Leptospirosis Prevalence and Risk Factors Among Patients Presenting With Fever to 4 Healthcare Sites in Sub-Saharan Africa and South East Asia: An International Multisite Observational and Nested Case–Control Study
John A Crump, Polycarp Mogeni, Sara A Ajanovic, Justina M Bramugy, Mabvuto Chimenya, Edward W Green, Sham Lal, David C W Mabey, Mayfong Mayxay, Paul N Newton, Ioana D Olaru, Heidi Hopkins, Mathieu Picardeau, Benjamin Amos, Benjamin Amos, Elizabeth A Ashley, Oliver Baerenbold

TL;DR
Leptospirosis was found among febrile patients in four countries, with risk factors including rice field work and river water exposure.
Contribution
This is the first international multisite study on leptospirosis prevalence and risk factors in sub-Saharan Africa and South East Asia.
Findings
Leptospirosis prevalence ranged from 0.3% to 4.6% across four countries.
Rice field work and river water consumption were significant risk factors.
Leptospira borgpetersenii, L. interrogans, and L. kirschneri were identified as causative species.
Abstract
We investigated the prevalence, diversity, and risk factors for acute leptospirosis in the Febrile Illness Evaluation in a Broad Range of Endemicities (FIEBRE) study. Febrile patients aged ≥2 months in Laos, Malawi, Mozambique, and Zimbabwe underwent a standardized clinical and exposure assessment. Acute and convalescent serum were tested by Leptospira microscopic agglutination test (MAT) and acute plasma by lfb1 polymerase chain reaction. A ≥4-fold rise in antibody titer, or a single reciprocal titer ≥800, or Leptospira PCR positive defined confirmed leptospirosis. The identity of possible infecting strains was investigated by MAT and sequencing of PCR products. Of 7851 febrile participants enrolled, 134 (1.7%) had confirmed leptospirosis: 88 (4.6%) in Laos, 17 (1.0%) Malawi, 7 (0.3%) Mozambique, and 22 (1.2%) Zimbabwe, and 23 (0.8%) had supportive evidence of leptospirosis.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
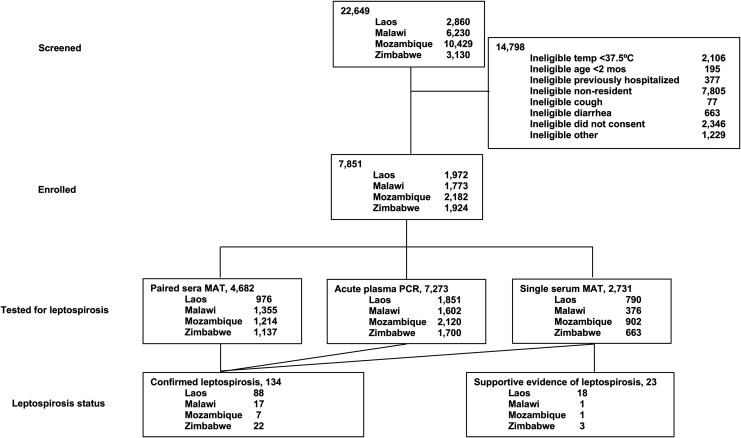 Figure 1
Figure 1| Site | Species | N Positive Age <15 y | N Positive Age ≥15 y | N Positive All Ages |
|---|---|---|---|---|
| Laos |
| 3 | 10 | 13 |
|
| 0 | 1 | 1 | |
| Malawi |
| 0 | 1 | 1 |
|
| 2 | 3 | 5 | |
| Mozambique |
| 2 | 0 | 2 |
|
| 0 | 4 | 4 | |
| Zimbabwe |
| 0 | 2 | 2 |
|
| 6 | 4 | 10 | |
| Overall |
| 0 | 3 | 3 |
|
| 13 | 17 | 30 | |
|
| 0 | 5 | 5 |
| Age Group, y | ≥4-Fold Rise In | Single |
| Total Confirmed Leptospirosis | Single Reciprocal Titer ≥200 But <800 | Total Confirmed or Supportive Evidence of Leptospirosis | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | n | (%) | N | n | (%) | N | n | (%) | N | n | (%) | N | n | (%) | N | n | (%) | ||
| Laos | <15 | 241 | 9 | (3.73) | 352 | 5 | (1.42) | 654 | 3 | (0.46) | 717 | 16 | (2.23) | 352 | 5 | (1.42) | 717 | 21 | (2.93) |
| ≥15 | 735 | 59 | (8.03) | 438 | 4 | (0.90) | 1197 | 11 | (0.92) | 1206 | 72 | (5.97) | 438 | 13 | (2.97) | 1206 | 85 | (7.05) | |
| All ages | 976 | 68 | (6.97) | 790 | 9 | (1.14) | 1851 | 14 | (0.76) | 1923 | 88 | (4.58) | 790 | 18 | (2.28) | 1923 | 106 | (5.51) | |
| Malawi | <15 | 674 | 2 | (0.30) | 244 | 1 | (0.41) | 863 | 2 | (0.23) | 930 | 5 | (0.54) | 244 | 0 | (0.00) | 1020 | 5 | (0.49) |
| ≥15 | 681 | 8 | (1.17) | 132 | 0 | (0.00) | 739 | 4 | (0.54) | 819 | 12 | (0.54) | 132 | 1 | (0.76) | 819 | 13 | (1.59) | |
| All ages | 1355 | 10 | (0.74) | 376 | 1 | (0.27) | 1602 | 6 | (0.37) | 1749 | 17 | (1.47) | 376 | 1 | (0.27) | 1749 | 18 | (1.03) | |
| Mozambique | <15 | 561 | 0 | (0.00) | 546 | 0 | (0.00) | 1122 | 2 | (0.18) | 1157 | 2 | (0.17) | 546 | 0 | (0.00) | 1157 | 2 | (0.17) |
| ≥15 | 653 | 2 | (0.31) | 356 | 0 | (0.00) | 998 | 4 | (0.40) | 1016 | 5 | (0.49) | 356 | 1 | (0.28) | 1016 | 6 | (0.59) | |
| All ages | 1214 | 2 | (0.16) | 902 | 0 | (0.00) | 2120 | 6 | (0.28) | 2173 | 7 | (0.32) | 902 | 1 | (0.11) | 2173 | 8 | (0.37) | |
