Pulmonary Electrical Injury: A Case Report on an Uncommon Cause of Refractory Hypoxemia
Santiago Rivera Castrillón, Jose F Zuluaga, Maria C Florian Perez, Daniel Filizzola, Manuela Orozco

TL;DR
This case report describes a rare instance of severe lung issues after high-voltage electrocution, highlighting the challenges in diagnosis and treatment.
Contribution
The paper presents a novel case of electrocution-induced pulmonary vascular injury with refractory hypoxemia and pulmonary hypertension.
Findings
The patient exhibited severe hypoxemia and pulmonary hypertension disproportionate to imaging findings.
CT pulmonary angiography identified distal subsegmental pulmonary embolism on day 4.
The patient's condition progressed to multiorgan failure despite standard interventions.
Abstract
Pulmonary involvement after high-voltage electrocution is rare and may present with hypoxemia and pulmonary hypertension out of proportion to imaging, suggesting a vascular/endothelial mechanism. The objective of this report is to describe a case of disproportionate hypoxemia with severe pulmonary hypertension after electrocution, highlight diagnostic pitfalls, and outline management implications. A previously healthy 46-year-old man sustained high-voltage electrocution, required prolonged resuscitation, and developed severe hypoxemia (PaO₂/FiO₂ (ratio of arterial oxygen partial pressure to fractional inspired oxygen): 68) despite protective ventilation and proning. CT showed only mild posterior ground-glass change; echocardiography revealed preserved right ventricular function. On ICU day 4, a CT pulmonary angiogram (CTPA) identified very distal subsegmental pulmonary embolism.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
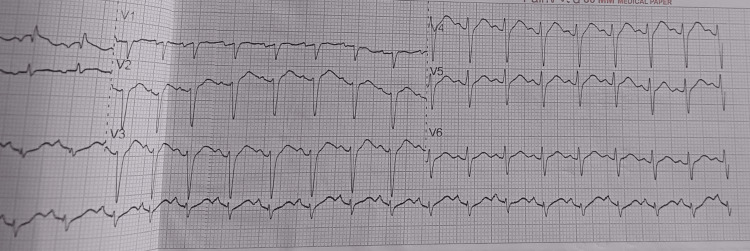 Figure 1
Figure 1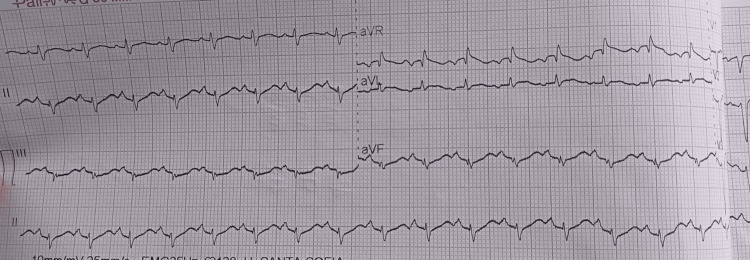 Figure 2
Figure 2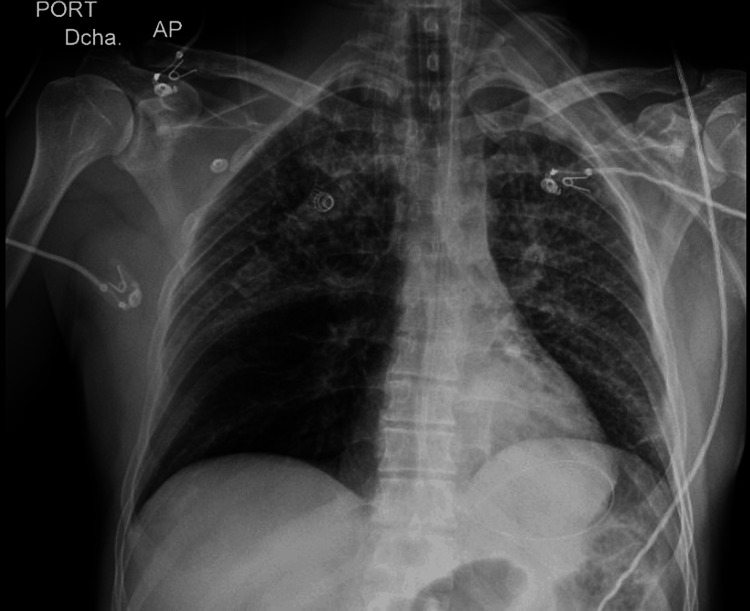 Figure 3
Figure 3 Figure 4
Figure 4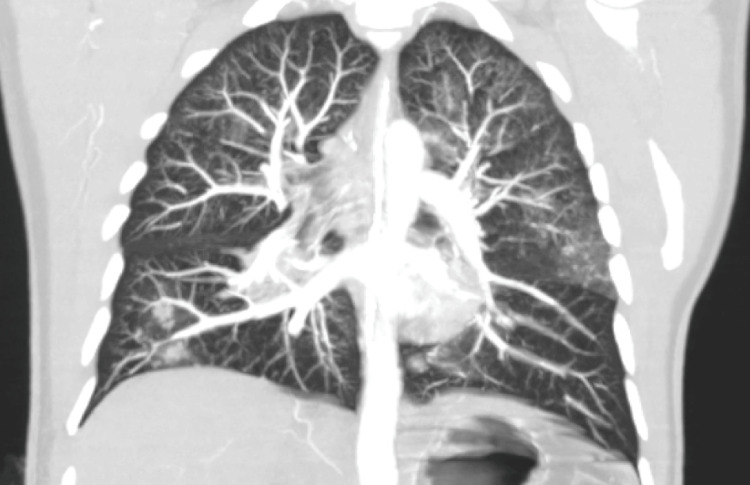 Figure 5
Figure 5| Parameter | Result | Units | Reference range | Comment |
| Arterial pH | 7.23 | — | 7.35–7.45 | Mixed acidosis |
