A Near-Miss Event: Constrictive Pericarditis Misdiagnosed as Heart Failure With Preserved Ejection Fraction
Karuna Rayamajhi, Fnu Parul, Majid Yavari, Kent Brummel, Christopher Scoma

TL;DR
A 66-year-old woman with rheumatoid arthritis was misdiagnosed with heart failure, but later found to have constrictive pericarditis, highlighting the need for careful echocardiographic evaluation.
Contribution
This case emphasizes the diagnostic challenges of constrictive pericarditis and the importance of multimodal imaging and expert evaluation.
Findings
Initial echocardiogram missed signs of constrictive pericarditis, leading to a misdiagnosis of heart failure.
Repeat echocardiogram and MRI confirmed constrictive pericarditis with features like ventricular septal bounce and annulus reversus sign.
The patient fully recovered after undergoing pericardiectomy.
Abstract
Constrictive pericarditis (CP) is often misdiagnosed, making echocardiography essential for initial evaluation. We present a case of misdiagnosed constrictive pericarditis in a 66-year-old female with rheumatoid arthritis who presented with shortness of breath. A transthoracic echocardiogram (TTE) performed by a cardiologist initially reported diastolic dysfunction, leading to a diagnosis of heart failure with preserved ejection fraction (HFpEF), and she was discharged on diuretics. Despite adherence to therapy, she was readmitted multiple times for worsening symptoms over 18 months. A repeat TTE revealed ventricular septal bounce in early diastole and a positive annulus reversus sign, both of which were missed on the initial study. Ventricular septal bounce in early diastole reflects abnormal interventricular dependence due to a noncompliant, often thickened pericardium, which…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
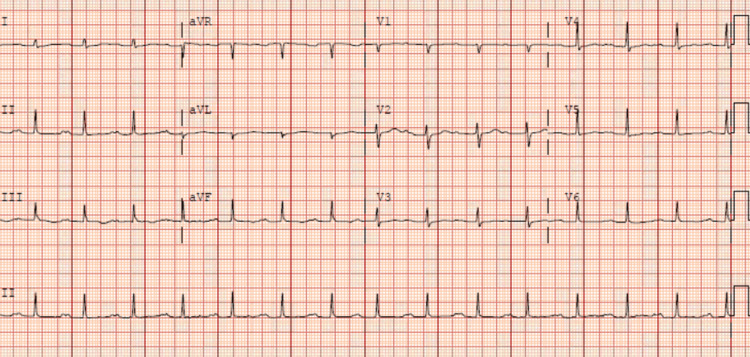 Figure 1
Figure 1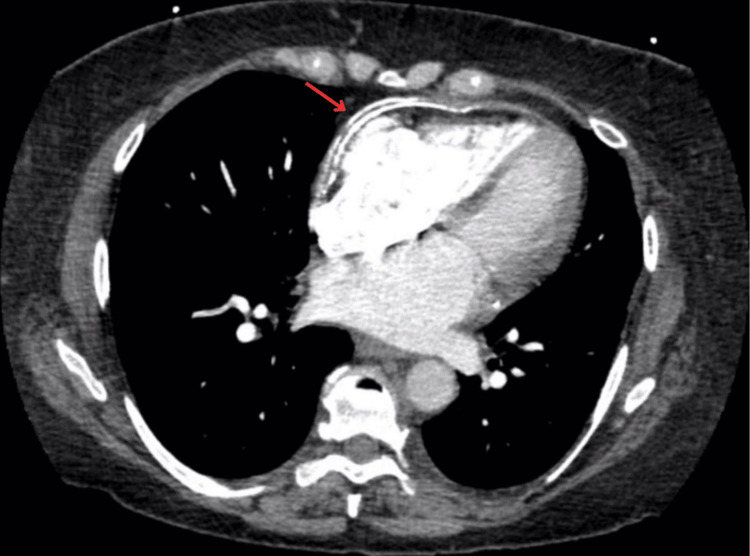 Figure 2
Figure 2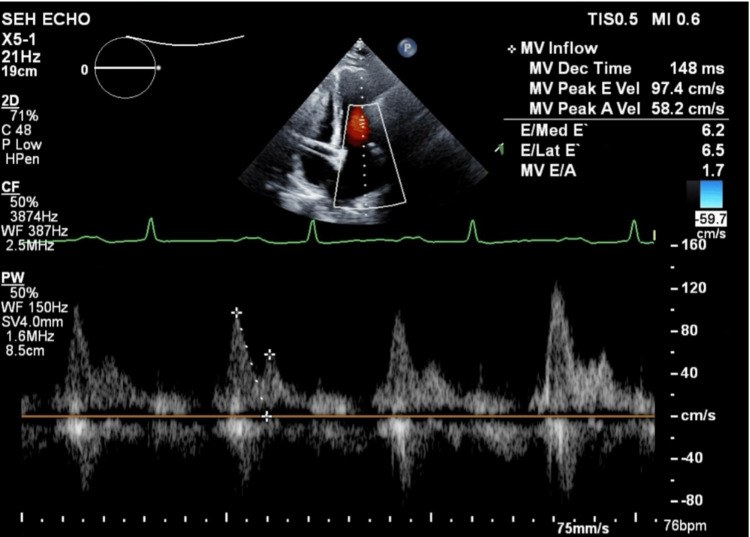 Figure 3
Figure 3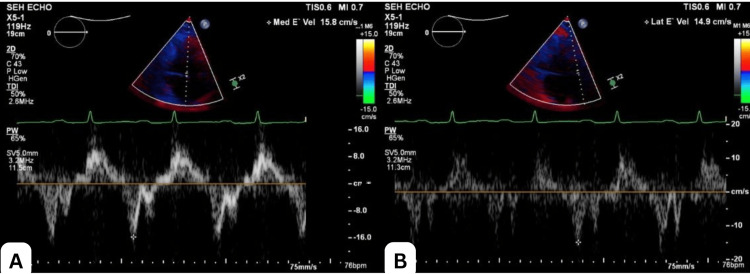 Figure 4
Figure 4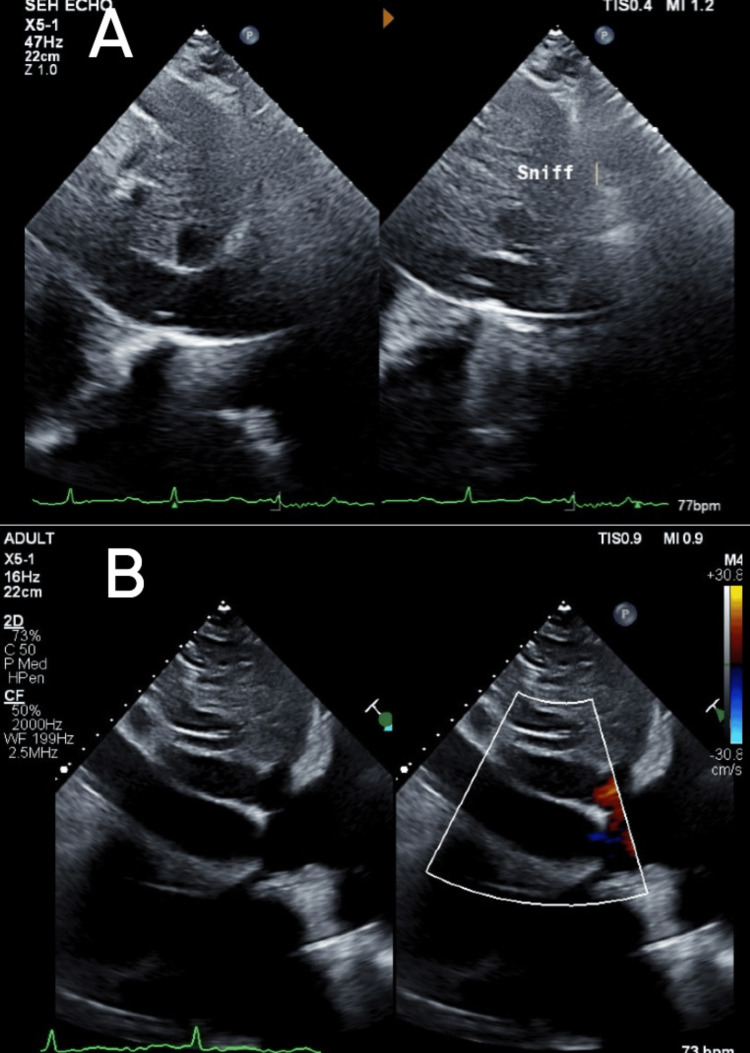 Figure 5
Figure 5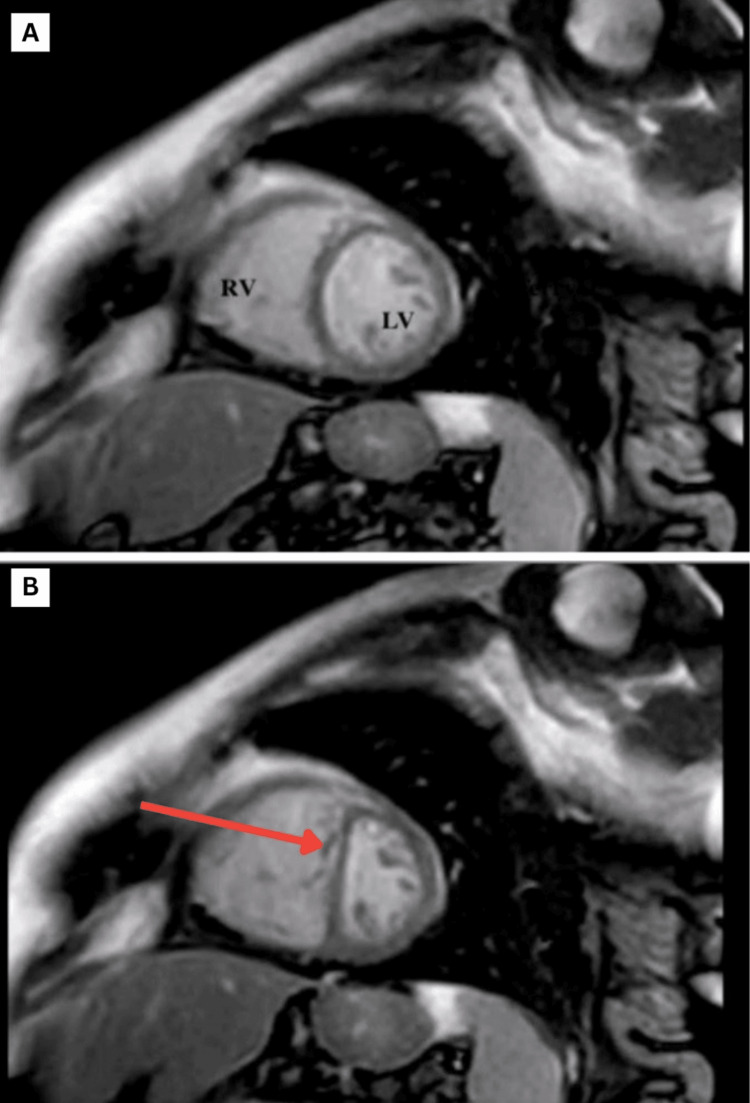 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Cardiac tumors and thrombi · Eosinophilic Disorders and Syndromes
Introduction
Constrictive pericarditis (CP) is a rare diagnosis with an estimated prevalence of 0.2%-0.4% among patients who have undergone cardiac surgery or experienced pericardial trauma or inflammation [1]. It is a reversible condition in which granulation tissue forms either from chronic inflammation or fibrosis within the pericardium, resulting in a loss of pericardial elasticity and restricted ventricular filling, ultimately leading to diastolic heart failure. The types of CP are transient/subacute (weeks to months, potentially reversible), chronic (months to years, irreversible), and occult (clinically silent until provoked). The risk of developing constrictive pericarditis is highest following purulent or tuberculous pericarditis and much lower after idiopathic or viral pericarditis (<0.5%) [2,3]. Post-surgical and post-radiation cases are increasingly recognized due to advances in cardiac interventions and cancer therapies [4-6]. CP can also mimic heart failure with preserved ejection fraction (HFpEF), often presenting with symptoms of right-sided heart failure. It is frequently misdiagnosed, underscoring the importance of expert evaluation and the use of multimodality imaging.