| Zimbabwe | <15 | 408 | 1 | (0.25) | 372 | 1 | (0.27) | 703 | 6 | (0.85) | 828 | 8 | (0.97) | 372 | 1 | (0.27) | 828 | 9 | (1.09) |
| ≥15 | 729 | 8 | (1.10) | 291 | 2 | (0.69) | 997 | 6 | (0.60) | 1036 | 14 | (1.35) | 291 | 2 | (0.69) | 1036 | 16 | (1.54) | |
| All ages | 1137 | 9 | (0.79) | 663 | 3 | (0.45) | 1700 | 12 | (0.71) | 1864 | 22 | (1.18) | 663 | 3 | (0.45) | 1864 | 25 | (1.34) | |
| Total | <15 | 1844 | 12 | (0.64) | 1514 | 7 | (0.46) | 3342 | 13 | (0.39) | 3632 | 31 | (0.85) | 1514 | 6 | (0.40) | 3632 | 37 | (1.02) |
| ≥15 | 2798 | 77 | (2.75) | 1217 | 6 | (0.49) | 3931 | 25 | (0.64) | 4077 | 103 | (2.53) | 1217 | 17 | (1.40) | 4077 | 120 | (2.94) | |
| All ages | 4682 | 89 | (1.90) | 2731 | 13 | (0.48) | 7273 | 38 | (0.52) | 7709 | 134 | (1.75) | 2731 | 23 | (0.84) | 7709 | 157 | (2.04) | |
| Confirmed or Supportive N = 157 | Neither N = 7551 | Unadjusted Model | Adjusted Model** | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | OR | 95% CI |
| aOR | 95% CI |
| |
| Sex | ||||||||||
| Female | 75 | (47.8) | 3993 | (52.9) | Ref. | Ref. | … | … | ||
| Male | 82 | (52.2) | 3558 | (47.1) | 1.23 | (.89,1.68) | .205 | 1.33 | (.75, 2.38) | .332 |
| Age years, median (IQR) | 27.0 | (17.0–43.0) | 18.0 | (4.7–33.0) | 1.02 | (1.01, 1.03) | <.001 | 1.01 | (1.00, 1.02) | .107 |
| Health facility admission status | ||||||||||
| Outpatient | 80 | (51.0) | 4320 | (57.2) | Ref. | … | Ref. | … | … | |
| Inpatient | 77 | (49.0) | 3232 | (42.8) | 1.29 | (.94, 1.76) | .118 | 1.43 | (.75, 2.74) | .278 |
| Admission temperature °C, median (IQR) | 38.0 | (37.6–38.5) | 38.1 | (37.7–38.9) | 0.77 | (.61, .97) | .026 | … | … | … |
| Systolic blood pressure mmHg, median (IQR) | 110.0 | (100.0–120.0) | 110.0 | (97.0–120.0) | 1.00 | (1.00, 1.00) | .990 | … | … | … |
| Diastolic blood pressure mmHg, median (IQR) | 70.0 | (60.0–80.0) | 70.0 | (60.0–79.0) | 0.99 | (.98, 1.01) | .384 | … | … | … |
| O2 saturation %, median (IQR) | 96.0 | (95.0–98.0) | 97.0 | (95.0–98.0) | 0.97 | (.94, .99) | .008 | … | … | … |
| Respiratory rate per minute, median (IQR) | 22.0 | (20.0–25.0) | 22.0 | (20.0–28.0) | 0.96 | (.93, .98) | .001 | … | … | … |
| Diarrhea | ||||||||||
| No | 33 | (89.2) | 3290 | (91.8) | Ref. | … | … | … | … | |
| Yes | 4 | (10.8) | 292 | (8.2) | 1.37 | (.48, 3.88) | .559 | … | … | … |
| History of fever days, median (IQR) | 3.0 | (2.0–4.0) | 2.0 | (2.0–4.0) | 1.00 | (.97, 1.04) | .914 | … | … | … |
| Cough | ||||||||||
| No | 108 | (68.8) | 4847 | (64.7) | Ref. | … | … | … | … | |
| Yes | 49 | (31.2) | 2639 | (35.3) | 0.83 | (.59, 1.17) | .294 | … | … | … |
| Vomit | ||||||||||
| No | 128 | (81.5) | 6372 | (85.1) | … | … | … | … | … | |
| Yes | 29 | (18.5) | 1115 | (14.9) | 1.29 | (.86, 1.95) | .215 | … | … | … |
| Headache | ||||||||||
| No | 31 | (21.4) | 1765 | (33.9) | Ref. | … | Ref. | … | … | |
| Yes | 114 | (78.6) | 3440 | (66.1) | 1.89 | (1.26, 2.82) | .002 | 2.20 | (1.79, 2.70) | <.001 |
| Musculoskeletal pain | ||||||||||
| No | 59 | (49.2) | 1995 | (51.4) | Ref. | … | … | … | … | |
| Yes | 61 | (50.8) | 1890 | (48.6) | 1.09 | (.76, 1.57) | .637 | … | … | … |
| Abdominal pain | ||||||||||
| No | 118 | (75.6) | 5588 | (76.6) | Ref. | … | … | … | … | |
| Yes | 38 | (24.4) | 1708 | (23.4) | 1.05 | (.73, 1.52) | .782 | … | … | … |
| Rash or skin lesions | ||||||||||
| No | 144 | (91.7) | 7072 | (94.0) | Ref. | … | Ref. | … | … | |
| Yes | 13 | (8.2) | 449 | (6.0) | 1.42 | (.80, 2.53) | .231 | 1.45 | (1.16, 1.82) | .001 |
| Skin blanching | ||||||||||
| No | 13 | (100.0) | 430 | (96.6) | Ref. | … | … | … | … | |
| Yes | 0 | (0.0) | 15 | (3.4) | 1.00 | … | … | … | … | |
| Conjunctivitis | ||||||||||
| No | 153 | (97.5) | 7462 | (99.2) | Ref. | … | Ref. | … | … | |
| Yes | 4 | (2.5) | 57 | (0.8) | 3.42 | (1.23, 9.55) | .019 | 3.33 | (2.55, 4.36) | <.001 |
