Denosumab Versus Bisphosphonates in Glucocorticoid-Induced Osteoporosis: A Systematic Review
Anas E Ahmed, Waleed A Alzaylaee, Abdullah S Suhluli, Shahd A Essa, Latifah M Bahkali, Alanood M Hakami, Razan A Alshamrani, Fahad R Alharbi, Roaa H Alhazmi, Tassnim H Khurayzi, Abdulmalik K Almihbash

TL;DR
This review compares denosumab and bisphosphonates for treating bone loss caused by steroids, finding denosumab more effective in improving bone density and structure.
Contribution
The study provides a systematic comparison of denosumab and bisphosphonates in glucocorticoid-induced osteoporosis using diverse clinical and imaging data.
Findings
Denosumab showed greater increases in lumbar spine bone mineral density compared to bisphosphonates.
Denosumab preserved cortical thickness and trabecular density better than bisphosphonates.
Fracture outcomes were similar between the two treatments due to limited study power.
Abstract
Glucocorticoid-induced osteoporosis (GIOP) is a major cause of secondary bone loss characterized by rapid trabecular deterioration and increased fracture risk, and while bisphosphonates are widely used as first-line therapy, the comparative effectiveness of denosumab remains clinically relevant. This systematic review synthesized evidence from randomized trials, imaging studies, and observational cohorts evaluating denosumab versus bisphosphonates in adults receiving glucocorticoids, focusing on bone mineral density, bone turnover, microarchitecture, fractures, and safety. Denosumab consistently produced greater increases in lumbar spine bone mineral density, with modest but generally favorable effects at the hip and variable advantages at the femoral neck. High-resolution imaging suggested superior preservation of cortical thickness, trabecular density, and estimated bone strength with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
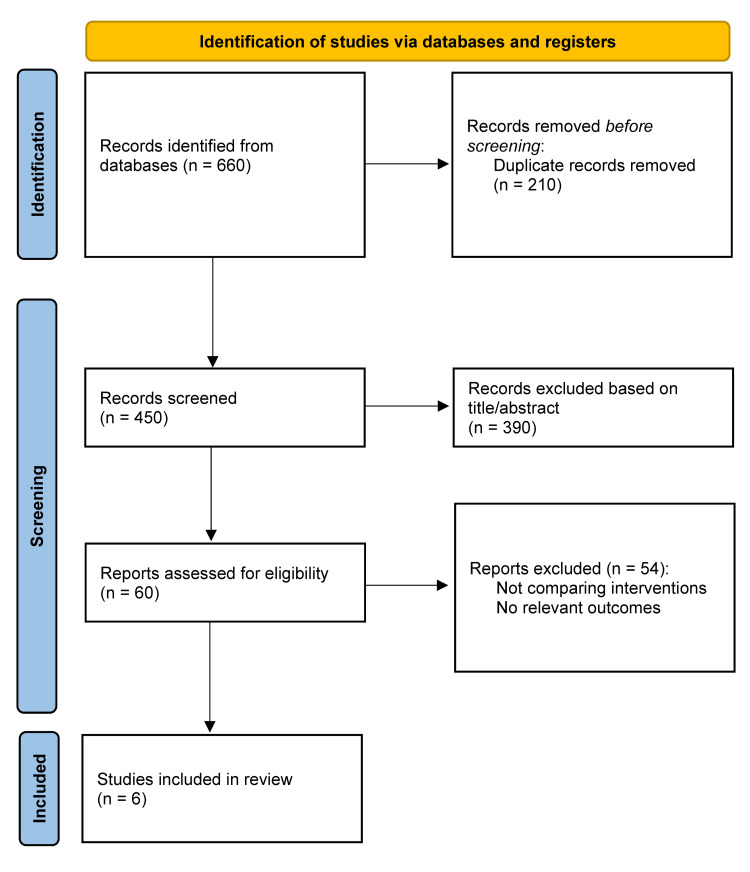 Figure 1
Figure 1| Study | Country | Study design | Population | Glucocorticoid details | Sample size (denosumab vs BP) | Denosumab regimen | Bisphosphonate regimen | Follow-up duration | Primary outcome | Secondary outcomes | Lumbar spine BMD change (%) | Total hip BMD change (%) | Femoral neck BMD change (%) | Bone turnover markers | Fractures | Adverse events | Key notes |
| Geusens et al. [ | Multinational | RCT substudy (HR-pQCT imaging) | GIOP patients (initiators & continuers) | Prednisone ≥7.5 mg/day | D: 55, BP: 55 | 60 mg SC q6 months | Risedronate 5 mg daily | 24 months | Bone strength (failure load, radius & tibia) | Cortical & trabecular microarchitecture | Not measured | Not measured | Not measured | Not measured | Not assessed | No new safety signals | Denosumab preserved/improved bone strength; BP associated with cortical deterioration |
