Soluble cytokines enhance risk prediction across all stages of classical Hodgkin lymphoma
Alexandra Kredátusová, Tomáš Chupáň, Heidi Móciková, Alice Sýkorová, Jana Marková, Marie Lukášová, Ľubica Gahérová, Pavla Štěpánková, Eva Kriegová, Mária Maco, Tomáš Kozák, Tomáš Papajík, Stephen M. Ansell, Vít Procházka

TL;DR
This study shows that measuring certain soluble cytokines improves predicting outcomes for classical Hodgkin lymphoma patients at all disease stages.
Contribution
The study introduces a new prognostic model using soluble cytokines that works across all stages of classical Hodgkin lymphoma.
Findings
High levels of sIL-6 and sCD30 are linked to worse outcomes and advanced disease features in cHL.
A new model combining age, extranodal disease, and cytokine levels outperforms existing risk models.
Patients with elevated sCD30 and sIL-6 have significantly worse 5-year progression-free survival.
Abstract
Classical Hodgkin lymphoma (cHL) is a heterogeneous malignancy with favorable outcomes, but accurate prognostic stratification remains challenging, particularly across all disease stages. Traditional risk models are focused on advanced stages and do not account for tumor microenvironment (TME) dynamics. Soluble cytokines reflecting TME activity may offer additional prognostic value. In our prospective multicenter study, we investigated the prognostic value of pretreatment plasma levels of soluble TARC, sCD30, sCD163, and sIL-6 in 162 newly diagnosed cHL patients and developed a model incorporating these biomarkers for risk prediction across all stages. Cytokine levels were measured using ELISA, and clinical characteristics, treatment responses, and outcomes were collected. The primary endpoint was 5-year progression-free survival (PFS). Elevated levels of sIL-6 and sCD30 were associated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
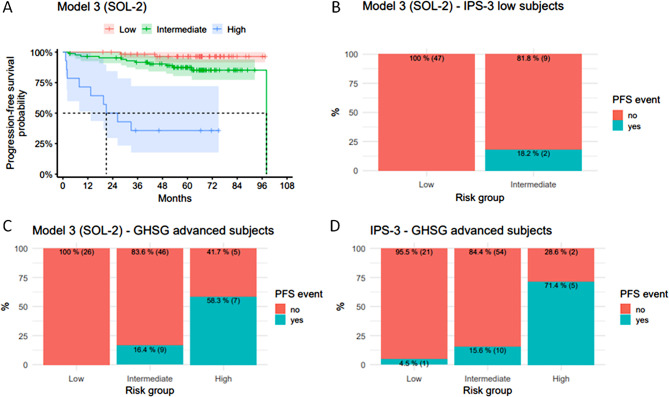 Figure 1
Figure 1- —https://doi.org/10.13039/501100009553Agentura Pro Zdravotnický Výzkum České Republiky
- —https://doi.org/10.13039/501100003243Ministerstvo Zdravotnictví Ceské Republiky
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphoma Diagnosis and Treatment · CAR-T cell therapy research · Cancer Immunotherapy and Biomarkers
To the editor,
we conducted a prospective multicenter study to evaluate soluble cytokines as predictors of outcomes in classic Hodgkin lymphoma (cHL). cHL has a generally favorable prognosis, however, some patients, even in the intermediate stage, experiences disease progression or relapse. This highlights the need for a prognostic model applicable across all disease stages to refine risk stratification and guide treatment decisions. We aimed to integrate clinical features with soluble cytokine markers to create a more precise prognostic tool. We hypothesized that soluble biomarkers in plasma reflect the tumor microenvironment (TME), and while linked to immune evasion and tumor growth in cHL [1–3], influence tumor behavior and patient outcomes. The goal of our study was to incorporate these markers into a model capable of predicting progression-free survival (PFS) in cHL patients, irrespective of clinical stage. A total of 162 patients diagnosed with cHL, with a median age of 42 years, were recruited from three institutions within Czech Hodgkin Lymphoma Study Group. The cohort included patients with various stages based on the German Hodgkin Study Group (GHSG) classification: 16% of patients were categorized as having early-stage disease, 25% as intermediate, and 59% as advanced. During a median follow-up period of 64.1 months (1.3–111.0), twenty-three PFS-related and thirteen OS-related events were observed. The five-year PFS rate was 86% (95% CI: 0.81–0.92), and 92% of patients (95% CI: 0.88–0.96) remained alive at five years without an OS event. The primary aim was to develop a complex prognostic model to predict PFS and stratify patients into low, intermediate, and high-risk categories. We identified age, albumin levels, and extranodal involvement as key variables for Model 1, which was further refined by incorporating soluble cytokines (sIL-6, sCD30, sCD163, and TARC) [4]. Elevated levels of sCD163 and sIL-6 or sCD30 and sIL-6 were linked to significantly worse PFS. We also explored alternative models incorporating cytokine combinations, resulting in Models 2 