A case of polydactylous nail changes and BAP1-tumor predisposition syndrome: Implications for earlier detection
Lucy Wang, Hasret Gunduz, June Y. Moon, Kenneth Shulman, Mehmet Fatih Atak, Banu Farabi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
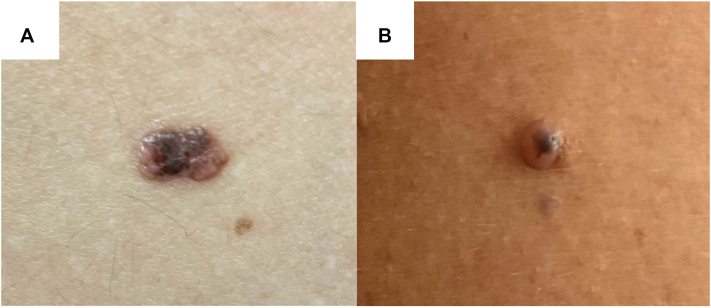 Figure 1
Figure 1 Figure 2
Figure 2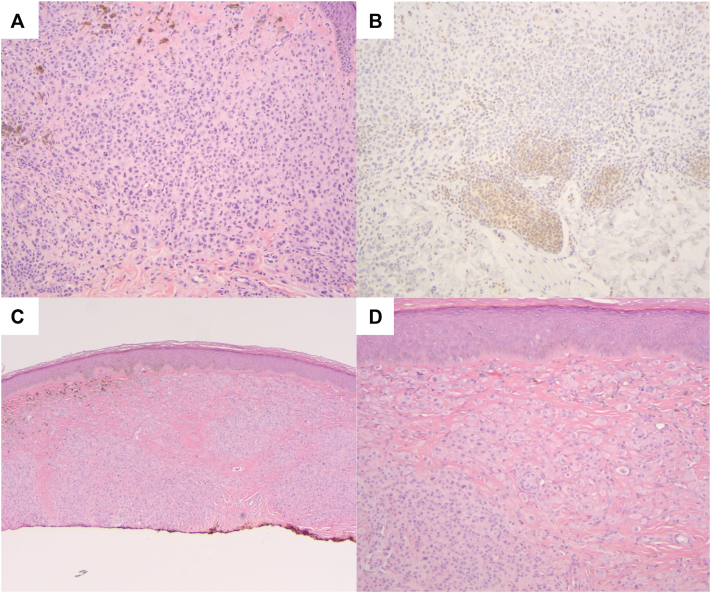 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDupuytren's Contracture and Treatments · Vascular Malformations and Hemangiomas · Dermatological and Skeletal Disorders
Introduction
BRCA1-associated protein (BAP1) tumor predisposition syndrome (BAP1-TPDS) is a cancer syndrome caused by loss-of-function variants in the BAP1 tumor suppressor gene. Although typically acquired in an autosomal dominant pattern, de novo pathogenic variants can also occur, resulting in disease in individuals without an affected parent.1 BAP1-TPDS increases susceptibility to various benign and malignant tumors, including BAP1-inactivated melanocytic tumors (BIMTs), uveal melanoma (UM), malignant mesothelioma (MMe), cutaneous melanoma (CM), and renal cell carcinoma (RCC).2 Although BIMTs are often the earliest clinical sign of BAP1-TPDS, polydactylous onychopapillomas have recently been identified as another unique diagnostic clue.3 We present a patient whose long-standing polydactylous nail changes, suggestive of onychopapillomas, represented a potential opportunity for earlier recognition of BAP1-TPDS.
