating | Key Methodological Notes |
| Fishbein et al. [ | Cross-sectional (U.S. PROMIS database) | AXIS | 18/20 | High | Nationally representative sample; validated sleep tools; no power analysis |
| Arima et al. [ | Cross-sectional (NHWS Japan) | AXIS | 18/20 | High | Propensity-matched population sample; strong analysis; self-reported AD and sleep |
| Ahn et al. [ | Cross-sectional (NHIS database, Korea) | AXIS | 18/20 | High | Large nationwide dataset; robust regression; minor limitation: objective sleep code only (no self-report) |
| Girolomoni et al. [ | Cross-sectional (EU5 NHWS) | AXIS | 18/20 | High | Large multicountry dataset; validated instruments; non-response bias possible |
| Hamid & Qurtas [ | Cross-sectional (Erbil, Iraq) | AXIS | 16/20 | Moderate–High | Valid severity and anthropometric measures; small, single-center sample |
| Ziyab et al. [ | Cross-sectional (Kuwait schools) | AXIS | 19/20 | High | Nationally representative, random sampling; minor reporting limits |
| Melikoğlu [ | Case–control (Turkey) | NOS | 9/9 | High | Rigorous case/control definition, matched sample, validated PSQI, zero attrition |
| Yang et al. [ | Mendelian randomization (UK Biobank & FinnGen) | Q-Genie | 70/77 | High | Strong genetic instrument validity, robust pleiotropy testing, comprehensive sensitivity analysis; large multi-cohort dataset |
| Sahin et al. [ | Cross-sectional (Poland) | AXIS | 16/20 | Moderate–High | Robust stats (mediation model); small sample; single center |
| Zaky et al. [ | Cross-sectional (Egypt) | AXIS | 17/20 | High | Sound analysis; validated Arabic PSQI; single-center sample |
| Atefi et al. [ | Cross-sectional (Tehran clinics) | AXIS | 16/20 | Moderate–High | Valid instruments; limited representativeness; small single-center sample |
| Kong et al. [ | Cross-sectional (Korea) | AXIS | 16/20 | Moderate–High | Validated PSQI/CSHQ; small non-random sample; single-hospital design |
| Yamaguchi et al. [ | Cross-sectional (Japan preschools) | AXIS | 15/20 | Moderate | Large sample but parental self-report; no validated sleep scale |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatology and Skin Diseases · Psoriasis: Treatment and Pathogenesis · Sleep and related disorders
Introduction and background
Sleep is essential for maintaining homeostasis, supporting tissue repair, and regulating immune function. Disrupted sleep contributes to widespread health consequences and may directly influence skin physiology, as the skin participates in circadian regulation and functions as both a barrier organ and a neuro-immunoendocrine interface [1-3]. Altered sleep can modify inflammatory pathways and impair tissue regeneration, creating conditions that may exacerbate dermatologic disease [4,5].
Sleep disorders are highly prevalent in inflammatory skin conditions, such as atopic dermatitis (AD), psoriasis (PSO), chronic urticaria (CU), and acne [1-3,6-10]. While pruritus and pain are the most immediate causes of nocturnal awakening, psychological distress and underlying inflammatory activity also play important roles [3,4,6]. In many patients, sleep loss is not simply a consequence of skin symptoms but a factor that may intensify immune dysregulation, worsen disease activity, and diminish quality of life [1,4,7,10].
Shared neuro-immunologic pathways further reinforce the bidirectional relationship between sleep and dermatologic inflammation. Cytokines involved in cutaneous disease also regulate sleep architecture, while circadian variations in cortisol, skin temperature, and barrier function heighten nighttime pruritus [1,3,8]. These interactions create a self-perpetuating cycle in which sleep loss and inflammation mutually exacerbate one another [2,4,6,9].
Although numerous studies have examined sleep disturbance in dermatologic conditions, findings regarding its relationship with disease severity remain inconsistent [1-13]. Variability in study design, diagnostic criteria, and outcome measures limits direct comparison across conditions. This systematic review aims to synthesize current evidence on the association between sleep disturbance and dermatologic disease severity, identify common mechanisms, and highlight gaps that can inform more integrated approaches to managing both skin disease and sleep health [1-13].
