The effects of emotional distress on the postoperative survival and progression in patients with breast cancer: a prospective observational study
Shanqing Xu, Li Yang, Juan Zhang, Aihua Tan, Dabao Xu, Jianbin Tong

TL;DR
This study shows that emotional distress in breast cancer patients after surgery is linked to worse survival and faster disease progression.
Contribution
The study provides new prospective evidence linking emotional distress to poorer breast cancer outcomes.
Findings
Emotional distress was associated with lower 7-year overall survival rates (78.5% vs. 93.7%).
Adjusted analysis showed emotional distress increased the risk of disease progression (HR = 3.73).
Psychological assessment and care should be integrated into cancer management.
Abstract
Emotional distress (ED), characterized by symptoms of depression and anxiety, is highly prevalent in patients with breast cancer. Although retrospective studies suggest an association between ED and adverse cancer outcomes, findings from prospective studies remain inconsistent. This prospective observational study aimed to investigate the association between emotional distress and long-term survival outcomes in patients with breast cancer following curative surgery. A total of 159 patients with breast cancer were enrolled. Baseline levels of emotional distress were assessed using standardized scales. Patients were prospectively followed for up to 7 years to monitor overall survival (OS) and progression-free survival (PFS). Inverse probability of treatment weighting (IPTW) was employed to adjust the baseline confounders. The unadjusted 7-year OS and PFS rates in patients with ED were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
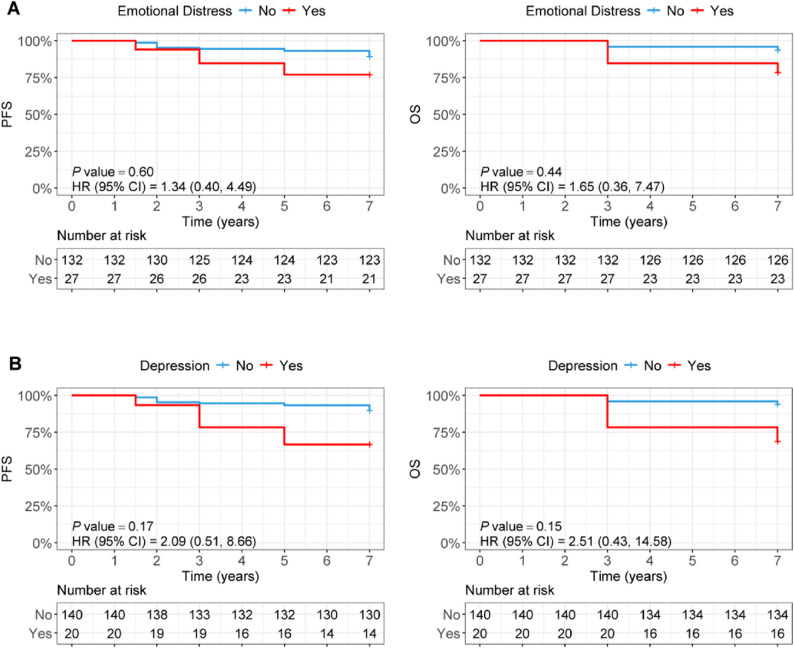 Figure 1
Figure 1- —National Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer survivorship and care · Cancer, Stress, Anesthesia, and Immune Response · Music Therapy and Health
Introduction
Breast cancer is the most commonly diagnosed cancer in women [1, 2]. According to the WHO statistics in 2022, the incidence of breast cancer varies between 26.7 in 100 000 and 100.3 in 100 000 [2]. Despite significant improvements in clinical outcomes owing to advances in early detection and treatment [1, 3, 4], breast cancer still accounts for approximately 7% of all female cancer deaths [5]. Consequently, further improving the long-term prognosis of patients has become a major focus of contemporary breast cancer research.