Case presentation
A 43-year-old male with multiple congenital nevi presented to our clinic for monitoring of an asymmetric 7 mm by 4 mm light-to dark-brown papule on the lower back that had been noticeable for the past 7 years (Fig 1, A). He denied any changes or symptoms related to the lesion since the last visit; however, a blue-white veil was observed on dermoscopy, and a shave biopsy was performed to rule out malignant melanoma. A dome-shaped, skin-colored papule with asymmetric black pigment was later found on his right shoulder and biopsied (Fig 1, B). Following a total body skin examination, nail abnormalities were noted, which the patient reported having since childhood. Specifically, clinical and dermoscopic examination revealed longitudinal leukonychia, V-shaped onycholysis, distal fissuring, and distal subungual hyperkeratotic papules on multiple fingernails and the left first digit toenail (Fig 2). The clinical presentation of these lesions was strongly suggestive of polydactylous onychopapillomas; however, a biopsy for histopathologic confirmation was deferred while awaiting the results from the skin biopsies.Fig 1. Clinical presentation of BAP1-inactivated melanocytic tumors (BIMTs) on the (A) lower back and (B) right shoulder.Fig 2. Presentation of polydactylous onychopapillomas. Clinical images of onychopapillomas involving (A) multiple fingernails and (B) the left first-digit toenail. Dermoscopic images of the (C) fingernail with subungual hyperkeratosis, longitudinal leukonychia, and onycholysis, and (D) toenail with a subungual hyperkeratotic papule corresponding to overlying longitudinal leukonychia and V-shaped onycholysis.
The results of the lower back lesion shave biopsy revealed a BAP1-deficient intradermal melanocytic nevus. Immunohistochemistry (IHC) showed BAP1 expression in small nevus cells but deficient or absent BAP1 expression in the larger epithelioid melanocytes (Fig 3). A combined Ki67 and Melan-A stain showed minimal proliferative activity (∼2%), and an HMB45 stain was focally reactive in the superficial component and negative in the majority of the lesion. The biopsy of the right shoulder papule demonstrated a combined melanocytic nevus, consisting of a conventional nevus component and epithelioid melanocytes with loss of BAP1 expression by IHC. The lesions were consistent with BIMTs and completely excised.Fig 3. Histopathologic images of the BIMT. A, Nodular proliferation of enlarged epithelioid melanocytes with nuclear pleomorphism and amphophilic cytoplasm (H&E, 10×). B, BAP1 immunostain demonstrates loss of BAP1 expression in enlarged epithelioid melanocytes with retained expression in small melanocytes at the base of the lesion (10×). C, Nodular intradermal proliferation of enlarged epithelioid melanocytes (H&E, 10×), (D) with nuclear pleomorphism and amphophilic cytoplasm (H&E, 20×).
The patient was referred to the Genetics Department, and genetic testing with direct sequencing revealed a heterozygous pathogenic loss-of-function variant in BAP1 exon 4 (NM_004656.4:c.189_198del, p.Thr64Metfs∗5), confirming BAP1-TPDS. Concurrently, a detailed family history was assessed and was not consistent with a hereditary pathogenic variant in the BAP1 gene, suggesting a de novo variant. He was counseled on annual screening for associated malignancies, including ophthalmologic and total-body skin examinations (TBSE), abdominal imaging with ultrasound or magnetic resonance imaging (MRI), and clinical evaluation for MMe or other malignancies.
Discussion
BAP1-TPDS results from germline pathogenic variants of the BAP1 gene encoding for the ubiquitin carboxy-terminal hydrolase BAP1. Initially identified for its role in BRCA1 regulation,4 BAP1 is now known as an independent tumor suppressor involved in DNA damage repair, cell cycle regulation, and cell growth.5 Affected individuals develop CM, UM, MMe, and RCC at a higher frequency and younger age than the general population. Early detection of BAP1-TPDS is crucial as it enables the implementation of targeted cancer surveillance for at-risk individuals. Current recommendations include annual physical examination for symptoms of MMe, TBSE for dermatologic malignancies beginning at age 18-20, and ophthalmologic examinations beginning at age 11-16. Screening for RCC may include annual abdominal ultrasound with biennial MRI or alternating biennial abdominal MRI and ultrasound beginning at age 30.2 These screenings maximize early detection and treatment of malignancy. Indeed, identification and treatment of UM when small and localized has been shown to significantly improve prognosis.6 The presence of BAP1-TPDS may also inform treatment approach, since studies have suggested worse survival with UM, CM, and RCC, but better survival with MMe when associated with BAP1-TPDS.2
As with our patient, individuals often present initially with BIMTs, allowing for BAP1-TPDS evaluation before the development of associated malignancies. These dome-shaped, skin-colored or pink papules typically appear on the head, neck, trunk, and upper extremities. Histologically, BIMTs are intradermal or junctional nevi with BAP1-negative epithelioid dermal melanocytes, making them key indicators for BAP1-TPDS evaluation. However, these lesions often go unbiopsied due to their inconspicuous appearance.