| PaCO₂ | 46 | mmHg | 35–45 | — |
| HCO₃⁻ | 19.3 | mmol/L | 22–26 | — |
| Lactate | 4.4 | mmol/L | 0.5–2.0 | Elevated |
| Base excess | −8.3 | mmol/L | −2 to +2 | — |
| Urine output (0–24 h) | Anuria | mL/24 h | >0.5 mL/kg/h | Consistent with AKI |
| Serum creatinine | 2.7 | mg/dL | 0.6–1.3 | Consistent with AKI |
| Urea | 25 | mg/dL | 10–50 | — |
| Potassium | 3.5 | mmol/L | 3.5–5.1 | — |
| Sodium | 140 | mmol/L | 135–145 | — |
| Total CPK | 9,214 | U/L | 20–200 | Rhabdomyolysis |
| Troponin T | 27,500 | ng/L | <14 | Myocardial injury |
| INR | 1.2 | — | 0.8–1.2 | __ |
| Platelets | 250 | ×10⁹/L | 150–400 | — |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBurn Injury Management and Outcomes · Restraint-Related Deaths · Planarian Biology and Electrostimulation
Introduction
Electrical injuries, particularly high-voltage exposures, are uncommon but carry substantial multisystem morbidity (cardiovascular, musculoskeletal, and integumentary) [1,2]. Pulmonary involvement is rare and likely underrecognized [1,3,4]. Reported phenotypes span diffuse alveolar hemorrhage and non-cardiogenic pulmonary edema to acute pulmonary hypertension and severe hypoxemia with minimal imaging abnormalities, a pattern consistent with a vascular/endothelial mechanism driven by electroporation-related endothelial injury, acute vasoconstriction, and microthrombosis [1-3,5-7]. Clinically, this may present with profound hypoxemia, elevated pulmonary artery pressures, and preserved right-ventricular function, with CT showing only mild parenchymal change.
Here, we report a high-voltage electrocution followed by disproportionate hypoxemia and marked pulmonary hypertension despite minimal imaging findings and preserved right ventricular (RV) function. We highlight diagnostic pitfalls, including the limited explanatory value of isolated very distal subsegmental PE, and discuss management implications in the ICU (hemodynamic profiling, consideration of inhaled vasodilators, and criteria for veno-venous extracorporeal membrane oxygenation (VV-ECMO)) [1,4-10].