To date, a number of factors have been reported to affect the recurrence and metastasis of breast cancer after curative surgery [1, 3, 6–9]. Among them, histological subtypes, the status of lymph nodes, and tumor size are well-known risk factors [10–12]. Emotional distress, commonly characterized by symptoms of depression and/or anxiety, is common in patients with breast cancer [13–15]. Its prevalence among breast cancer patients is estimated to be 15 to 54% [16, 17]. Although most women with breast cancer believe that emotional distress has an important influence on the recurrence of their cancer, inconsistent results between retrospective studies and prospective studies have been reported [13, 18]. Population-based retrospective studies have showed that emotional distress is associated with an increased risk of mortality and recurrence of breast cancer. In contrast, a population-based prospective cohort study showed no significant effect of emotional distress on the distant disease-free survival and overall survival of breast cancer patients during median follow-up of 8.2 years (0.8 to 14.4 years) [8]. Another prospective case-control study of 34 breast cancer patients during follow-up of 25 years supported a predictive role of emotional distress for relapse-free survival [19]. These inconsistent findings suggest that (1) the relationship between the prognosis of breast cancer and emotional distress after surgery remains unclear, (2) a relatively short follow-up period in some studies may not be sufficient to observe the long-term impact on survival outcomes, given the high 5-year survival rates of breast cancer (77.5%-90.3%).
To test the relationship between the prognosis of breast cancer and emotional distress after surgery, we evaluated the levels of postoperative emotional distress, and prospectively detected the survival and recurrence of 159 patients with breast cancer(recruited from 1st May 2018 to 8th October 2019)during follow-up of 7 years.
Materials and methods
Study design and population
This prospective observational cohort study was conducted as a post-hoc follow-up of a previously completed randomized, double-blind, placebo-controlled trial, which evaluated the effect of probiotic supplementation on cognitive function in breast cancer patients undergoing neoadjuvant chemotherapy [20]. All participants had completed neoadjuvant chemotherapy prior to enrollment in the present study. The original RCT enrolled 160 eligible patients (stage I-III breast cancer, aged 20–60 years, no immune diseases), who were randomly assigned to receive either probiotics or placebo. The present study was a post-trial observational follow-up study focusing on the association between baseline emotional distress and long-term survival, irrespective of the original intervention. One patient was lost to follow-up, resulting in 159 patients included in the final analysis. All patients were followed until September 1, 2025, with a median follow-up of 7 years (range: 1.5–7 years). The study protocol was approved by the Ethics committee of Third Xiangya Hospital, Central South University, Changsha, China(2020-S289).
Definition of emotional distress
The Self-rating Anxiety Scale (SAS), a validated 20-item instrument with established reliability and validity in Chinese cancer populations, was used to assess the severity of anxiety symptoms. Each item is rated on a 4-point Likert scale, with responses ranging from 1 (“none of the time”) to 4 (“most of the time”). Total scores are computed by summing individual item scores, resulting in a range of 20 to 80 [21, 22]. Consistent with validated diagnostic thresholds for clinical research [21, 22], a total SAS score ≥ 50 was defined as clinically significant anxiety. Similarly, the Self-rating Depression Scale (SDS)—a 20-item tool with comparable reliability and validity in the target population—was used to evaluate depressive symptom severity, employing the same 4-point Likert scoring system as the SAS (total score range: 20–80) [23, 24]. A total SDS score ≥ 53 was defined as clinically significant depression, in accordance with validated cutoff criteria [23, 24]. Emotional distress (ED) was defined as the presence of either clinically significant anxiety (SAS ≥ 50) or clinically significant depression (SDS ≥ 53), aligning with widely accepted standards for clinical distress in oncology settings [21, 23].
Data collection and outcomes
Follow-up data were primarily extracted from outpatient and inpatient hospital charts. For patients without recent hospital visits, information was collected via structured telephone interviews or WeChat. All endpoint events—death and disease progression—were adjudicated by an independent Clinical Events Committee, which remained blinded to the original treatment allocation. The primary outcome was progression-free survival (PFS), defined as the time from baseline to the first occurrence of disease progression or death from any cause. The secondary outcome was overall survival (OS), defined as the time from baseline to death from any cause.
Statistical analysis
Given that the classification of emotional distress (ED) was non-randomized and baseline differences were observed between the ED (n = 27) and non-ED (n = 132) groups, all analyses were conducted as observational. Categorical variables are reported as frequencies and percentages, while continuous variables are presented as medians with interquartile ranges (IQRs) due to non-normal distribution (assessed via Shapiro-Wilk test, data not shown). Baseline between-group comparisons were performed using the Mann–Whitney U test for continuous variables and Fisher’s exact test for categorical variables (due to small expected cell counts in some categories).