Review
Methods
Literature Search Strategy
A systematic review was conducted in accordance with established reporting guidelines. Comprehensive searches were performed in PubMed, Cochrane Library, Web of Science, and Scopus from database inception to October 2025. Search strategies combined three major concept groups using AND, while synonyms within each concept group were combined using OR. For PubMed, the search string included the following: (sleep OR sleep disorders OR sleep disturbance OR sleep quality OR insomnia) AND (dermatology OR skin disease OR atopic dermatitis OR eczema OR psoriasis OR chronic urticaria OR acne) AND (SCORAD OR PASI OR DLQI OR “disease severity” OR severity index). MeSH terms and free-text keywords were used in parallel to maximize sensitivity. Search strategies were adapted for each database and limited to English-language publications. Two reviewers independently screened all titles and abstracts, followed by full-text review, with disagreements resolved by a third reviewer. The screening process, including reasons for exclusion, was documented in a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram [14]. The PubMed search strategy included terms for sleep (e.g., sleep disorders, sleep quality, insomnia), dermatology (e.g., skin diseases, AD, PSO, CU, acne), and severity indices such as the Scoring Atopic Dermatitis (SCORAD) index [15], the Psoriasis Area and Severity Index (PASI) [16], and the Dermatology Life Quality Index (DLQI) [17]. Search strategies were adapted for each database and limited to English-language publications.
Eligibility Criteria
Studies were eligible if they (1) included patients with any dermatologic condition, (2) assessed sleep disturbance or sleep quality using standardized instruments, and (3) examined the association between sleep disturbance and disease severity using validated clinical indices such as SCORAD, PASI, or DLQI. Eligible designs included cross-sectional, case-control, cohort, and Mendelian randomization studies. Excluded studies included reviews, case reports, conference abstracts, letters, editorials, non-human studies, non-dermatologic populations, and studies lacking quantitative measures of sleep or disease severity. Only full-text articles in English were included.
Data Extraction and Quality Appraisal
Data were extracted into a standardized template by two independent reviewers. Extracted variables included study characteristics, participant demographics, dermatologic condition, sleep assessment method, disease severity measure, key findings, and statistical outcomes. Quality appraisal was performed according to study design: the Appraisal Tool for Cross-Sectional Studies (AXIS) for cross-sectional studies [18], the Newcastle-Ottawa Scale (NOS) for case-control studies [19], and the Q-Genie tool for Mendelian randomization studies [20]. Each domain was rated for risk of bias, and the overall quality of included studies ranged from moderate-high to high.
Results
Study Selection
The database search yielded 6,683 records. After removing duplicates, 5,768 unique studies were screened by title and abstract, resulting in the exclusion of 5,714 non-eligible records. Fifty-four full-text articles were assessed, and 41 were excluded for reasons including inappropriate study design, non-dermatologic populations, or insufficient data. Thirteen studies met all inclusion criteria and were included in the qualitative synthesis. No studies met the criteria for meta-analysis due to heterogeneity in design, populations, and outcome measures. The full screening process is presented in the PRISMA diagram (Figure 1).
PRISMA flow diagram of the study selection processPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Study Characteristics
The 13 included studies, published between 2015 and 2025, represented populations from Asia, Europe, North America, and Africa. Most were cross-sectional designs [2-6,9,10], with one case-control study [7] and one Mendelian randomization study [8]. Sample sizes ranged from 42 to over 180,000 participants. Age groups spanned early childhood to older adulthood, and female representation generally ranged between 40% and 60% (Table 1).
AD and PSO were the most commonly studied conditions, with additional studies on eczema, acne, and CU [6,8,11]. Sleep was assessed using validated tools such as the PSQI [7,9,10], the Children’s Sleep Habits Questionnaire (CSHQ) [12], and the Patient-Reported Outcomes Measurement Information System (PROMIS) sleep scales [1], as well as self-reported questionnaires [2,4]. Large-scale datasets often relied on diagnostic codes [3]. Disease severity was most frequently measured using SCORAD for AD [5] and PASI or DLQI for PSO [7], although some studies used self-rated severity or clinical features [2,11].
Across studies, sleep disturbance affected 30%-70% of patients with dermatologic disease. Greater disease severity, higher itch intensity, and psychological comorbidity were consistently associated with worse sleep [1,4,9]. Pediatric cohorts demonstrated frequent nocturnal awakenings and daytime behavioral consequences [5,11,12], while adults commonly reported reduced productivity and impaired quality of life [4,10]. Genetic evidence supported these findings: insomnia increased the risk of AD and PSO, whereas longer sleep duration reduced the risk of acne and CU [8]. Environmental factors such as nocturnal itching, tobacco smoke exposure, and mouth breathing during sleep further contributed to sleep disruption [6,13].
Quality Assessment
Methodological quality ranged from moderate-high to high (Table 2). Cross-sectional studies scored 15-19 of 20 on the AXIS tool, reflecting clear objectives, appropriate design, valid measurement methods, and transparent statistical reporting. Common limitations included limited sample representativeness, incomplete reporting of recruitment procedures, and insufficient justification of sample size. Large population-based studies more adequately addressed these issues [3,6].