With increasing awareness of their association with BAP1-TPDS, polydactylous onychopapillomas may represent another cutaneous marker for the syndrome.3 Onychopapilloma presents as longitudinal erythronychia and distal subungual hyperkeratosis, with other features including longitudinal leukonychia and melanonychia, splinter hemorrhages, onycholysis, and distal fissuring.7 While most cases involve a single digit, a recent study found onychopapillomas in 83% (39/47) of BAP1-TPDS patients, with 97% (38/39) showing polydactylous involvement.3 Additionally, longitudinal leukonychia was more common than longitudinal erythronychia in BAP1-TPDS, differing from the general population.3^,^7 In patients with suspected polydactylous onychopapillomas, careful exclusion of additional cutaneous and systemic findings can distinguish them from other conditions that have polydactylous longitudinal leukonychia (eg, Hailey-Hailey disease, tuberous sclerosis complex)3 or polydactylous longitudinal erythronychia (eg, Darier disease, lichen planus).8 Ultimately, histopathology confirms the diagnosis and should subsequently prompt BAP1-TPDS testing.
Although our patient was diagnosed with BAP1-TPDS following identification of BIMTs, the presence of nail changes highly suggestive of polydactylous onychopapillomas preceding the onset of BIMTs highlights a case in which recognition of this association may have led to earlier detection and surveillance. Thus, we emphasize the importance of the emerging association between polydactylous onychopapillomas and BAP1-TPDS. Clinicians should maintain a high index of suspicion for BAP1-TPDS when polydactylous onychopapillomas are suspected or confirmed, especially in patients with multiple nevi or atypical melanocytic lesions.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chau C.van Doorn R.van Poppelen N.M.Families with BAP 1-tumor predisposition syndrome in the Netherlands: path to identification and a proposal for genetic screening guidelines Cancers 118201911143138269410.3390/cancers 11081114 PMC 6721807 · doi ↗ · pubmed ↗
- 2Lalloo F.Kulkarni A.Chau C.Clinical practice guidelines for the diagnosis and surveillance of BAP 1 tumour predisposition syndrome Eur J Hum Genet 31112023126112693760798910.1038/s 41431-023-01448-z PMC 10620132 · doi ↗ · pubmed ↗
- 3Lebensohn A.Ghafoor A.Bloomquist L.Multiple onychopapillomas and BAP 1 tumor predisposition syndrome JAMA Dermatol 160820248388453875922510.1001/jamadermatol.2024.1804 PMC 11102040 · doi ↗ · pubmed ↗
- 4Jensen D.E.Proctor M.Marquis S.T.BAP 1: a novel ubiquitin hydrolase which binds to the BRCA 1 RING finger and enhances BRCA 1-mediated cell growth suppression Oncogene 169199810971112952885210.1038/sj.onc.1201861 · doi ↗ · pubmed ↗
- 5Walpole S.Pritchard A.L.Cebulla C.M.Comprehensive study of the clinical phenotype of germline BAP 1 variant-carrying families worldwide J Natl Cancer Inst 110122018132813413051773710.1093/jnci/djy 171PMC 6292796 · doi ↗ · pubmed ↗
- 6Hussain R.N.Coupland S.E.Kalirai H.Small high-risk uveal melanomas have a lower mortality rate Cancers 139202122673406684210.3390/cancers 13092267 PMC 8125943 · doi ↗ · pubmed ↗
- 7Tosti A.Schneider S.L.Ramirez-Quizon M.N.Zaiac M.Miteva M.Clinical, dermoscopic, and pathologic features of onychopapilloma: a review of 47 cases J Am Acad Dermatol 74320165215262651817310.1016/j.jaad.2015.08.053 · doi ↗ · pubmed ↗
- 8Curtis K.L.Ho B.Jellinek N.J.Rubin A.I.Tosti A.Lipner S.R.Diagnosis and management of longitudinal erythronychia: a clinical review by an expert panel J Am Acad Dermatol 91320244804893870519710.1016/j.jaad.2024.04.032 · doi ↗ · pubmed ↗