Challenges and Limitations of Sequential MET ‐ TKI Therapy in METex14 ‐ Positive NSCLC With a Focus on Non‐ ILD Toxicities: A Case Report
Akina Nigi, Toshikazu Kumasa, Keisuke Iwamoto, Hidetoshi Itani, Shigeto Kondou, Junji Uraki

TL;DR
This case report explores the challenges of using three different MET tyrosine kinase inhibitors in a patient with METex14-positive lung cancer, highlighting non-ILD toxicities.
Contribution
This is the first reported case of sequential use of all three MET-TKIs approved in Japan for METex14-positive NSCLC.
Findings
Sequential treatment with tepotinib, capmatinib, and gumarontinib was interrupted due to non-ILD toxicities.
Each MET-TKI exhibited distinct toxicity profiles, suggesting rechallenge may be viable with personalized risk assessment.
Toxicities varied between agents, emphasizing the need for careful monitoring in sequential therapy.
Abstract
Nonsmall cell lung cancer (NSCLC) with mesenchymal‐epithelial transition exon 14 skipping mutation (METex14) represents a distinct molecular subtype with limited therapeutic options. Selective MET tyrosine kinase inhibitors (MET‐TKIs) such as tepotinib, capmatinib, and gumarontinib have improved outcomes, but toxicities frequently limit their use. Previous case reports have described sequential rechallenge with two MET‐TKIs and, in rare cases, with three agents including an investigational drug. To our knowledge, this is the first reported case worldwide of sequential treatment with all three MET‐TKIs currently approved in Japan—tepotinib, capmatinib, and gumarontinib. We report a 72‐year‐old man with METex14‐positive NSCLC who underwent surgery and adjuvant chemotherapy, later developing pleural dissemination. Tepotinib was discontinued after 2 months due to Grade 3 interstitial lung…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
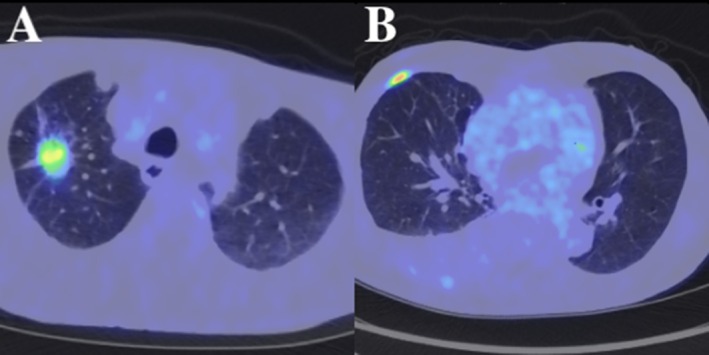 FIGURE 1
FIGURE 1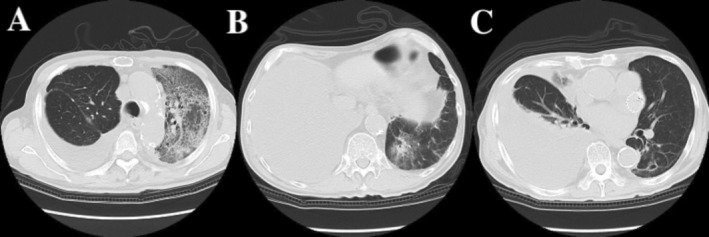 FIGURE 2
FIGURE 2| Date | Event/treatment | Notes/duration |
|---|---|---|
| 2022 early February | Right upper lobectomy + lymph node dissection |
StageIIA No LN metastasis |
| 2024 mid January | Recurrence: right pleural dissemination | METex14 skipping positive, PD‐L1 10% |
| 2024 late February | Tepotinib 500 mg daily | |
| 2024 early May | Discontinued after 69 days due to ILD; improved with steroids | |
| 2024 early July | CBDCA + pemetrexed ×3 cycles → pembrolizumab added | Temporary response; later progression with pleural effusion |
| 2024 late September | Disease progression | Effusion, tumor growth |
| 2024 early October | Capmatinib started | Discontinued after 10 days due to fever |
| 2024 late October | Docetaxel + ramucirumab | Six cycles given |
| 2025 late March | Gumarontinib started | Discontinued after 36 days due to hepatotoxicity |
| 2025 late April | Gumarontinib restarted (150 mg/day) | Discontinued after 57 days due to edema and renal impairment |
| 2025 late August—present | CBDCA + pemetrexed + bevacizumab | Ongoing chemotherapy regimen |
| Capmatinib | Tepotinib | Gumarontinib | |
|---|---|---|---|
| Major adverse events | Edema, dysgeusia, liver dysfunction | Edema, liver dysfunction, loss of appetite | Liver dysfunction, fever |
| Reported frequency of ILD | 2%–3% | 6% | 1.2% |
| Incidence of edema | 51% | 70% | 10% |
| Incidence of liver dysfunction | 20% | 26% | 30% |
| Mucosal and taste disorders | Frequent | Rare | Rare |
| Discontinuation rate | 10% | 7%–10% | 5%–10% |
| Study (Author) | Treatment sequence TKI | Initial/second TKI toxicity | PDL1 | Observation period | TKI duration (days) | Toxicities during rechallenge |
|---|---|---|---|---|---|---|
| Kashizaki et al. [ |
Investigationaldrug (MET‐TKI) Tepotinib Capmatinib | Maculopapular rash/same | 1%–4% | 24 months | 11/8/30 | Unknown |
| Kunimasa et al. [ |
Tepotinib Capmatinib | Peripheral edema Grade 3 | 60% | 36 months | 14/100 | Unremarkable |