Rationale/novelty
Pulmonary electrical injury with hypoxemia and pulmonary hypertension out of proportion to imaging is under-recognized and diagnostically challenging. By pairing this phenotype with quantitative invasive hemodynamics and a pragmatic escalation pathway, we aim to help clinicians identify and manage similar presentations.
Case presentation
A 46-year-old male with no relevant medical history sustained a high-voltage electrical injury after direct contact with a primary energy distribution line. A family member trained in basic life support found him unresponsive and pulseless, initiating resuscitation that continued en route to a tertiary care hospital. Upon arrival, he remained in ventricular fibrillation, requiring three 200-joule biphasic defibrillation shocks. Return of spontaneous circulation (ROSC) was achieved after 25 minutes.
Post-resuscitation examination revealed burn marks on the right hand (entry point), occipital scalp, right chest, scapular region, abdomen, and right leg (exit point). In the ICU on admission (day 0), the findings were: blood pressure 109/61 mmHg (mean arterial pressure (MAP) ≈ 77 mmHg), heart rate 123 bpm, oxygen saturation (SpO₂) 93% on invasive ventilation, and temperature 36.5 °C. He remained in shock, requiring vasopressor and ventilatory support.
Initial laboratory findings showed severe mixed acidosis, anuria, markedly elevated creatine phosphokinase (9,214 U/L), and troponin T (27,500 ng/L), as well as active gastrointestinal bleeding (Table 1).
ECG showed sinus tachycardia without conduction or repolarization abnormalities (Figures 1, 2).
Electrocardiogram on ICU day 1 showing sinus tachycardia (~150 bpm) without conduction or repolarization abnormalities with no ST-segment elevation or depressionQTc ~ 352 ms. Paper speed 25 mm/s, gain 10 mm/mV.Digital markers: arrows indicate regular P waves; calibration markers shown.ECG: electrocardiogram; QTc: corrected QT interval
Electrocardiogram on ICU day 1 showing sinus tachycardia (~150 bpm) without conduction or repolarization abnormalities with no ST-segment elevation or depressionQTc ~ 352 ms. Paper speed 25 mm/s, gain 10 mm/mV.Digital markers: arrows indicate regular P waves; calibration markers shown.ECG: electrocardiogram; QTc: corrected QT interval
Chest X-ray with mild-moderate alveolar infiltrates (Figure 3). At day 1, a transthoracic echocardiogram demonstrated a hyperdynamic left ventricle with preserved ejection fraction (65%) and normal right ventricular function.
Chest X-ray on ICU day 1 showing mild left-sided alveolar infiltrates
On ICU day 1, PaO₂/FiO₂ declined further, prompting initiation of prone positioning and neuromuscular blockade (cisatracurium). Despite lung-protective ventilation with FiO₂ 1.0, PEEP 8 cm H₂O, and tidal volume ~6 mL/kg PBW, the patient remained severely hypoxemic (PaO₂/FiO₂ 68). CT pulmonary angiography (Figures 4, 5) on day 4 revealed very distal subsegmental pulmonary embolism (SSPE) and mild posterior ground-glass opacities. These findings did not fully explain the respiratory compromise. Pulmonary hypertension was determined by pulmonary artery catheterization: systolic/diastolic PAP 68/39 mmHg, yielding a mean pulmonary arterial pressure (mPAP) of ≈49 mmHg ( \begin{document}\frac{sPAP + 2 \times dPAP}{3}\end{document} ). Pulmonary capillary wedge pressure (PCWP) was 18 mmHg. With a cardiac index of 4.19 L/min/m², the transpulmonary gradient (TPG) was ≈31 mmHg (mPAP − PCWP), and the diastolic pressure gradient (DPG) was ≈21 mmHg (dPAP − PCWP). Pulmonary vascular resistance (PVR) was ~6.2 Wood units (~495 dyn·s·cm⁻⁵). These values indicate elevated left-sided filling pressure with a substantial pre-capillary component (elevated TPG/DPG and PVR), consistent with combined post- and pre-capillary pulmonary hypertension in the acute setting. We therefore use “pulmonary hypertension” descriptively while emphasizing the prominent pulmonary vascular component.