| Jaundice | ||||||||||
| No | 147 | (93.6) | 7329 | (97.4) | Ref. | … | Ref. | … | … | |
| Yes | 10 | (6.4) | 195 | (2.6) | 2.56 | (1.33, 4.93) | .005 | 1.75 | (1.39, 2.19) | <.001 |
| Pediatric Early Warning Score, median (IQR) | 14.0 | (10.0–20.0) | 11.0 | (7.0–18.0) | 1.01 | (.98, 1.05) | .512 | … | … | … |
| Universal Vital Assessment Score, median (IQR) | 0.0 | (0.0–0.0) | 0.0 | (0.0–2.0) | 0.65 | (.52, .81) | <.001 | … | … | … |
| Logistic Organ Dysfunction Score, median (IQR) | 0.0 | (0.0–0.0) | 0.0 | (0.0–0.0) | 0.53 | (.13, 2.08) | .361 | … | … | … |
| Antimalarials administered | ||||||||||
| No | 153 | (98.1) | 6463 | (86.8) | Ref. | … | Ref. | … | … | |
| Yes | 3 | (1.9) | 980 | (13.2) | 0.13 | (.04, .41) | <.001 | 0.10 | (.02, .44) | .002 |
| Any antimicrobial administered | ||||||||||
| No | 10 | (76.9) | 751 | (88.2) | Ref. | … | … | … | … | |
| Yes | 3 | (23.1) | 100 | (11.8) | 2.25 | (.61, 8.32) | .223 | … | … | … |
| Died by day 28 | ||||||||||
| No | 136 | (88.9) | 6293 | (85.8) | Ref. | … | … | … | … | |
| Yes | 5 | (3.3) | 266 | (3.6) | 0.87 | (.35, 2.14) | .761 | … | … | … |
| Lost to follow-up | 12 | (7.8) | 779 | (10.6) | 0.71 | (.39, 1.29) | .265 | … | … | … |
| Died in hospital | ||||||||||
| No | 149 | (94.9) | 7279 | (96.4) | Ref. | … | … | … | … | |
| Yes | 2 | (1.3) | 98 | (1.3) | 1.00 | (.24, 4.08) | .997 | … | … | … |
| Referred | 6 | (3.8) | 175 | (2.3) | 1.67 | (.73, 3.84) | .223 | … | … | … |
| Confirmed Or Supportive N = 157 | Neither N = 7551 | Unadjusted Model | Adjusted Model** | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | OR | 95% CI |
| aOR | 95% CI |
| |
| Sex | ||||||||||
| Female | 75 | (47.8) | 3993 | (52.9) | Ref. | … | Ref. | … | … | |
| Male | 82 | (52.2) | 3558 | (47.1) | 1.23 | (.89, 1.68) | .205 | 1.09 | (.61, 1.94) | .772 |
| Age years, median (IQR) | 26.5 | (17.0–43.0) | 18.0 | (4.7–33.0) | 1.02 | (1.01, 1.03) | <.001 | 1.02 | (1.01, 1.02) | <.001 |
| Lived or worked in close contact with cattle in the past month | ||||||||||
| No | 137 | (87.8) | 7048 | (94.1) | … | … | … | … | … | |
| Yes | 19 | (12.2) | 439 | (5.9) | 2.23 | (1.36, 3.63) | .001 | … | … | … |
| Lived or worked in close contact with goats in the past month | ||||||||||
| No | 153 | (97.5) | 7105 | (94.8) | Ref. | … | … | … | … | |
| Yes | 4 | (2.5) | 391 | (5.2) | 0.48 | (.18, 1.29) | .144 | … | … | … |
| Lived or worked in close contact with pigs in the past month | ||||||||||
| No | 149 | (94.9) | 7291 | (97.2) | … | … | … | … | … | |
| Yes | 8 | (5.1) | 207 | (2.8) | 1.89 | (.92, 3.90) | .085 | … | … | … |
| Lived or worked in close contact with cattle, goats, or pigs in the past month | ||||||||||
| No | 132 | (84.6) | 6710 | (89.7) | Ref. | … | … | … | … | |
| Yes | 24 | (15.4) | 769 | (10.3) | 1.59 | (1.02, 2.47) | .040 | … | … | … |
| Waded, swum or bathed in pond water, lake water, or stream water in the past month | ||||||||||
| No | 113 | (72.0) | 6822 | (91.1) | Ref. | … | … | … | … | |
| Yes | 44 | (28.0) | 667 | (8.9) | 3.98 | (2.79, 5.69) | <.001 | … | … | … |
| Worked in rice fields in the past month | ||||||||||
| No | 96 | (61.1) | 6903 | (92.2) | Ref. | … | Ref. | … | … | |
| Yes | 61 | (38.9) | 580 | (7.8) | 7.56 | (5.43, 10.54) | <.001 | 6.24 | (3.25, 11.98) | <.001 |
| Source of drinking water in the dry season: river | ||||||||||
| No | 154 | (98.1) | 7489 | (99.7) | Ref. | … | Ref. | … | … | |
| Yes | 3 | (1.9) | 21 | (0.3) | 6.95 | (2.05, 23.54) | .002 | 5.11 | (2.00, 13.09) | .001 |
| Source of drinking water in the dry season: pond | ||||||||||
| No | 157 | (100.0) | 7508 | (100.0) | Ref. | … | … | … | … | |
| Yes | 0 | (0.0) | 2 | (<0.1) | 1.00 | … | … | … | … | |
| Source of drinking water in the dry season: river or pond | ||||||||||
| No | 154 | (98.1) | 7487 | (99.7) | Ref. | … | … | … | … | |
| Yes | 3 | (1.9) | 23 | (0.3) | 6.34 | (1.88, 21.34) | .003 | … | … | … |