| Mok et al. [ | Hong Kong | Randomized controlled trial (open-label, 1:1) | Women on ≥2 yrs of oral BP + long-term GCs | Prednisolone ≥2.5 mg/day for ≥1 yr (mean 101 mo; mean dose 4.4 mg/day) | D: 21, BP: 21 | 60 mg SC q6 months | Continued BP: ALN 79%, RIS 12%, IBN 10% | 12 months | Lumbar spine BMD change | Hip BMD; FN BMD; BTMs; fractures; safety | +3.4% ± 0.9% vs +1.5% ± 0.4% (p = 0.01 adj.) | +1.38% vs +0.80% (NS) | −0.14% vs +0.57% (NS) | Denosumab suppressed P1NP & β-CTX more strongly | No vertebral or non-vertebral fractures | URTI slightly higher in D; no SAEs | BP inadequate responders; denosumab superior for LS BMD & BTMs |
| Saag et al. [ | Multinational | Randomized, double-blind, double-dummy Phase III RCT | Adults with GIOP (initiators & continuers) | ≥7.5 mg/day prednisone | D: 398, BP: 397 | 60 mg SC q6 months | Risedronate 5 mg daily | 24 months | Lumbar spine BMD change | TH & FN BMD; radius BMD; BTMs; fractures; safety | Initiators: +6.2% vs +1.7%; Continuers: +6.4% vs +3.2% | Initiators: +3.1% vs 0.0%; Continuers: +2.9% vs +0.5% | Initiators: +1.5% vs −0.9%; Continuers: +2.2% vs +0.4% | Stronger CTX & P1NP suppression with denosumab | Any: 8.8% vs 9.1%; Vertebral: 4.4% vs 6.9%; Non-vertebral: 5.3% vs 3.8% | Similar AE rates; 1 atypical femoral fracture in D; no ONJ | Largest high-quality RCT; robust evidence of denosumab superiority |
| Handa et al. [ | Japan | Retrospective cohort | Neuroimmunological disorders (NMOSD, MG, CIDP) on long-term GCs | Median PSL ~10 mg/day; >3 months | D: 23, BP: 34 | 60 mg SC q6 months | Mixed BP: ALN, RIS, minodronate | Up to 6 years | LS & TH BMD % change | Fractures | LS: +4.1 → +9.7 → +6.6% vs BP −0.8 → −0.6 → −0.7% | TH: +2.3 → +4.3 → +7.1% vs BP −2.1 → −2.2 → −2.6% | Not reported | Not measured | 2/23 vs 2/34 (2 yrs); 2/8 vs 5/33 (6 yrs) | No hypocalcemia, no ONJ; similar AEs | Longest follow-up; denosumab consistently superior; retrospective design limits certainty |
| Mok et al. [ | Hong Kong | Randomized controlled trial (open-label, 1:1) | Adults on long-term GCs (81% SLE) | Prednisolone ≥2.5 mg/day for ≥1 yr (mean 5.1 mg/day) | D: 69, ALN: 70 | 60 mg SC q6 months | Alendronate 70 mg weekly | 12 months | Lumbar spine BMD | TH BMD; FN BMD; BTMs; AEs | +3.5% ± 2.5% vs +2.5% ± 2.9% (p = 0.045 adj.) | +0.9% vs +1.6% (NS) | +1.04% vs +1.5% (NS) | Stronger suppression: P1NP 53% vs 22%; CTX 57% vs 5.3% | 2 vertebral fractures in each group | AE rates similar; no ONJ; mild infections slightly ↑ in D | Largest ALN comparison in GC users; denosumab superior for LS BMD & BTMs |
| Iseri et al. [ | Japan | Prospective, randomized, open-label trial | Adults with glomerular disease & new GIOP | Median PSL 5 mg/day (29% <3 mo; 71% ≥3 mo) | D: 14, ALN: 14 | 60 mg SC q6 months + calcitriol | Alendronate 35 mg weekly + calcitriol | 12 months | % change LS BMD | FN BMD; UD radius; BTMs; safety | +5.3% ± 1.0% (p<0.01); superior to ALN (p<0.05) | No significant change | +1.8% ± 1.1% (NS); ALN slightly declined | Strong suppression of TRACP-5b, BAP, t-P1NP | 1 femoral neck fracture in D | Mild hypocalcemia; eczema flare; TB case; none severe | First ALN-controlled RCT in GIOP; denosumab significantly improved LS BMD |
| Study | Reporting (0-10) | External validity (0-3) | Internal validity - bias (0-7) | Internal validity - confounding (0-6) | Power (0-2) | Total score (0-28) | Quality rating |