To ensure the rigor and reproducibility of results, statistical analyses were performed in a hypothesis-driven sequential framework, with each step focused on validating key assumptions or mitigating potential biases: (1) Validation of core survival model assumptions: For the log-rank test, Schoenfeld residuals derived from the univariate Cox proportional hazards (PH) model (its statistical equivalent) were used to verify the PH assumption (p > 0.05). For multivariate Cox models, variable-specific and global Schoenfeld tests confirmed that all covariates satisfied the PH assumption (p > 0.05)—a critical prerequisite for reliable hazard ratio (HR) estimates (Supplementary Tables S1 and S2). (2) Evaluation of inverse probability of treatment weighting (IPTW): IPTW was assessed across four key dimensions to minimize bias and ensure robustness: weight stability (summarized via descriptive statistics and histograms), covariate balance (standardized mean difference [SMD] < 0.3 and p > 0.05), appropriate propensity score specification (≥ 10 events per covariate), and absence of multicollinearity (variance inflation factor [VIF] < 5) (Supplementary Tables S3–S7). (3) Testing for multicollinearity: Multicollinearity in multivariate Cox models was evaluated using the VIF function from R’s car package. A VIF < 5 confirmed no substantial multicollinearity, ensuring accurate quantification of each variable’s independent association with survival outcomes (Supplementary Table S8). (4) Sensitivity analysis for time-dependent effects: Time-dependent Cox models (incorporating interaction terms of covariates [TNM stage and molecular subtype] with log(time + 20)) were used to address potential PH violations. These models were IPTW-weighted and adjusted for confounders to verify the robustness of primary findings (Supplementary Table S9). (5) Estimation of survival rates: Kaplan–Meier methods were used to estimate 1-, 3-, 5-, and 7-year PFS and OS rates. Logit transformation was applied to calculate 95% confidence intervals (CIs), which quantified uncertainty and enhanced the interpretability of long-term outcomes (Supplementary Table S10).
Results
Study baseline assessment
A total of 159 patients were included in the final analytical cohort. Using the predefined criteria (SAS ≥ 50 or SDS ≥ 53), 27 patients (17.0%) were classified as having baseline emotional distress (ED), and 132 patients (83.0%) were categorized into the non-ED group. The baseline clinical and demographic characteristics of the cohort, stratified by ED status, are summarized in Tables 1 and 2. The median age was 46.0 years (IQR: 39.0–52.0), and the median body mass index (BMI) was 23.05 kg/m² (IQR: 20.89–24.83). Comparative analysis revealed no significant differences in most baseline characteristics between the ED and non-ED groups, except for anxiety and depression scores, which were significantly higher in the ED group (both P < 0.001), thereby validating the classification scheme (Table 1).
Table 1. Baseline demographic and clinical characteristics of the follow-up cohortVariableOverall(n = 159)No ED(n = 132)ED(n = 27) P Age, median (IQR),year46.00(39.00,52.00)46.00 (39.75,53.00)45.00 (38.00,49.00)0.228BMI, median (IQR),kg/m²23.05 (20.89,24.83)23.04 (20.79,24.75)23.23 (21.52,24.87)0.943TNM Stage, n (%)0.014 І48 (30.20)34 (25.80)14 (51.90) П/Ш111 (69.80)98 (74.20)13 (48.10)Molecular subtype, n (%)0.728 HER-2- Negative87 (54.70)70 (53.00)17 (63.00) HER-2-Postive51(32.10)44(33.33)7(25.92) Tri-Negative21(13.20)18(13.63)3(11.11)Treatment, n (%)0.699 Placebo79(49.7)67(50.76)12(44.44) Probiotics80(50.3)65(49.24)15(55.56)Anxiety score,median (IQR)35.00 (30.00,40.00)34.00 (30.00,38.00)48.00 (43.50,53.00)< 0.001Depression score,median (IQR)39.00 (34.00,45.50)36.00 (34.00,43.00)54.00 (50.50,59.00)< 0.001