| Site | Serogroup | N Positive | Acute Titer Range | Convalescent Titer Range | Median Titer | Potential Regional Reservoirs |
|---|---|---|---|---|---|---|
| Laos | Australis | 19 | 0–200 | 200–12 800 | 400 | Cattle, rat, dog, pig, horse, nutria, toad |
| Sejroe | 17 | 0–200 | 200–3200 | 400 | Cattle, dog, rat, vole | |
| Bataviae | 14 | 0–200 | 200–1600 | 400 | Rat, frog, cat | |
| Icterohemorrhagiae | 12 | 0–200 | 200–6400 | 800 | Rat, cattle, dog, pig, vole, civet, raccoon, mouse | |
| Grippotyphosa | 9 | 0–0 | 200–1600 | 200 | Rat, frog, cattle, dog, flying squirrel, goat, mouse, hedgehog, sheep, tick from cattle | |
| Autumnalis | 3 | 0–0 | 800–1600 | 1600 | Rat, cattle, dog, toad, hedgehog, pig | |
| Celledoni | 3 | 0–0 | 400–12 800 | 800 | Rat | |
| Pomona | 2 | 0–0 | 400–800 | 600 | Civet, cattle, mouse, mongoose, cat, dog, pig, rat, squirrel, fox | |
| Hebdomadis | 1 | 0–0 | 200 | 200 | Cattle, mouse, rat, raccoon, vole | |
| Malawi | Icterohemorrhagiae | 5 | 0–0 | 200–6400 | 200 | Rat, cattle, mongoose, fox |
| Sejroe | 2 | 0–0 | 400–6400 | 3400 | Rat, cattle | |
| Australis | 1 | 0–0 | 6400 | 6400 | Rat, cattle | |
| Mini | 1 | 0–0 | 200 | 200 | None | |
| Pyrogenes | 1 | 0–0 | 200 | 200 | Rat, cattle | |
| Mozambique | Australis | 2 | 0–0 | 200–200 | 200 | Rat, cattle |
| Autumnalis | 1 | 0–0 | 200 | 200 | Rat | |
| Icterohemorrhagiae | 1 | 0–0 | 200 | 200 | Rat, cattle, mongoose, fox | |
| Zimbabwe | Ballum | 6 | 0–0 | 200–6400 | 300 | Rat, mouse |
| Icterohemorrhagiae | 3 | 0–0 | 200–800 | 400 | Rat, cattle, mongoose, fox | |
| Pomona | 1 | 0–0 | 200 | 200 | Cattle | |
| Pyrogenes | 1 | 0–0 | 200 | 200 | Rat, cattle |
- —UK government
- —Wellcome Trust10.13039/100010269
- —Wellcome Trust Clinical PhD Programme
- —London School of Hygiene and Tropical Medicine10.13039/100009660
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLeptospirosis research and findings
Leptospirosis is a zoonotic bacterial infection established as a major cause of fever in Asia [1] and increasingly recognized as an important cause of fever in Africa [2, 3]. Leptospirosis commonly presents as a febrile illness in humans that is difficult to distinguish clinically from other causes of fever and may be severe and fatal [4]. Reference standard laboratory diagnosis relies on microscopic agglutination testing (MAT) of paired sera, nucleic acid amplification tests, and bacterial isolation rarely available in low-resource endemic areas [5]. Leptospira includes diverse pathogenic and intermediate pathogenic strains capable of causing human illness across a wide range of Leptospira species, serogroups, and serovars. Nonhuman animals are the reservoirs of Leptospira spp. associated with human illness. Infected animals may remain well or experience a range of clinical manifestations from infertility, abortion, and poor milk yield, and become carriers, continuing to excrete Leptospira in their urine, in turn contaminating water and moist soil [5]. Humans are infected following direct contact with the urine of animals shedding Leptospira or indirectly by contacted with urine-contaminated environments [6]. The organism enters the human host via mucous membranes and broken skin. Leptospira have a complex and diverse ecology with variation in dominant host species by location and over time. Rodents are recognized as major reservoirs of Leptospira worldwide [5] and activities exposing persons to rodent urine, including residence in an urban slum, proximity to open sewers, exposure to floodwaters, and rice paddy work, are associated with increased risk for disease [5–7]. Risk factors for leptospirosis are less well understood in mainland Africa than elsewhere. While rodents are likely to be important hosts, cattle exposure was associated with increased odds for disease at some locations [8–11].