The case-control study achieved the maximum NOS score, indicating strong internal validity [7]. The Mendelian randomization study (Q-Genie appraisal) demonstrated excellent methodological quality with robust genetic instrumentation and comprehensive sensitivity analyses [8]. All studies reported ethical approval and funding sources, supporting overall reliability.
Associations Between Sleep Disturbance and Dermatologic Conditions
Sleep disturbance was highly prevalent across dermatologic conditions, with rates ranging from 16% to over 70%. Poor sleep consistently correlated with greater disease severity, diminished quality of life, and heightened psychological symptoms. Pruritus, pain, and emotional distress frequently mediated these associations, emphasizing the bidirectional relationship between inflammation and sleep dysregulation.
In AD, sleep disturbance was one of the most burdensome symptoms across age groups [1,2,5,11-13]. Increased disease severity was associated with higher rates of sleep impairment, with pruritus emerging as the strongest predictor. Pediatric studies documented additional neurobehavioral consequences, including attention difficulties and hyperactivity [11,12]. Mouth breathing during sleep further contributed to nocturnal arousals in children [13]. Psychological distress - including anxiety and depression - amplified sleep disruption and reduced quality of life [2,4].
In PSO, sleep disturbance ranged from 16% to over 60%, depending on disease severity. Poor sleep correlated with PASI scores, pruritus intensity, and impaired quality of life [7,9,10]. Depression frequently mediated the relationship between disease severity and sleep impairment, underscoring the importance of emotional factors. Younger age, female sex, and higher body mass index (BMI) were additional predictors of poor sleep [9].
Other dermatologic conditions showed similar patterns. Mendelian randomization analyses demonstrated that insomnia increased the risk of AD and PSO, while longer sleep duration reduced the risk of acne and CU [8], supporting a causal bidirectional relationship.
Discussion
This systematic review synthesizes evidence from 13 studies spanning diverse populations and methodological approaches to clarify the association between sleep disturbance and dermatologic disease severity. Across studies, sleep disruption was consistently common, affecting approximately one-third to two-thirds of individuals with skin disease, with higher rates observed in moderate-to-severe conditions. Despite substantial heterogeneity in measurement tools, age groups, and disease categories, a consistent pattern emerged: greater dermatologic disease severity, higher pruritus intensity, and increased psychological burden were strongly linked to poorer sleep outcomes.
AD was the most frequently studied condition, reflecting the well-established burden of nocturnal itching. Findings across pediatric and adult cohorts were largely concordant. Studies using validated severity indices such as SCORAD, POEM, and DLQI demonstrated that worsening AD severity corresponded with increased sleep disturbance, nocturnal awakenings, and impaired restorative sleep [1,5,12]. Pruritus emerged as the strongest and most consistent mediator of sleep impairment. In children, these disturbances extended beyond nighttime symptoms and were associated with measurable daytime behavioral effects, including hyperactivity, attentional difficulties, and reduced school functioning [11,12]. Environmental and physiological modifiers - such as exposure to environmental tobacco smoke, dog-keeping, and mouth breathing - further exacerbated sleep disruption among younger populations [6,13].
In psoriasis, the relationship between disease severity and sleep impairment was similarly evident. Multiple clinical studies demonstrated that PASI and pruritus severity were significantly correlated with poor sleep quality and greater daytime dysfunction [7,9,10]. Sleep disruption in psoriasis may reflect a combination of inflammatory cytokine dysregulation, discomfort from plaques, and psychological distress. Indeed, studies that incorporated mediation models found that depression and reduced quality of life partially explained the association between psoriasis severity and poor sleep [9]. This highlights the multidimensional nature of sleep disturbance, where dermatologic, psychological, and lifestyle components intersect.
Emerging evidence also highlighted disease-specific nuances. Mendelian randomization findings supported a potential causal relationship between insomnia and increased risk of AD and psoriasis, while longer sleep duration appeared protective for acne and chronic urticaria [8]. These genetic data strengthen the plausibility of a bidirectional relationship: skin inflammation disrupts sleep, and sleep dysregulation may in turn exacerbate inflammatory pathways relevant to dermatologic disease. Additionally, non-AD eczema and urticaria cohorts demonstrated that nocturnal itching and sleep fragmentation remain substantial burdens even in the absence of classic AD presentations [3,6].