CT pulmonary angiography (axial, lung window) on ICU day 4Mild posterior ground-glass opacities (boxes) with otherwise preserved aeration is seen. No proximal pulmonary arterial filling defects seen on this slice.Digital markers: boxes highlight ground-glass areas.CT = computed tomography; CTPA = CT pulmonary angiography
CT pulmonary angiography (coronal MIP, 10-mm slab) on ICU day 4Very distal SSPE (arrow) seen along a peripheral branch; central and lobar arteries are patent. Coronal MIP enhances visualization of small, contrast-opacified vessels.MIP: maximum intensity projection; SSPE: subsegmental pulmonary embolism
The patient progressed to multiorgan failure, including hepatic, renal, hematologic, and respiratory involvement. Coagulopathy, anemia, and thrombocytopenia worsened rapidly, culminating in death.
Discussion
This patient’s course after high-voltage electrocution is best explained by a vascular-dominant acute lung injury, where physiology outpaced imaging. Within hours of ROSC, PaO₂/FiO₂ fell to 68 despite protective ventilation and proning, while CT showed only mild posterior ground-glass change, and transthoracic echocardiography showed a preserved right ventricle. This discordance-profound hypoxemia with minimal parenchymal burden aligns with reports of primary endothelial injury in electrical trauma [1-3,7], and with broader forensic/clinical observations on electrocution pathophysiology [11,12]. Endothelial disruption can drive acute pulmonary vasoconstriction and loss of hypoxic vasoregulation, causing severe V/Q maldistribution (functional shunt) despite relatively intact alveoli [1-3,5,7,11]. A concurrent pro-coagulant milieu likely adds microthrombosis below routine CT resolution, coherently explaining the hemodynamics observed (PAP 68/39 mmHg, CI 4.19 L/min/m²) and the severity of gas-exchange failure.
The very distal SSPE detected on day 4 is unlikely to be the primary cause of hypoxemia. Contemporary guidance notes its limited hemodynamic impact in isolation and the need to balance anticoagulation against bleeding risk and competing diagnoses [9,10]. Here, the preserved RV function and scant parenchymal findings favor diffuse vascular dysfunction rather than macro-embolic physiology.
Management was framed by this vascular lens. Protective ventilation and prolonged proning remained foundational [4,5]. Where pulmonary hypertension and endothelial features predominate, a time-limited trial of inhaled vasodilators (nitric oxide/prostacyclins) is reasonable, with response tracked by PaO₂/FiO₂ and hemodynamics [6,7]. VV-ECMO should be considered when PaO2/FiO2 ≤100 persists despite optimization, per the Extracorporeal Life Support Organization (ELSO) principles and local capacity [8], consistent with acute respiratory distress syndrome (ARDS) escalation frameworks for refractory hypoxemia [13]. In our center, inhaled vasodilators and VV-ECMO were not available, which precluded their use despite physiologic rationale.
This report adds quantitative invasive hemodynamics to an under-recognized presentation--disproportionate hypoxemia with severe pulmonary hypertension and minimal imaging changes--supporting a primary pulmonary vascular injury after electrocution. Limitations include the absence of bronchoscopy with bronchoalveolar lavage (BAL), incomplete serial ventilatory/gas-exchange data, and the local unavailability of inhaled vasodilators and VV-ECMO. Even so, the synthesis of clinical, imaging, and hemodynamic signals provides a coherent, actionable narrative aligned with emerging evidence [1-3,4-10,13]. Our case differs from prior reports by demonstrating severe hypoxemia with minimal parenchymal change and no structural cardiac involvement, absence of explanatory macrothrombosis on CTPA, and detailed invasive hemodynamics (PAP 68/39 mmHg with a high/normal cardiac index) supporting a primary pulmonary vascular injury. The persistent sinus tachycardia despite correction of the usual triggers further underscores ongoing vascular stress rather than parenchymal flooding.