The lack of widespread access to reference diagnostic tests for leptospirosis, their complexity, and the limited investment in leptospirosis as a neglected tropical zoonosis mean that our understanding of its role as a cause of febrile illness and associated risk factors is incomplete [12, 13]. The Febrile Illness Evaluation in a Broad Range of Endemicities (FIEBRE) study [14] sought to describe treatable and preventable causes of febrile illness among inpatients and outpatients at multiple sites with little or no data on leptospirosis and other causes of fever using reference standard diagnostics.
To provide insights into variation in the role of acute leptospirosis as a cause of febrile illness, the diversity of infecting Leptospira species and serogroups, clinical features, clinical diagnosis, behaviors, and exposures associated with disease, we undertook a secondary analysis of FIEBRE data focused on participants with and without leptospirosis. We extended this work by examining the predominant reactive Leptospira serogroups associated with human illness in FIEBRE sites and their potential hosts.
METHODS
The overall design of FIEBRE has been described in detail elsewhere [14]. A brief summary is provided below, including detailed methods for the present analysis.
Study Sites
FIEBRE was conducted at 4 sites: Vientiane Provincial Hospital, Phonghong, Lao People's Democratic Republic (Laos); Chikwawa District Hospital, Malawi; Manhiça District Hospital and General Macamo Hospital, Maputo, Mozambique; and Sally Mugabe Central Hospital, Parirenyatwa Hospital, Chitungwiza General Hospital, and 3 primary care clinics in Harare, Zimbabwe.
Enrollment, Follow-up, Data Collection, and Sample Collection for Febrile Participants
Febrile outpatients and inpatients aged ≥2 months were eligible for enrollment if they had a tympanic or axillary temperature of ≥37.5°C at presentation and had not been hospitalized or undergone surgery in the previous month. Outpatients were eligible if they were residents within a defined catchment area around the health facility at the time of enrollment. For outpatients aged ≥15 years, those without symptoms of either lower respiratory infection or diarrheal disease were eligible. For outpatients aged ≥2 months to <15 years, those without symptoms of diarrheal disease were eligible. After provision of informed consent, demographic information and a standardized clinical and exposure history were taken, and physical examination was performed on all participants and recorded on a case report form (Supplementary Appendix). The exposure history included questions relevant to risk for leptospirosis, such as exposure to surface water, rice fields, and animals, including livestock.
Whole blood and ethylenediaminetetraacetic acid (EDTA) blood were collected on day 0, and participants were asked to return 28 days after enrollment (acceptable range: 26–48 days) for collection of convalescent whole blood. Serum and plasma were separated, aliquoted, and stored at −70°C. Samples were shipped on dry ice to the London School of Hygiene and Tropical Medicine, London, United Kingdom, for distribution on dry ice to reference laboratories.
Laboratory Methods
Leptospira Serology
At the Unité Biologie des Spirochètes, French National Reference Center for Leptospirosis, WHO Collaborating Centre for Reference and Research on Leptospirosis, Institut Pasteur, Paris, France, acute and convalescent serum was first screened by Leptospira fainei serovar Hurstbridge IgM enzyme-linked immunosorbent assay (ELISA) [15]. Serum of participants screening positive by ELISA on the acute or convalescent sample proceeded to testing with the Leptospira standard MAT. The MAT panels were based on the World Health Organization recommended list of globally representative reference Leptospira strains [16] adjusted to incorporate African and Asian regional isolates (Supplementary Appendix).
Leptospira Nucleic Acid Amplification Testing and Speciation
Acute plasma collected in EDTA from all participants was tested by polymerase chain reaction (PCR) to the lfb1 pathogenic Leptospira target [17]. Among samples positive by Leptospira lfb1 PCR, PCR products were sequenced for Leptospira speciation [18, 19].
Study Definitions
For the purpose of this analysis and consistent with widely accepted case definitions [20], we defined confirmed acute leptospirosis as a participant with ≥4-fold rise in antibody titer between acute and convalescent sample or a single reciprocal titer ≥800, or Leptospira PCR positive for the lfb1 gene target. We defined supportive evidence of leptospirosis as a participant with a single reciprocal titer ≥200 but <800. The predominant reactive serogroup was defined as the serogroup for the reacting serovar with the highest MAT titer.
Potential Host Animal Species of Leptospira
To generate hypotheses about potential host animals of Leptospira by site, we interrogated the Dr Leopold Kirschner database of Leptospira species and serovar isolations and detections from animals worldwide at the serogroup level [21, 22]. We did this for leading predominant reactive Leptospira serogroups by study site for participants with serologically confirmed leptospirosis at the level of country and United Nations region.
Sample Size
The sample size for this analysis was driven by that of the parent FIEBRE study and is described in detail elsewhere [14].
Statistical Analyses
We used median and interquartile range (IQR) to summarize continuous variables, while categorical variables were summarized using percentages. We used range to summarize antibody titers by serogroup. To investigate clinical predictors and exposures associated with leptospirosis, we used separate logistic regression models to assess the associations between confirmed or supportive evidence of leptospirosis and the sociodemographic and clinical variables, adjusted for sex and age without data imputation. To account for the possibility of differences in predominant exposure pathways between Africa and Asia, we conducted subgroup analyses separately for data from African sites and from the Asian site. We used bivariable analyses, retaining significant covariates at P < .1 and backward exclusion of nonsignificant covariates with P > .05 to arrive at a final parsimonious model. The variance inflation factor was used to examine potential collinearity. Age and sex were considered a priori confounders and were included in multivariable models. Uncertainty was reported as 95% confidence intervals (CIs). To explore the possibility of variation in predominant transmission routes by continent, and particularly the role of ruminant livestock as sources for leptospirosis at African sites [8–10], we undertook subgroup analyses separately for data from Africa and Laos. All data analyses were performed using STATA version 18.0 (Stata Corp, College Station, Texas).