Table 2. Associations between emotional distress and survival analysis1-years, n (%), 95%CI3-years, n (%), 95%CI5-years, n (%), 95%CI7-years, n (%), 95%CIPFS survival rateDepressionNo140[100% (100.0-100.0)]132[94.6% (91.0-98.3)]130[93.3% (89.3–97.4)]125[89.7% (84.9–94.8)]Yes20[100% (100.0-100.0)]16[78.3% (55.5–100.0)]14[66.7% (43.7–100.0)]14[66.7% (43.7–100.0)]AnxietyNo146[100% (100.0-100.0)]137[94.1% (90.5–97.9)]135[92.2% (88-96.5)]130[88.8% (83.9–94.0)]Yes12[100% (100.0-100.0)]11[88.1% (68.8–100.0)]11[85.5% (65.8–100.0)]11[85.5% (65.8–100.0)]EDNo132[100% (100.0-100.0)]124[94.5% (90.8–98.3)]123[93.1% (89-97.3)]118[89.3% (84.3–94.6)]Yes27[100% (100.0-100.0)]23[84.6% (67.3–100.0)]21[76.9% (58.5–100.0)]21[76.9% (58.5–100.0)]OS survival rate nDepressionNo140[100% (100.0-100.0)]134[96% (92.8–99.2)]134[96% (92.8–99.2)]131[93.9% (90.1–97.9)]Yes20[100% (100.0-100.0)]16[78.3% (55.5–100.0)]16[78.3% (55.5–100.0)]14[68.8% (45.5–100.0)]AnxietyNo146[100% (100.0-100.0)]139[95.4% (92.2–98.8)]139[95.4% (92.2–98.8)]135[92.8% (88.7–97.0)]Yes12[100% (100.0-100.0)]11[88.1% (68.8–100)]11[88.1% (68.8–100.0)]11[88.1% (68.8–100.0)]EDNo132[100%(100.0-100.0)]126[95.9% (92.7–99.2)]126[95.9% (92.7–99.2)]123[93.7% (89.8–97.8)]Yes27[100% (100.0-100.0)]23[84.6% (67.3–100.0)]23[84.6% (67.3–100.0)]22[78.5% (60.0-100.0)]95%CI 95% confidence interval, PFS progression-free survival, OS overall survival, ED Emotional DistressCumulative survival rates were estimated using the Kaplan-Meier product-limit method based on weighted data. Here, "n" denotes the weighted expected number of survivors (not the original actual patient count)
Survival analysis
The endpoints were progression-free survival (PFS) and overall survival (OS). Kaplan-Meier methods with log-rank tests were used to compare 1-, 3-, 5-, and 7-year PFS and OS rates between the ED and non-ED groups, showing that patients with ED had consistently lower survival rates across all time points (7-year PFS: 76.9% vs. 89.3%; 7-year OS: 78.5% vs. 93.7% in the non-ED group) and Kaplan-Meier curves illustrated an inferior trend in PFS and OS for the ED group, though the unadjusted log-rank test was not statistically significant (P > 0.05; Table 2 and Fig. 1). To address baseline imbalances (e.g., TNM stage), inverse probability of treatment weighting (IPTW) was applied to adjust for covariates including intervention group (probiotics vs. placebo), age, BMI, molecular subtype, and TNM stage, and after adjustment, ED was independently associated with a significantly increased risk of OS events (adjusted HR = 6.52, 95% CI: 1.78–23.88, P = 0.005) and PFS events (adjusted HR = 3.73, 95% CI: 1.18–11.71, P = 0.024; Table 3). All statistical models met underlying assumptions: the proportional hazards (PH) assumption was verified via Schoenfeld residuals (P > 0.05 for all covariates; Supplementary Tables S1 and S2), and IPTW adjustment achieved adequate covariate balance (standardized mean difference < 0.3) with stable weights and no multicollinearity (variance inflation factor < 5; Supplementary Tables S3–S7), confirming result robustness. Sensitivity analyses using time-dependent Cox models (incorporating interaction terms of TNM stage/molecular subtype with log(time + 20)) to address potential PH violations showed that after adjusting for time-varying effects, confounders, and IPTW weighting, depression remained independently associated with worse PFS (HR = 5.25, 95% CI: 1.54–17.87, P = 0.008) and OS (HR = 8.42, 95% CI: 2.45–28.94, P = 0.001), ED was significantly associated with reduced PFS (HR = 3.69, 95% CI: 1.04–13.15, P = 0.044) and OS (HR = 6.47, 95% CI: 1.78–23.51, P = 0.005), while anxiety (SAS ≥ 50) showed no significant association with PFS (HR = 2.37, 95% CI: 0.46–12.34, P = 0.305) or OS (HR = 2.51, 95% CI: 0.78–8.07, P = 0.124), with detailed results presented in Supplementary Tables S9 and S10.