| Geusens et al. [ | 10 | 1 | 7 | 5 | 0 | 23 / 28 | Good |
| Mok et al. [ | 10 | 2 | 6 | 5 | 2 | 25 / 28 | Good |
| Saag et al. [ | 10 | 3 | 7 | 6 | 2 | 28 / 28 | Excellent |
| Handa et al. [ | 9 | 1 | 4 | 2 | 0 | 16 / 25 | Fair |
| Mok et al. [ | 10 | 2 | 6 | 5 | 2 | 25 / 28 | Good |
| Iseri et al. [ | 10 | 2 | 6 | 4 | 2 | 24 / 28 | Good |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone health and osteoporosis research · Bone and Joint Diseases · Bone Metabolism and Diseases
Introduction and background
Glucocorticoid-induced osteoporosis (GIOP) is the most common form of secondary osteoporosis and a major concern for patients requiring long-term systemic glucocorticoid therapy. Even low doses accelerate bone loss by disrupting normal bone remodeling, leading to reduced bone formation, increased bone resorption, and a rapid decline in bone mineral density (BMD) within the first few months of treatment [1-3]. These changes significantly increase the risk of fragility fractures, particularly vertebral fractures, which contribute to substantial morbidity and healthcare burden. Despite multiple available therapeutic options, optimizing bone protection in glucocorticoid-treated patients remains a clinical priority [1-4].
Bisphosphonates have traditionally served as first-line therapy due to their established ability to reduce bone turnover and increase BMD at major skeletal sites [2,5,6]. However, limitations such as dependence on remodeling surfaces, poor gastrointestinal absorption, long skeletal retention, and reduced effectiveness in some high-risk or previously treated patients have highlighted the need for alternatives [2,5,6].
Denosumab, a monoclonal antibody targeting receptor activator of nuclear factor κB ligand (RANKL), offers a distinct antiresorptive mechanism by suppressing osteoclast formation and activity. It produces rapid reductions in bone turnover and substantial gains in both cortical and trabecular bone across various osteoporosis populations [1,2,3]. Its reversible action, convenient administration, and suitability for patients with renal impairment further enhance its clinical utility [1,4,6]. Emerging evidence suggests that denosumab may provide greater improvements in BMD than bisphosphonates in individuals receiving glucocorticoids [1-3,6].
However, uncertainty persists regarding the comparative benefits and risks of denosumab, specifically in the context of GIOP. Existing studies vary in patient characteristics, glucocorticoid exposure, duration, and outcome reporting, and long-term fracture data remain limited [1-6]. A systematic evaluation of the available evidence is therefore warranted to clarify whether denosumab provides meaningful advantages over bisphosphonates for patients undergoing glucocorticoid therapy [1-6].
This systematic review aims to synthesize evidence comparing denosumab and bisphosphonates in adults with GIOP, focusing on changes in BMD at key skeletal sites, bone turnover markers, fractures, and adverse events to inform clinical decision making in this high-risk population [1-6].