Research Ethics
Ethics approval was obtained from the Lao National Ethics Committee for Health Research Committee and the Oxford Tropical Research Ethics Committee, United Kingdom, for Laos; the University of Malawi College of Medicine Research and Ethics Committee and the Liverpool School of Tropical Medicine Research Ethics Committee for Malawi; Comité Institucional de Medical Research Bioética para a Saúde do Centro de Investigação em Saúde de Manhiça and the Comité Nacional de Bioética em Saúde de Moçambique for Mozambique; and the Medical Research Council of Zimbabwe for Zimbabwe. The study was also approved by the research and ethics committee of the London School of Hygiene and Tropical Medicine. Written informed consent was obtained from all study participants or their parents or guardians.
Role of the Funding Source
The funder had no role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; nor in the decision to submit the paper for publication.
RESULTS
Of 7851 febrile participants enrolled across study sites from 22 June 2018 to 31 March 2021, 142 had missing serology and PCR results, and 7413 (94.4%) had at least day 0 or day 28 serum samples available for testing for leptospirosis, of which 4682 (59.6%) had paired day 0 and day 28 sera available, and 7273 (92.6%) had plasma available for PCR analysis (Figure 1).
Study flow diagram for acute leptospirosis prevalence and risk factors in the Febrile Illness Evaluation in a Broad Range of Endemicities (FIEBRE) study, 2018–2021.
Of 7851 febrile participants, 134 (1.7%) had confirmed leptospirosis: 89 (1.1%) by ≥4-fold rise in Leptospira MAT titer between the acute and convalescent sample, 13 (0.2%) by a single Leptospira MAT reciprocal titer ≥800, and 38 (0.5%) by Leptospira lfb1 PCR. Among those confirmed by Leptospira lfb1 PCR, the detected Leptospira species are shown in Table 1. Confirmed leptospirosis was identified in 88 (4.6%) participants from Laos, 177 (1.0%) from Malawi, 7 (0.3%) from Mozambique, and 22 (1.2%) from Zimbabwe (Table 2). Of 89 participants with a ≥4-fold rise in Leptospira MAT titer between the acute and convalescent sample and a Leptospira lfb1 PCR result, 6 (6.7%) were also Leptospira lfb1 PCR positive. Of 12 participants with a single Leptospira MAT reciprocal titer ≥800 and a Leptospira lfb1 PCR result, 0 (0.0%) were Leptospira lfb1 PCR positive. Of 22 participants positive by Leptospira lfb1 PCR and paired sera tested by Leptospira MAT, 6 (27.3%) also had a ≥4-fold rise in Leptospira MAT titer between the acute and convalescent sample. Of 16 participants who were positive by Leptospira lfb1 PCR and a serum sample tested by Leptospira MAT, 0 (0.0%) had a single Leptospira MAT reciprocal titer ≥800. In Laos 14 (15.9%) of 88 cases of confirmed leptospirosis were diagnosed by PCR, whereas in Africa sites 24 (52.2%) of 46 cases of confirmed leptospirosis were diagnosed by PCR.
The median (IQR) age of all participants with confirmed leptospirosis was 27 (17–41) years compared with 18 (4.8–33) years for those without confirmed leptospirosis (P < .001). Of pediatric participants, 31 (0.9%) had confirmed leptospirosis, and the median (IQR) age was 8 (5–11) years. Among adult participants, 103 (2.5%) had confirmed leptospirosis, and the median (IQR) age was 35 (23–46) years. Among all participants, 62 (46.3%) with confirmed leptospirosis were female compared with 4006 (52.9%) of those without confirmed leptospirosis (P = .128).
Of 7851 febrile participants, 23 (0.3%) had supportive evidence of leptospirosis. Supportive evidence of leptospirosis was identified in 18 (2.3%) participants from Laos, 1 (0.3%) from Malawi, 1 (0.1%) from Mozambique, and 3 (0.5%) from Zimbabwe (Table 2).
Clinical Characteristics and Predictors of Leptospirosis
Clinical characteristics of participants with and without confirmed or supportive evidence of leptospirosis are shown in Table 3. On bivariable analysis of participants with confirmed or supportive evidence of leptospirosis compared with those without the median (IQR) admission temperature was 38.0°C (37.6°C, 38.5°C) versus 38.1°C (37.7°C, 38.9°C) (odds ratio [OR] 0.77 per °C, P = .026), median (IQR) oxygen saturation 96.0% (95.0%, 98.0%) versus 97.0% (95.0%, 98.0%) (OR 0.96 per %, P = .008), median (IQR) respiratory rate was 22.0 (20.0. 25.0) versus 22.0 (20.0, 28.0) per minute (OR 0.96 per breath per minute, P = .001), headache was reported by 114 (78.6%) versus 3440 (66.1%) (OR 1.9, P = .002), conjunctivitis was observed in 4 (2.5%) versus 57 (0.8%) (OR 3.40, P = .019), the median (IQR) Universal Vital Assessment score among adults was 0.0 (0.0–0.0) versus 0 (0.0–2.0) (OR per unit 0.65, P < .001), jaundice was seen in 10 (6.3%) versus 195 (2.6%) (OR 2.56, P = .005), and antimalarials were administered in 3 (1.9%) versus 980 (13.2%) (OR 0.13, P = .001). A multivariable analysis found headache (adjusted OR [aOR] 2.20, P < .001), rash or skin lesions (aOR 1.45, P = .001), conjunctivitis (aOR 3.33, P < .001), and jaundice (aOR 1.75, P < .001) remained associated with confirmed or supportive evidence of leptospirosis, whereas administration of antimalarials was associated with reduced odds of confirmed or supportive evidence of leptospirosis (aOR 0.10, P = .002). Of those with confirmed or supportive evidence of leptospirosis, 2 (1.3%) of 151 with vital outcome data died in hospital.