| Tseng et al. [ |
Capmatinib Investigational drug(MET‐TKI) Tepotinib | ILD Grade 3/tumor progression | Negative | 5 months | 30/14/30 | None except tumor progression |
| Hashiguchi et al. [ |
Capmatinib Tepotinib | ILD Grade 2 | 90% | 4 years 7 months | 6/180 | |
| Current case |
Tepotinib Capmatinib Gumarontinib | ILD Grade 3/fever Grade 3 | 10% | 20 months | 60/10/36 + 57 | Hepatotoxity Grade 2 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Lung Cancer Diagnosis and Treatment · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis
Introduction
1
Nonsmall cell lung cancer (NSCLC) harboring mesenchymal‐epithelial transition exon 14 skipping mutations (METex14) represents a distinct molecular subtype, comprising approximately 3% of all NSCLC cases. Without targeted therapy, this subtype is associated with poor prognosis. Use of selective MET tyrosine kinase inhibitors (TKIs) such as tepotinib and capmatinib has significantly improved patient outcomes. In pivotal trials, the median overall survival was 17.1 months with tepotinib and 21.5 months with capmatinib [1, 2].
Although MET‐TKI‐induced interstitial lung disease (ILD) is uncommon, with an incidence of 3%–6% in clinical trials, it can be severe enough to negatively limit treatment. Other adverse events, including rash, edema, and hepatotoxicity, are more common and may also lead to discontinuation.
Several case reports have described successful rechallenge with different MET‐TKIs after resolution of ILD [3, 4, 5, 6]. However, data on sequential MET‐TKI treatment following multiple toxicities are limited. The effects of chemotherapy and immune checkpoint inhibitors (ICIs) on subsequent MET‐TKI are unclear. There are reports that MET‐TKI after ICI increases adverse events.
Herein, we present the case of a patient with METex14‐positive NSCLC who sequentially received tepotinib, capmatinib, and gumarontinib, each associated with distinct toxicities, leading to treatment discontinuation. By comparing four previously reported cases, we argue that non‐ILD toxicities may pose a more significant barrier to durable rechallenge than previously recognized.
Case Presentation
2
In March 2022, a 72‐year‐old Japanese man was diagnosed and treated at the Japanese Red Cross Ise Hospital (Mie, Japan). He had a history of atrial fibrillation and hypertension, both diagnosed over 5 years prior and well‐controlled with medication. The patient underwent a right upper lobectomy with systematic mediastinal and hilar lymph node dissection, including stations 2R, 4R, 10R, 11R, and 12R, for stage IIA (pT2aN0M0) lung adenocarcinoma (Figure 1A).
Initial diagnosis and disease recurrence. (A) Base line PET‐CT imaging prior to initial surgery demonstrating a fluorodeoxyglucose (FDG)‐avid lesion in the right upper lobe, consistent with primary lung adenocarcinoma. (B) Follow‐up chest CT approximately 22 months postoperatively, showing pleural dissemination suggestive of disease recurrence.
Postoperative molecular profiling in April 2022 revealed a MET exon 14 skipping mutation, with EGFR, ALK, and ROS1 mutations negative. The PD‐L1 tumor proportion score was 10%. The patient received oral tegafur‐uracil (UFT) as adjuvant chemotherapy, planned for 2 years. In January 2024, routine imaging revealed pleural dissemination (Figure 1B). UFT was discontinued, and tepotinib (500 mg/day) was initiated. Two months after starting tepotinib, in March 2024, the patient developed fatigue and dyspnea. Chest CT showed diffuse ground‐glass opacities in the left lung (Figure 2A), and he was diagnosed with Grade 3 ILD. Bronchoscopy with bronchoalveolar lavage fluid was not performed because the patient's respiratory condition required urgent initiation of corticosteroid therapy. The diagnosis was therefore made based on clinical presentation and radiological findings.