Clinical implications
The clinical implications of this study are: early hemodynamic profiling matters; don’t over-attribute refractory hypoxemia to distal SSPE; consider inhaled vasodilators as a diagnostic-therapeutic probe; and maintain a low threshold for ECMO triage in centers with capability.
Conclusions
High-voltage electrocution may present as a primary pulmonary vascular injury with hypoxemia and pulmonary hypertension out of proportion to imaging. Recognizing this phenotype has direct management implications--prompt hemodynamic assessment, avoidance of over-attribution to isolated distal SSPE, and consideration of time-limited trials of inhaled vasodilators with early VV-ECMO triage when hypoxemia remains refractory.
Beyond a single case, these observations encourage a pragmatic escalation pathway for similar presentations: (1) confirm severity with serial gas exchange and lung-protective ventilation; (2) evaluate for a vascular pattern using echocardiography and, when available, pulmonary artery catheterization; (3) where pulmonary hypertension predominates with minimal imaging burden, test nitric oxide or inhaled prostacyclins for physiologic response; and (4) if PaO2/FiO2 remains ≤100 or work of breathing is unsustainable, assess the transfer or initiation of VV-ECMO according to institutional capability and contemporary standards. Future studies should better define the incidence of pulmonary vascular phenotypes after electrical injury, elucidate biomarkers of endothelial damage, and determine which patients derive the greatest benefit from vasodilator therapy or extracorporeal support.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Isolated pulmonary injury following electric shock: a case report and literature review Ann Med Surg (Lond) Vu-Hoai N Dang-Vu T Lam-Quoc D Duong-Minh N Tran-Ngoc TH Tran-Ngoc N Nguyen-Dang K 167016778720254021318510.1097/MS 9.0000000000002875 PMC 11981285 · doi ↗ · pubmed ↗
- 2Isolated pulmonary hemorrhage after electric shock: a rare phenomenon Monaldi Arch Chest Dis Singh DK Pandey G Rizvi SH Singh PK 94202310.4081/monaldi.2023.251837522860 · doi ↗ · pubmed ↗
- 3High-voltage electrical lung injury Balkan Med J Čampar B BabićB 79804220253964834910.4274/balkanmedj.galenos.2024.2024-9-73PMC 11725673 · doi ↗ · pubmed ↗
- 4ESICM guidelines on acute respiratory distress syndrome: definition, phenotyping and respiratory support strategies Intensive Care Med Grasselli G Calfee CS Camporota L 7277594920233732664610.1007/s 00134-023-07050-7PMC 10354163 · doi ↗ · pubmed ↗
- 5Antithrombotic therapy for VTE disease. Compendium and review of CHEST guidelines 2012-2021 Chest Stevens SM Woller SC Baumann Kreuziger L 38840416620243845843010.1016/j.chest.2024.03.003 · doi ↗ · pubmed ↗
- 6Inhaled nitric oxide in patients with acute respiratory distress syndrome caused by COVID-19: treatment modalities, clinical response, and outcomes Ann Intensive Care Mekontso Dessap A Papazian L Schaller M 571320233736803610.1186/s 13613-023-01150-9PMC 10299982 · doi ↗ · pubmed ↗
- 7Inhaled nitric oxide improved refractory hypoxemia through attenuation of intrapulmonary shunt Am J Respir Crit Care Med Wang Y Zhong M 111420520223516741310.1164/rccm.202107-1598 IM · doi ↗ · pubmed ↗
- 8Management of adult patients supported with venovenous extracorporeal membrane oxygenation (VV ECMO): guideline from the Extracorporeal Life Support Organization (ELSO)ASAIO J Tonna JE Abrams D Brodie D Greenwood JC Rubio Mateo-Sidron JA Usman A Fan E 6016106720213396597010.1097/MAT.0000000000001432 PMC 8315725 · doi ↗ · pubmed ↗