Exposures Associated With Leptospirosis
Exposures reported by participants with and without confirmed or supportive evidence of leptospirosis are shown in Table 4. On bivariable analysis of participants with confirmed or supportive evidence of leptospirosis compared with those without the median (IQR) age was 26.5 (17.0, 43.0) versus 18.0 (4.7, 33.0) years (OR 1.02 per year, P < .001), living or working in close contact with cattle in the past month was reported by 19 (12.2%) versus 439 (5.9%) (OR 2.23, P = .001), living or working in close contact with cattle, goats, or pigs in the past month by 24 (15.4%) versus 769 (10.3%) (OR 1.59, P = .040), wading, swimming, or bathing in pond water, lake water, or steam water in the past month by 44 (28.0%) versus 667 (8.9%) (OR 3.98, P < .001), working in rice fields in the past month by 61 (38.9%) versus 580 (7.8%) (OR 7.56, P < .001), a river as the source of drinking water in the dry season by 3 (1.9%) versus 21 (0.3%) (OR 6.95, P = .002), and a river or pond the source of drinking water in the dry season by 3 (1.9%) versus 23 (0.3%) (OR 6.34, P = .003), respectively. On multivariable analysis, working in rice fields in the past month (aOR 6.24, P < .001) and having a river as the source of drinking water in the dry season (aOR 5.11, P = .001) remained associated with confirmed or supportive evidence of leptospirosis.
Of participants at African sites, 4 (8.5%) of 47 with confirmed or supportive evidence of leptospirosis and 80 (1.4%) of 5673 without worked in rice fields. On multivariable analysis of exposures at African sites, working in rice fields in the past month (aOR 9.10, P < .001) was associated with confirmed or supportive evidence of leptospirosis, and living and working in close contact with cattle in the past month (aOR 1.56, P = .309) was not. In contrast, among participants at the Asian site, 47 (53.4%) of 88 with confirmed or supportive evidence of leptospirosis and 500 (27.6%) of 1809 without worked in rice fields. On multivariable analysis of exposures at the Laos site, working in rice fields in the past month (aOR 2.94, P = .001) and having a river as the source of drinking water in the dry season (aOR 9.25, P = .009) were associated with confirmed or supportive evidence of leptospirosis.
Predominant Reactive Leptospira Serogroups, Species, and Potential Host Range
Table 5 shows the predominant reactive Leptospira serogroup among participants with serologically confirmed leptospirosis based on ≥4-fold rise in titer between acute and convalescent serum by study site. In Laos, participants with serologically confirmed leptospirosis were predominantly reactive to Leptospira serogroups Australis, Sejroe, Bataviae, Icterohemorrhagiae, Grippotyphosa, Autumnalis, Celledoni, Pomona, and Hebdomadis in descending order of prevalence. Strains representing these serogroups have been isolated from a wide range of host species in Asia, including but not limited to rodents, ruminant livestock, dogs, and pigs [21, 22]. In Malawi, participants with serologically confirmed leptospirosis were predominantly reactive to Leptospira serogroups Icterohemorrhagiae, Sejroe, Australis, Mini, and Pyrogenes; in Mozambique to Leptospira serogroups Australis, Autumnalis, and Icterohemorrhagiae; and in Zimbabwe to Leptospira serogroups Ballum, Icterohemorrhagiae, Pomona, and Pyrogenes. Strains representing these serogroups have been predominantly isolated from rats and cattle in Africa (Table 5) [21, 22]. Among the identified Leptospira species Leptospira borgpetersenii, Leptospira interrogans, and Leptospira kirschneri, variation was observed between study sites, also consistent with variation in host species (Table 1).
DISCUSSION
Using a standardized study design and laboratory strategy, we showed that leptospirosis was a common cause of febrile illness at a site in Laos, and was present but less common at sites in Malawi, Mozambique, and Zimbabwe. In terms of clinical features, headache, rash or skin lesions, conjunctivitis, and jaundice were associated with increased odds of confirmed or supportive evidence of leptospirosis. Exposures, including working in rice fields in the past month and having a river as the source of drinking water in the dry season, were associated with increased odds of confirmed or supportive evidence of leptospirosis. L. interrogans, L. kirschneri, and L. borgpetersenii were confirmed in participants with positive lfb1 PCR. A wider diversity of Leptospira predominant reactive serogroups and potential host species was observed in Laos compared with in African sites. Rats and cattle feature as common potential hosts across all study sites.
Leptospirosis often presents as a nonspecific febrile illness that is difficult to distinguish from other causes of fever by clinical history and physical examination alone [5]. We found that headache, rash or skin lesions, conjunctivitis, and jaundice, all recognized clinical features of leptospirosis, were associated with increased odds of the disease. However, while these features support a diagnosis of leptospirosis, none is sufficiently sensitive nor specific to be reliable for leptospirosis diagnosis alone. This highlights the need for wider access to reference diagnostics for leptospirosis, and better still, for developing point-of-care tests of sufficient accuracy to be useful for patient care [23, 24].