Fig. 1. Kaplan-Meier curves for progression-free survival (PFS) and overall survival (OS) stratified by baseline Emotional distress (ED) status A and Depression B
Table 3. Associations between emotional distress and survival outcomes (based on IPTW model)PFSOSGroupUnadjustedHR (CI 95%)AdjustedHR (CI 95%)Adjusted P Unadjusted HR (CI 95%)Adjusted* HR (CI 95%)Adjusted^^ P Depression No3.75(1.20,11.67)5.30 (1.84,15.31)0.0025.86 (1.65,20.82)8.48(2.50,28.63)0.001 YesAnxiety No1.39 (0.23,8.50)2.38 (0.42,13.60)0.3291.72 (0.22,13.62)2.51(0.75,8.35)0.134 YesED No2.36 (0.75,7.45)3.73(1.18,11.71)0.0243.72 (1.04,13.34)6.52 (1.78,23.88)0.005 YesIPTW* Inverse probability of treatment weighting
Discussion
The belief that cancer outcomes might be related to psychological factors dates back to around 200 AD when Galen hypothesized that melancholic women were predisposed to breast cancer [8]. Compared to patients with other cancers, patients with breast cancer are more likely to experience emotional distress because of concerns about altered body image, subsequent treatment, cancer recurrence, as well as economic burden. However, to date, the relationship between the prognosis of breast cancer and emotional distress after surgery remains unclear.
In this prospective observational study, we found that breast cancer patients with baseline emotional distress had significantly worse long-term survival outcomes after adjusting for key clinical confounders using IPTW. Our findings align with several previous studies reporting that emotional distress is associated with higher cancer-specific mortality and poorer overall survival [13, 25–27]. Our findings are different from a population-based prospective cohort study that showed no significant effect of emotional distress on the distant disease-free survival and overall survival of breast cancer patients during median follow-up of 8.2 years (0.8 to 14.4 years). A possible explanation for the difference is that the patients in our study were all recruited over a short period in a single medical center, ensuring more homogeneous treatments than the population-based prospective cohort study. Collectively, our study supports that emotional distress promotes the progression and metastasis of breast cancer after surgery.
The mechanisms by which emotional distress promotes the progression and metastasis of breast cancer after surgery is still unclear. Previous studies have indicated that emotional distress plays a potential role in fostering the development of an immunosuppressive tumor microenvironment via inducing the dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis. New evidence have showed that β-adrenergic signaling can suppress an effector phenotype in CD8 + T Cells and undermines checkpoint Inhibitor therapy [28]. Stress-glucocorticoid-TSC22D3 axis compromises therapy-induced antitumor immunity [29]. kisspeptin/GPR54 signaling plays an important role in the stress-induced tumor immune evasion [30]. These new findings support that emotional distress promotes the recurrence and metastasis of breast cancer after surgery possibly via complex molecular signaling of the HPA axis downstream.
Several limitations of our study should be acknowledged. First, the relatively small sample size, particularly the limited number of patients with ED, may limit the statistical power and increase the risk of type II errors, despite the use of robust statistical adjustment. Second, although we adjusted for several key confounders, residual confounding from unmeasured factors cannot be entirely ruled out. Third, ED was measured only at baseline (no longitudinal assessments during follow-up), precluding capture of dynamic ED changes—may have oversimplified the ED-survival relationship, future studies should use serial ED measurements to address this gap. Finally, the single-center design may affect the generalizability of our findings to broader breast cancer populations.
In conclusion, this prospective study provides evidence that emotional distress is independently associated with an increased risk of disease progression and mortality in breast cancer patients following curative surgery. These findings underscore the potential importance of systematic psychological screening and integrated supportive care in the comprehensive management of breast cancer.
Supplementary Information
Supplementary Material 1.