Despite variability in study design, several unifying themes emerge. First, itch - whether due to AD, psoriasis, or urticarial conditions - remains the most powerful predictor of sleep disturbance. Second, psychological comorbidities such as anxiety, depression, and fatigue frequently co-occur with poor sleep outcomes and may act as both contributors to and consequences of sleep disruption. Third, sleep impairment is associated with broader functional impacts, including reduced productivity, increased healthcare utilization, impaired growth in children, and higher rates of behavioral concerns. The consistent presence of these associations across cultures, age groups, and measurement methods strengthens confidence in the observed relationships.
Overall, this systematic review highlights that sleep disturbance is a core component of dermatologic disease burden rather than an ancillary symptom. These findings emphasize the need for clinicians to routinely assess sleep quality in patients with chronic skin conditions and to integrate sleep-focused interventions - such as itch management, behavioral sleep strategies, or treatment of comorbid psychological symptoms - into comprehensive dermatologic care.
Limitations
This review has several limitations. First, the included studies showed substantial heterogeneity in study design, sleep assessment tools, disease severity measures, age groups, and outcome reporting, which precluded a meta-analysis. Many studies relied on cross-sectional designs, limiting causal inference, and several used self-reported diagnoses or non-validated sleep measures, introducing the risk of misclassification. Sample sizes varied widely, with some studies based on small, single-center populations, reducing generalizability. Although most studies adjusted for key confounders, residual confounding - particularly related to psychological symptoms, socioeconomic factors, and comorbid allergic disease - remains possible. Pediatric and adult data were unevenly represented across conditions, and relatively few studies assessed nighttime physiological parameters (e.g., actigraphy). Finally, publication bias is possible, as studies reporting positive associations may be more likely to be published.
Conclusions
Sleep disturbance is a significant and multidimensional component of chronic dermatologic disease. Evidence across AD, PSO, CU, acne, and related conditions supports a bidirectional relationship driven by pruritus, pain, psychological factors, and underlying inflammation. These findings underscore the importance of routinely assessing sleep in dermatologic care and adopting multidisciplinary management approaches that incorporate sleep-focused behavioral strategies, psychological support, and targeted anti-inflammatory treatments. Future research should prioritize mechanistic and interventional studies to clarify causal pathways and determine whether improving sleep can enhance both skin-specific and overall health outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sleep disturbance in school-aged children with atopic dermatitis: prevalence and severity in a cross-sectional sample J Allergy Clin Immunol Pract Fishbein AB Cheng BT Tilley CC 31203129920213399170410.1016/j.jaip.2021.04.064PMC 8355069 · doi ↗ · pubmed ↗
- 2Burden of atopic dermatitis in Japanese adults: analysis of data from the 2013 National Health and Wellness Survey J Dermatol Arima K Gupta S Gadkari A 3903964520182938833410.1111/1346-8138.14218 PMC 5947641 · doi ↗ · pubmed ↗
- 3Cross-sectional study of psychiatric comorbidities in patients with atopic dermatitis and nonatopic eczema, urticaria, and psoriasis Neuropsychiatr Dis Treat Ahn HJ Shin MK Seo JK Jeong SJ Cho AR Choi SH Lew BL 146914781520193123968210.2147/NDT.S 191509 PMC 6551560 · doi ↗ · pubmed ↗
- 4The economic and psychosocial comorbidity burden among adults with moderate-to-severe atopic dermatitis in Europe: analysis of a cross-sectional survey Dermatol Ther (Heidelb) Girolomoni G Luger T Nosbaum A Gruben D Romero W Llamado LJ Di Bonaventura M 1171301120213318032010.1007/s 13555-020-00459-8PMC 7858996 · doi ↗ · pubmed ↗
- 5Growth parameters in children with atopic dermatitis in Erbil city, Kurdistan region-Iraq Bali Med J Hamid AM Qurtas DS 74574892020
- 6Eczema among adolescents in Kuwait: prevalence, severity, sleep disturbance, antihistamine use, and risk factors World Allergy Organ J Ziyab AH Holloway JW Ali YM Zhang H Karmaus W 1007311620223660126010.1016/j.waojou.2022.100731 PMC 9791032 · doi ↗ · pubmed ↗
- 7Sleep quality and its association with disease severity in psoriasis Eurasian J Med Melikoglu M 124127492017 https://pubmed.ncbi.nlm.nih.gov/28638255/2863825510.5152/eurasianjmed.2017.17132 PMC 5469838 · doi ↗ · pubmed ↗
- 8Association between specific sleep traits and four inflammatory skin diseases: a Mendelian randomization study Clin Cosmet Investig Dermatol Yang P Huang Y He W Chen T Wei S Zhao Y 2509252118202510.2147/CCID.S 541688 PMC 1249389541050715 · doi ↗ · pubmed ↗