This article was previously presented as a poster presentation at the 74^th^ Annual Scientific Session of the American College of Cardiology on March 31, 2025. Written informed consent for publication of this case report and all accompanying images was obtained from the patient.
Case presentation
A 66-year-old female patient with a history of seropositive rheumatoid arthritis (RA) and hypertension presented with exertional dyspnea, orthopnea, and lower limb swelling for one and a half months. She denied chest pain, recent viral illness, or prior history of tuberculosis, radiation, or surgery. On presentation, her vital signs were stable (blood pressure (BP): 133/80 mmHg, heart rate (HR): 76 beats per minute (bpm), SpO₂: 96% on room air). A physical exam revealed bilateral pitting edema of the lower extremities and abdominal distension consistent with moderate ascites; chest examination was unremarkable.
The electrocardiogram showed sinus rhythm with low-voltage QRS complexes and nonspecific ST-T wave changes (Figure 1).
An electrocardiogram showed sinus rhythm, low voltage amplitude with nonspecific ST and T wave changes.
Chest X-ray didn’t reveal any signs of constrictive pericarditis, but computed tomography (CT) performed 36 hours after presentation showed extensive pericardial calcification, most prominent along the lateral wall of the right ventricle, with mild pericardial thickening/effusion (maximum thickness: 7 mm; Figure 2).
Computed tomography of the chest showing extensive pericardial calcification, most severe along the right ventricular lateral wall, with small pericardial thickening/effusion with a maximum thickness of 7 mm.
Laboratory evaluation showed a mildly elevated B-type natriuretic peptide (BNP) level of 225 pg/mL (reference range: 0-100 pg/mL); inflammatory markers were unremarkable; and a transthoracic echocardiogram (TTE) performed by a cardiologist revealed trivial pericardial effusion with preserved left ventricular volume and function (Figure 3), along with an elevated right ventricular systolic pressure (RVSP) of 46 mmHg.
Transthoracic echocardiography showed preserved ejection fraction with mitral E/A ratio of 1.7 (greater than 1.5).
She was subsequently diagnosed with HFpEF of 55%-60% and was discharged on diuretics, mineralocorticoid receptor antagonists, and sodium glucose co-transporter (SGLT) 2 inhibitors. Over the next 18 months, she experienced multiple hospitalizations for episodes of acute exacerbation of HFpEF, despite compliance with optimal medical therapy, and was noted to have progressively worsening fluid retention.
A repeat TTE revealed ventricular septal bounce, which is a dynamic echocardiographic finding characterized by abnormal, rapid, and exaggerated motion of the interventricular septum during early diastole, often with a brief posterior and then anterior movement (Video 1); a plethoric inferior vena cava with reduced respiratory collapse (Figure 4); and a positive annulus reversus sign characterized by a reversal of the normal relationship between early diastolic mitral annular velocities: the medial (septal) e′ velocity exceeds the lateral e′ velocity. Normally, the lateral e′ is higher than the medial e′, but in constrictive pericarditis, pericardial tethering of the lateral annulus leads to a reduced lateral e′, while the medial e′ remains preserved or is even increased (Figure 5), suggestive of CP. A review of the previous TTE revealed that the septal bounce had been missed. Hepatic vein flow and respiratory cycle monitoring had not been performed at that time. Right heart catheterization showed mildly elevated pulmonary artery pressure (29 mmHg). Cardiac magnetic resonance imaging (MRI) revealed pericardial thickening, septal bounce, interventricular dependence, and biatrial dilation (Figure 6), confirming the diagnosis of CP.
Repeat transthoracic echocardiography revealed ventricular septal bounce in early diastole.