Review
Methods
Literature Search Strategy
A systematic search was conducted across PubMed, Scopus, Web of Science, and the Cochrane Library for all available studies up to December 2025. Search terms included combinations related to glucocorticoid-induced osteoporosis, osteoporosis and bone density outcomes, denosumab, and bisphosphonates, with filters for comparative study designs. Searches were restricted to human studies in English and to original research directly comparing denosumab with bisphosphonates in adults receiving systemic glucocorticoids.
Eligibility Criteria
Eligibility was defined according to the Population-Intervention-Comparator-Outcome framework [7]. Included studies examined adults receiving systemic glucocorticoids for any medical condition, with denosumab as the intervention and any oral or intravenous bisphosphonate as the comparator. Studies were required to report at least one skeletal outcome, including BMD, bone turnover markers, bone microarchitecture, or fractures. Eligible designs included randomized controlled trials (RCTs), prospective studies, and retrospective comparative cohorts. Exclusion criteria were non-comparative designs, non-bisphosphonate comparators, case reports, reviews, conference abstracts, pediatric studies, laboratory research, and studies lacking extractable skeletal outcomes.
Study Selection
All records were imported into reference management software for duplicate removal. Two reviewers independently screened titles and abstracts, followed by full-text assessment of potentially eligible studies. Disagreements were resolved through discussion or adjudication by a third reviewer. The selection process is summarized in a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram [8].
Data Extraction and Quality Appraisal
Two reviewers independently extracted data on study design, participant characteristics, glucocorticoid exposure, interventions, comparators, follow-up duration, and skeletal outcomes. Extracted data were cross-checked for accuracy. Quality assessment was performed using the Downs and Black checklist, evaluating reporting quality, external validity, internal validity, and statistical power [9]. Quality ratings informed the interpretation of findings in the qualitative synthesis.
Results
Study Selection
The database search initially identified 660 records. After removing duplicates, 450 studies were screened, and 390 were excluded based on title and abstract. Sixty full-text articles were assessed, of which 54 were excluded for lacking comparative interventions, not involving glucocorticoid-induced osteoporosis (GIOP) populations, or not reporting relevant skeletal outcomes. Six studies met all inclusion criteria [1-6]. Heterogeneity in study design and outcomes precluded quantitative meta-analysis (Figure 1).
PRISMA flow diagram of the study selection processPRISMA - Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Baseline Characteristics of Included Studies
The six included studies consisted of four randomized controlled trials (RCTs), one high-resolution peripheral quantitative computed tomography (HR-pQCT) mechanistic substudy, and one long-term retrospective cohort. The largest RCT by Saag et al. [3] demonstrated greater improvements in lumbar spine, total hip, and femoral neck bone mineral density (BMD) with denosumab compared with risedronate. The HR-pQCT substudy by Geusens et al. [1] provided mechanistic evidence of superior preservation of cortical thickness, trabecular density, and estimated bone strength with denosumab. Additional RCTs by Mok et al. [2,4] and Iseri et al. [5] reported larger lumbar spine BMD gains and deeper suppression of bone turnover markers with denosumab. The retrospective cohort by Handa et al. [6] demonstrated sustained long-term increases in lumbar spine and hip BMD with denosumab, whereas patients treated with bisphosphonates exhibited minimal or declining trends over time (Table 1).
Quality Assessment
Overall quality was high. Saag et al. [3] achieved the highest score, and the RCTs by Mok et al. [2,4] and Iseri et al. [5] were rated good to excellent. The HR-pQCT substudy [1] demonstrated good internal validity despite a smaller imaging subset. The retrospective cohort [6] was rated Fair due to inherent design limitations but contributed meaningful long-term data (Table 2).
Lumbar Spine BMD
Denosumab consistently produced the largest and most consistent gains in lumbar spine BMD. In the largest RCT [3], increases of +6.2% to +6.4% over 24 months exceeded those observed with risedronate. Similar superiority was reported in the RCTs by Mok et al. [2,4], in the trial by Iseri et al. [5], and in the long-term follow-up of Handa et al. [6].
Total Hip BMD
Total hip BMD generally favored denosumab. Saag et al. [3] reported significantly greater gains across all glucocorticoid exposure groups. Other RCTs reported smaller or nonsignificant differences [2,4,5], whereas the retrospective cohort demonstrated sustained improvements with denosumab and declines with bisphosphonates [6].