Imaging of adverse events during sequential MET‐TKI therapy. (A) Diffuse ground‐glass opacities in the left lung observed on CT after 2 months of tepotinib therapy, consistent with Grade 3 drug‐induced ILD. (B) Newly developed ground‐glass opacities after 10 days of capmatinib therapy, raising suspicion of ILD (Grade 1). (C) Chest CT on Day 36 of gumarontinib therapy. No ILD findings were observed, although right pleural effusion was present. Gumarontinib was discontinued due to Grade 2 hepatotoxicity.
Treatment was initiated with steroid pulse therapy (methylprednisolone 1000 mg/day for 3 days), followed by oral prednisolone (5 mg/day) and tacrolimus (0.5 mg/day). Resolution of CT findings and symptom improvement confirmed treatment efficacy. After ILD recovery in May 2024, confirmed by imaging and clinical improvement, the patient underwent two cycles of carboplatin plus pemetrexed, followed by two cycles of pembrolizumab in combination, and then four cycles of pembrolizumab monotherapy. However, in October 2024, increased pleural effusion and dyspnea were noted, and disease progression was assessed. In November 2024, capmatinib was started, but discontinued on Day 10 due to high‐grade fever (39°C), oral ulcers, and new ground‐glass opacities (Figure 2B), raising suspicion of Grade 1 possible ILD. This was followed by six cycles of docetaxel (DTX) and ramucirumab (Ram) between December 2024 and April 2025, which resulted in temporary disease control. Subsequently, due to recurrent pleural effusion, gumarontinib (300 mg/day) was initiated in May 2025. On Day 36 of gumarontinib treatment (June 2025), the patient experienced fatigue, and laboratory tests revealed Grade 2 hepatotoxicity (AST 92 IU/L, ALT 92 IU/L), leading to temporary discontinuation. Although right pleural effusion was present, no evidence of ILD was observed on CT (Figure 2C). After recovery of liver function, treatment was resumed at a reduced dose of 150 mg/day. No hepatic dysfunction was observed on testing 2 weeks after resumption. After an additional 57 days of treatment, in August 2025, gumarontinib was discontinued due to renal dysfunction and edema. Subsequently, the patient was maintained on carboplatin plus pemetrexed and bevacizumab, which is ongoing at the time of this report. The clinical course is outlined in Table 1 for clarity. The severity of events was graded according to the Common Terminology Criteria for Adverse Events (CTCAE), version 5.0.
Discussion
3
Gumarontinib, a selective MET tyrosine kinase inhibitor (TKI) developed in China, is the third MET‐TKI approved in Japan for the treatment of NSCLC harboring MET exon 14 skipping alterations. Alongside tepotinib and capmatinib, it is considered one of the key targeted therapies for MET exon 14 altered NSCLC.
Although MET‐TKIs demonstrate substantial therapeutic efficacy, treatment discontinuation due to adverse events remains a significant clinical challenge. ILD is particularly notable as a severe adverse event, with reported incidence rates of 6.1% in the VISION trial for tepotinib and 4.5% in the GEOMETRY mono‐1 trial for capmatinib. Among Japanese patients, the ILD incidence rose to 8.3% [1, 2]. In contrast, gumarontinib was primarily associated with hepatotoxicity, and the ILD incidence was reported at 1.2% [7]. While direct comparison is difficult due to differences in patient backgrounds, observation periods, and evaluation criteria across trials, these data offer useful guidance for clinical decision‐making. Table 2 summarizes these outcomes. Notably, ILD was not the most frequent cause of treatment discontinuation.
In pivotal trials, the median overall survival was 17.1 months with tepotinib and 21.5 months with capmatinib [1, 2].
Recent case reports have demonstrated the potential efficacy of MET‐TKI rechallenge after resolution of ILD [3, 4, 5, 6]. This approach holds clinical value as a strategy to overcome resistance or for patients with limited therapeutic options. In the context of EGFR‐TKIs, rechallenge with a different TKI following discontinuation due to adverse effects has been shown to improve overall survival [8], suggesting the potential utility of a similar strategy for MET‐TKIs. However, in clinical practice, non‐ILD adverse events—such as skin rash, fatigue, peripheral edema, and liver dysfunction—often lead to treatment discontinuation within 1–3 months, making long‐term rechallenge difficult. In this case, treatment with tepotinib was discontinued due to Grade 3 ILD, while both capmatinib and gumarontinib had to be discontinued shortly thereafter due to non‐ILD toxicities (fever, mucositis, fatigue, and hepatotoxicity).