Working in rice fields in the past month and measures of surface water exposure were associated with increased odds of leptospirosis across FIEBRE study sites. Notably, an analysis of risk factors for leptospirosis restricted to African sites confirmed the role of rice field exposure at those sites but found no significant association with living and working in close contact with cattle despite other African studies identifying an important role for cattle exposure in leptospirosis risk [8, 10]. While rice field exposure was considerably less common among participants at African sites compared with the Asian site, this finding highlights the potential impact on leptospirosis risk of increases in irrigated rice farming in Africa [25]. The lack of association of leptospirosis with cattle exposure in African sites highlights the diverse ecology of the disease by location, even within the same region.
The diversity of Leptospira predominant reactive serogroups was higher in Laos than in African sites, possibly in part because the higher number of participants with serologically confirmed disease with serologically confirmed disease in Laos. Additionally, the Laos MAT panel was supplemented with local Leptospira strains, whereas we had limited ability to enrich the African MAT panel with local strains since relatively very few Leptospira strains have been isolated from African countries [21, 22]. This was in turn associated with a wider range of potential host species in Laos than in the African sites. While using predominant patterns of Leptospira serogroup reactivity provides only a crude insight into potential animal hosts of infecting strains [26], the findings generate hypotheses for future studies in these locations to investigate specific animal contacts as risk factors for human infection.
Our study had a number of limitations. MAT was only done after screening of acute and convalescent serum by L. fainei serovar Hurstbridge IgM ELISA, the sensitivity of which is uncertain for the diagnosis of leptospirosis particularly in Africa. Since the case definition for confirmed leptospirosis relied in part on the availability of a convalescent serum sample for MAT, it is likely that the case fatality ratio of leptospirosis was underestimated among those who died before a convalescent sample was collected. PCR to lfb1 detected a larger proportion of confirmed leptospirosis infections relative to MAT among participants enrolled at African sites relative to the Asian site. This may reflect unmeasured differences in pre-enrollment antimicrobial use in Laos compared with the African sites, or perhaps the African MAT panel did not sufficiently represent the diversity of Leptospira strains circulating at the African sites compared with the Asian site. More work is needed to increase available isolates of pathogenic and intermediate pathogenic Leptospira from African countries to improve the performance of serologic diagnosis and gain a more complete picture of predominant reactive serogroup diversity. While our risk factor questionnaire included questions relevant to leptospirosis, it was not comprehensive and was insufficient to gain a nuanced picture of leptospirosis risk factors by site. The use as controls of participants presenting to healthcare facilities rather than those from the community may have introduced bias. Since leptospirosis was less common in Malawi, Mozambique, and Zimbabwe than Laos, our power to detect risk factors at African sites was reduced.
We confirm that leptospirosis is an important cause of fever in Laos and was present but less common at all 3 African sites studied. Since a specific diagnosis of leptospirosis cannot be made by clinical means alone, ongoing efforts to develop accurate diagnostic tests suitable for use in low-resource settings are needed. Rice field exposure is a major risk factor for infection, even in Africa, where rice field exposure was not as common, highlighting the need for focused prevention in rice field workers, especially as irrigated rice farming expands in Africa. We highlight the need to redouble efforts to isolate Leptospira strains in Africa to improve serologic diagnosis and identify hypotheses for more detailed risk factor studies.
Supplementary Material
jiaf464_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shrestha P, Dahal P, Ogbonnaa-Njoku C, et al Non-malarial febrile illness: a systematic review of published aetiological studies and case reports from Southern Asia and South-eastern Asia, 1980–2015. BMC Med 2020; 18:299.32951591 10.1186/s 12916-020-01745-0PMC 7504862 · doi ↗ · pubmed ↗
- 2Elven J, Dahal P, Ashley EA, et al Non-malarial febrile illness: a systematic review of published aetiological studies and case reports from Africa, 1980–2015. BMC Med 2020; 18:279.32951596 10.1186/s 12916-020-01744-1PMC 7504660 · doi ↗ · pubmed ↗
- 3Allan KJ, Biggs HM, Halliday JE, et al Epidemiology of leptospirosis in Africa: a systematic review of a neglected zoonosis and a paradigm for ‘One Health’ in Africa. P Lo S Negl Trop Dis 2015; 9:e 0003899.26368568 10.1371/journal.pntd.0003899 PMC 4569256 · doi ↗ · pubmed ↗
- 4Biggs HM, Bui DM, Galloway RL, et al Leptospirosis among hospitalized febrile patients in northern Tanzania. Am J Trop Med Hyg 2011; 85:275–81.21813847 10.4269/ajtmh.2011.11-0176 PMC 3144825 · doi ↗ · pubmed ↗
- 5Levett PN . Leptospirosis. Clin Microbiol Rev 2001; 14:296–326.11292640 10.1128/CMR.14.2.296-326.2001 PMC 88975 · doi ↗ · pubmed ↗
- 6Mwachui MA, Crump L, Hartskeerl R, Zinsstag J, Hattendorf J. Environmental and behavioural determinants of leptospirosis transmission: a systematic review. P Lo S Negl Trop Dis 2015; 9:e 0003843.26379035 10.1371/journal.pntd.0003843 PMC 4574979 · doi ↗ · pubmed ↗
- 7Bovet P, Yersin C, Merien F, Davis CE, Perolat P. Factors associated with clinical leptospirosis: a population-based case-control study in the Seychelles (Indian Ocean). Int J Epidemiol 1999; 28:583–90.10405868 10.1093/ije/28.3.583 · doi ↗ · pubmed ↗
- 8Maze MJ, Cash-Goldwasser S, Rubach MP, et al Risk factors for human acute leptospirosis in northern Tanzania. P Lo S Negl Trop Dis 2018; 12:e 0006372.29879114 10.1371/journal.pntd.0006372 PMC 5991637 · doi ↗ · pubmed ↗