Transthoracic echocardiography (TTE) shows mitral ‘annulus reversus,’ as evidenced by mitral velocity e’ velocity >2% and higher than lateral e’ velocity, which was missed during initial TTE evaluation, the reason being preserved lateral e’ velocity. Figure A shows medial e' velocity of 15.8 cm/s, and Figure B shows lateral e' velocity of 14.9 cm/s.
Transthoracic echocardiography in respirophasic cycle.Figure A shows reduced collapsibility of the inferior vena cava (IVC; 2.76 cm) on inspiration. Normally, it's collapsible in inspiration. Normal IVC diameter is 2.9 cm here. Figure B shows a plethoric IVC during inspiration.
Cardiac magnetic resonance imaging (MRI)Figure A shows a normal interventricular septum in diastole. Figure B shows a leftward shift towards the ventricle known as septal bounce or flattening in inspiration.
She was referred to a higher center for pericardiectomy per her preference. She underwent pericardiectomy and was discharged in stable condition with oral diuretics, SGLT2 inhibitors, and a mineralocorticoid receptor antagonist. On follow-up, the patient reported significantly improved symptoms. Follow-up at six months post-pericardiectomy showed sustained symptomatic improvement to New York Heart Association (NYHA) class I and normalization of right-sided pressures on echocardiography; N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels fell from 1200 to 210 pg/mL.
Discussion
CP is a rare condition with a prevalence likely underestimated due to frequent misdiagnosis. Globally, tuberculosis remains the leading cause; however, in developed countries, CP is typically idiopathic or secondary to previous viral infections, cardiac surgery, or radiation. While pericarditis can occur in up to 20% of patients with systemic lupus erythematosus, and 30%-50% of RA patients may have asymptomatic pericardial effusions, progression to constrictive physiology is rare, which was presumed to be the etiology for chronic CP in the presented case [7,8]. Clinical manifestations commonly align with those of right-sided heart failure, including elevated jugular venous pressure, ascites, peripheral edema, Kussmaul’s sign, and a pericardial knock. Consequently, CP may clinically overlap with conditions such as restrictive cardiomyopathy, severe tricuspid regurgitation, cirrhosis, or chronic obstructive pulmonary disease (COPD) with cor pulmonale. In contrast to cardiomyopathies like restrictive cardiomyopathy, BNP levels in CP are typically normal or only mildly elevated, as observed in this case [9]. Additionally, inflammatory markers such as ESR and CRP may be elevated, particularly in autoimmune-related CP.
Echocardiography is the initial imaging modality for diagnosing constrictive pericarditis (CP), and the diagnosis is established based on the Mayo Clinic Diagnostic Criteria, which include respirophasic septal motion bounce, respiratory variation in mitral E velocity (>25%), medial mitral e′ velocity ≥9 cm/s, medial-to-lateral e′ ratio ≥0.91, and hepatic vein expiratory diastolic reversal ratio ≥79% [10]. In our case, medial e′ was 15.8 cm/s, lateral e′ was 14.9 cm/s, and septal bounce was evident, consistent with CP. Although 93% of septal bounce occurrences are associated with CP, the specificity remains low, as septal bounce may also be observed in left bundle branch block (LBBB), right ventricular pacing, cardiac tamponade, or pulmonary hypertension [10].
Multimodality imaging, including CT and cardiac MRI, is often critical for further evaluation of suspected cases. Cardiac MRI has a 93% sensitivity for detecting pericardial thickening greater than 4 mm [11]. However, the absence of thickening does not exclude CP, as some patients may present with constriction without radiographic evidence [12,13]. Cardiac catheterization remains the gold standard diagnostic approach, particularly when noninvasive evaluations are inconclusive. Diagnostic hemodynamic findings for CP include [14,15]: Equalization of right and left ventricular end-diastolic pressures (within 5 mmHg), rapid early diastolic filling with a "dip-and-plateau" or "square root" sign, interventricular dependence (discordant respiratory changes in RV and LV systolic pressures), and dissociation between intrathoracic and intracardiac pressures during respiration.