Femoral Neck BMD
Femoral neck outcomes were more variable. Saag et al. [3] observed significant improvements with denosumab, while smaller RCTs showed minimal between-group differences [2,4,5].
Bone Microarchitecture
The HR-pQCT substudy [1] demonstrated that denosumab more effectively preserved cortical thickness, trabecular density, and estimated bone strength at the radius and tibia, whereas risedronate was associated with cortical deterioration.
Bone Turnover Markers
All RCTs [2-5] consistently reported deeper suppression of bone turnover markers, including C-terminal telopeptide (CTX), procollagen type I N-terminal propeptide (P1NP), and tartrate-resistant acid phosphatase 5b (TRACP-5b), reflecting denosumab's potent antiresorptive activity.
Fracture Outcomes
Fracture rates were low across the studies. The largest RCT [3] and the long-term retrospective cohort [6] reported no significant differences in vertebral or nonvertebral fractures between the denosumab and bisphosphonate groups. Smaller RCTs reported no new fractures, limiting conclusions regarding comparative fracture reduction.
Safety Outcomes
Both therapies were generally well tolerated. Denosumab was associated with slightly higher rates of mild infections in some studies [2,4] and occasional hypocalcemia [5], whereas bisphosphonates were more frequently linked to gastrointestinal adverse effects. No cases of osteonecrosis of the jaw were reported. Overall, denosumab demonstrated consistent advantages in BMD and bone turnover suppression with comparable safety to bisphosphonates.
Conclusions
This systematic review indicates that denosumab provides meaningful benefits over bisphosphonates for glucocorticoid-induced osteoporosis, particularly in improving lumbar spine BMD and suppressing bone turnover. While evidence for fracture reduction remains limited due to low event rates and short follow-up durations, the available data support denosumab as an effective therapeutic option, especially for patients who respond inadequately to bisphosphonates. Larger and longer-term RCTs with fracture endpoints are needed to better define its comparative effectiveness.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Effect of denosumab compared with risedronate on bone strength in patients initiating or continuing glucocorticoid treatment J Bone Miner Res Geusens P Bevers MS van Rietbergen B 113611463720223534006210.1002/jbmr.4551 PMC 9324223 · doi ↗ · pubmed ↗
- 2Denosumab versus alendronate in long-term glucocorticoid users: a 12-month randomized controlled trial Bone Mok CC Ho LY Leung SM Cheung HN Chen SP Ma KM 11590214620213363135510.1016/j.bone.2021.115902 · doi ↗ · pubmed ↗
- 3Denosumab versus risedronate in glucocorticoid-induced osteoporosis: final results of a twenty-four-month randomized, double-blind, double-dummy trial Arthritis Rheumatol Saag KG Pannacciulli N Geusens P 117411847120193081664010.1002/art.40874 PMC 6619388 · doi ↗ · pubmed ↗
- 4Effects of denosumab and bisphosphonates on glucocorticoid-induced osteoporosis in patients with neuroimmunological disorders Intern Med Handa H Uzawa A Mori M 5435496420253898718310.2169/internalmedicine.3954-24PMC 11904454 · doi ↗ · pubmed ↗
- 5Switching of oral bisphosphonates to denosumab in chronic glucocorticoid users: a 12-month randomized controlled trial Bone Mok CC Ho LY Ma KM 2222287520152576143410.1016/j.bone.2015.03.002 · doi ↗ · pubmed ↗
- 6The effects of denosumab and alendronate on glucocorticoid-induced osteoporosis in patients with glomerular disease: a randomized, controlled trial P Lo S One Iseri K Iyoda M Watanabe M 013201810.1371/journal.pone.0193846 PMC 585434429543887 · doi ↗ · pubmed ↗
- 7Utilization of the PICO framework to improve searching Pub Med for clinical questions BMC Med Inform Decis Mak Schardt C Adams MB Owens T Keitz S Fontelo P 16720071757396110.1186/1472-6947-7-16PMC 1904193 · doi ↗ · pubmed ↗
- 8The PRISMA 2020 statement: an updated guideline for reporting systematic reviews BMJ Page MJ Mc Kenzie JE Bossuyt PM 0372202110.1186/s 13643-021-01626-4PMC 800853933781348 · doi ↗ · pubmed ↗