and 3. These models retained age and extranodal involvement, replacing albumin levels with cytokine pairs. Models 2 and 3 showed comparable Akaike Information Criterion (AIC) and C-index values to Model 1. Cross-validation confirmed that Model 3, which included the sCD30/sIL-6 high-high cytokine combination, outperformed the IPS-3 score [5] in predicting patient outcomes, particularly for advanced-stage patients (Table 1). For clinical applicability, we discretized the linear predictors from Models 1–3 into three risk groups using the rsolr12() function. Model 3, applying the SOL-2 algorithm, showed the best separation in Kaplan–Meier survival curves (Fig. 1A). Notably, Model 3 also provided finer stratification than IPS-3, particularly for low-risk patients classified by IPS-3, suggesting that our model may identify high-risk patients who would benefit from more intensive treatment despite their low IPS-3 score (Fig. 1B). Further validation against IPS-3 in a subgroup of GHSG advanced-stage patients demonstrated that Model 3 could better differentiate between intermediate- and high-risk patients compared to IPS-3 (Fig. 1C-D). To facilitate clinical application, an online calculator was developed to simplify the use of our model [6]. Our study has some limitations, including the relatively low number of high-risk patients due to the generally good treatment outcomes in cHL. A larger cohort is needed for further validation. The selection of cytokines is another limitation; other cytokines may also contribute to disease aggressiveness, which could be explored in future studies. TARC, although correlated with tumor burden, did not emerge as significant in the model, possibly reflecting disease activity rather than tumor aggression. This suggests that TARC may be more useful for monitoring disease activity than predicting patient outcomes [7, 8]. The strength of this study lies in its prospective design and multicenter approach, which enhances generalizability. All laboratory measurements were performed centrally using standardized ELISA methods, ensuring data consistency. Future studies should validate our model in larger cohorts treated with novel therapies such as brentuximab vedotin or immune checkpoint inhibitors. Combining soluble biomarkers with genetic profiling, such as cell-free DNA analysis, could offer a more comprehensive prognostic tool, enhancing personalized treatment strategies. In conclusion, soluble biomarkers like sIL-6 and sCD30, integrated into prognostic models, can improve risk stratification in cHL, particularly for borderline-stage disease or patients with unrecognized high-risk features. Our findings support the development of more individualized, risk-adapted strategies beyond traditional staging systems.
Table 1. Comparison of the models’ performanceModelIBS (data)IBS (CV)C-index (data)C-index (CV)Reference0.0930.093––Model 10.0670.0740.830.79Model 20.0690.0760.810.78Model 30.0690.0760.800.76Model 4 = IPS-3 score only0.0730.0770.720.70Note: IBS = Integrated Brier Score, a measure of prediction error for survival models. The C-index measures how well the model discriminates between patients. It represents the probability that, for any two patients, the one who experiences the event earlier had a higher predicted risk according to the model. A C-index of 0.5 indicates no predictive ability (equivalent to chance), whereas a C-index of 1.0 reflects perfect discrimination. The AIC quantifies model quality by balancing fit and complexity (lower AIC indicates a better-fitting, more parsimonious model)
Fig. 1(A) Progression-free survival (all patients) stratified according to the Model 3. (B) The distribution of PFS events across IPS-3 low risk pts according to the Model-3 risk groups. (C) Progression-free survival (GSHG-advanced pts) stratified according to the Model 3. (D) Progression-free survival (GSHG-advanced pts) stratified according to the IPS-3
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aldinucci D, Gloghini A, Pinto A, De Filippi R, Carbone A. The classical Hodgkin’s lymphoma microenvironment and its role in promoting tumour growth and immune escape. J Pathol. 2010;221(3):248 – 63. 10.1002/path.2711. PMID: 20527019.10.1002/path.271120527019 · doi ↗ · pubmed ↗
- 2Available from: https://tomchupan.shinyapps.io/H Lrisk/. Accessed 8 October 2025.