According to the ACC/American Heart Association (AHA) guidelines, radical (complete) pericardiectomy remains the mainstay of treatment for patients with constrictive pericarditis, particularly those with non-inflammatory disease or those who do not respond to anti-inflammatory therapy for inflammatory pericarditis. In patients with evidence of active inflammation, reflected by elevated inflammatory markers such as ESR or CRP or by cardiac MRI findings (pericardial calcification or absence of active inflammation), an initial trial of anti-inflammatory therapy is recommended for several weeks, with close monitoring for clinical improvement. Postoperatively, patients with idiopathic or viral pericarditis generally have more favorable outcomes. Conversely, individuals with comorbid conditions such as advanced age, renal dysfunction, pulmonary hypertension, or prior radiation exposure, as well as those with underlying systemic inflammatory disease or significant myocardial involvement, tend to experience poorer prognoses [16,17]. Diuretics may also aid in symptomatic management; however, they don't have any mortality benefit. If misdiagnosed or untreated, CP carries a mortality rate exceeding 90% [18]. This case emphasizes the diagnostic challenge posed by CP, particularly given its nonspecific clinical presentation that can closely resemble HFpEF. The unusual association with rheumatoid arthritis further complicates recognition. Clinicians should maintain a high index of suspicion for CP in patients with diuretic-refractory HFpEF phenotypes. Comprehensive echocardiographic assessment, including respiratory variation in transvalvular flows and hepatic vein Doppler analysis, should be pursued early. Integration of multimodal imaging and invasive hemodynamic evaluation via catheterization is essential for definitive diagnosis and timely therapeutic intervention.
Conclusions
CP is a rare but potentially reversible cause of diastolic heart failure, characterized by pericardial fibrosis and calcification that impair ventricular filling. Advances in imaging, particularly cardiac MRI and hemodynamic assessment via catheterization, have significantly improved diagnostic accuracy, especially in differentiating constriction from restrictive cardiomyopathy. While medical management may offer temporary symptomatic relief in selected inflammatory cases, definitive treatment lies in surgical pericardiectomy, which, when performed timely, is associated with favorable long-term survival and functional recovery. Early recognition and multidisciplinary evaluation are critical to improving patient prognosis and preventing irreversible myocardial damage.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Constrictive pericarditis: a practical clinical approach Prog Cardiovasc Dis Miranda WR Oh JK 3693795920172806226710.1016/j.pcad.2016.12.008 · doi ↗ · pubmed ↗
- 2American Society of Echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease: endorsed by the Society for Cardiovascular Magnetic Resonance and Society of Cardiovascular Computed Tomography J Am Soc Echocardiogr Klein AL Abbara S Agler DA 9651012262013 https://doi.org/10.1016/j.echo.2013.06.0232399869310.1016/j.echo.2013.06.023 · doi ↗ · pubmed ↗
- 3Evaluation and treatment of pericarditis: a systematic review JAMA Imazio M Gaita F Le Winter M 1498150631420152646199810.1001/jama.2015.12763 · doi ↗ · pubmed ↗
- 4Risk of constrictive pericarditis after acute pericarditis Circulation Imazio M Brucato A Maestroni S Cumetti D Belli R Trinchero R Adler Y 1270127512420112184407710.1161/CIRCULATIONAHA.111.018580 · doi ↗ · pubmed ↗
- 5Constrictive pericarditis: diagnosis, management and clinical outcomes Heart Welch TD 72573110420182917597810.1136/heartjnl-2017-311683 · doi ↗ · pubmed ↗
- 6Constrictive pericarditis Circ J Sengupta PP Eleid MF Khandheria BK 155515627220081876270610.1253/circj.cj-08-0654 · doi ↗ · pubmed ↗
- 7Correction to: current diagnostic and treatment strategies for specific dilated cardiomyopathies: a scientific statement from the American Heart Association Circulation 0134201610.1161/CIR.000000000000045527832612 · doi ↗ · pubmed ↗
- 8Diagnosis, risk stratification, and treatment of pericarditis: a review JAMA Cremer PC Klein AL Imazio M 1090110033220243923577110.1001/jama.2024.12935 · doi ↗ · pubmed ↗