Reports by Hasnibuchi et al. and Yasuda et al. also noted that while ILD recurrence was not observed, non‐ILD toxicities were the main barrier to sustained rechallenge [9, 10]. Among rechallenge cases, long‐term continuation was only achieved in the report by Hashiguchi et al. (approximately 180 days), with most other cases discontinued within 10–90 days (Table 3). Table 3 summarizes five MET‐TKI rechallenge cases, including ours. The full treatment history, including chemotherapy and immunotherapy, is shown in Table S3. Although higher PD‐L1 expression may be associated with longer response duration, NSCLCs with MET exon 14 skipping mutations tend to exhibit high PD‐L1 but low TMB, making them generally less responsive to ICIs [11].
The reproducibility of toxicity across MET‐TKIs may be attributed to their shared pharmacological properties. Tepotinib, capmatinib, and gumarontinib are all reversible, Type I ATP‐competitive inhibitors. Although structurally distinct from agents such as EGFR‐TKIs, they may share a class‐related toxicity profile [12]. However, adverse events are not universally repeated in every patient; notably, none of the five documented cases, including the present case, experienced ILD recurrence, suggesting that MET‐TKI rechallenge may be a viable option in carefully selected patients, although no definitive conclusions can be drawn from this limited sample. Interindividual differences in adverse reactions may be explained by multiple interacting factors, including tissue distribution of the drugs, plasma concentrations, metabolic pathways (e.g., CYP3A4, UGT1A1), immune response variability, and prior treatment‐induced tissue sensitization [13].
Previous use of ICIs or combination chemotherapy may alter immune and metabolic environments, potentially lowering the threshold for TKI‐related toxicity. Indeed, one report found that the incidence of grade ≥ 3 adverse events increased to 27% when MET‐TKIs were administered after ICIs [14, 15], underscoring the importance of risk assessment based on treatment history. In this case [15], although 6 months had passed between the last pembrolizumab dose and gumarontinib rechallenge, non‐ILD toxicities still emerged, suggesting that ICI‐induced effects may persist even after prolonged intervals.
To our knowledge, this is the first report describing gumarontinib treatment in a patient with prior discontinuation of both tepotinib and capmatinib (based on a PubMed search as of April 2025). Although these MET‐TKIs share similar pharmacologic mechanisms, the pattern of adverse events may differ, and non‐ILD toxicities appear to be the most significant limitation to continued treatment.
Rechallenge with MET‐TKIs, when guided by careful assessment of toxicity risks, may offer a viable strategy, especially for patients whose prior discontinuation was due to adverse effects. Although the treatment duration was limited in this case, sequential administration of multiple TKIs enabled cumulative disease control, offering clinically relevant insight into the balance between therapeutic benefit and toxicity risk.
Moving forward, accumulation of more clinical cases and prospective trials will be critical to evaluate the safety and efficacy of rechallenge strategies. Additionally, identifying predictive biomarkers for toxicity, elucidating the link with immune‐environmental changes, and developing risk stratification models that consider treatment history are essential next steps.
Conclusion
4
This case represents the first report of sequential use of all three MET‐TKIs currently approved in Japan and highlights both the challenges and the potential of MET‐TKI rechallenge therapy.
In this patient, treatment discontinuation was not due to recurrent ILD but rather to distinct non‐ILD toxicities associated with each agent.
These findings suggest that toxicity profiles vary among MET‐TKIs and that rechallenge may remain feasible with careful monitoring and individualized risk assessment.
Further accumulation of clinical data and identification of predictive biomarkers will be essential to define safe conditions for MET‐TKI rechallenge in the future.
Limitations
5
This report describes a single patient, which limits the generalizability of the findings. In addition, pharmacokinetic analyses and mechanistic biomarkers were not available, precluding definitive differences in toxicity among sequential MET‐TKIs.
Author Contributions
A.N. contributed significantly to the clinical management of the patients, study conception, and manuscript writing. T.K., K.I., H.I., and J.U. are also involved in clinical practice. H.I. and S.K. contributed to pathological examination and case review. All authors reviewed the final draft of the manuscript and approved its submission.
Funding
The authors have nothing to report.
Ethics Statement
This study was conducted in accordance with the ethical standards of the institution.
Consent
Written informed consent was obtained from the patient for participation and publication of this case report and any accompanying images. Ethics committee approval was not required for this single‐patient case report.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Table S3: Comprehensive treatment histories of the reported cases, including MET‐TKIs, chemotherapy, and immune checkpoint inhibitors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. Wolf , T. Seto , J. Y. Han , et al., “Capmatinib in MET Exon 14–Mutated or MET‐Amplified Non–Small‐Cell Lung Cancer,” New England Journal of Medicine 383 (2020): 944–957, 10.1056/NEJ Moa 2002787.32877583 · doi ↗ · pubmed ↗
- 2P. K. Paik , E. Felip , R. Veillon , et al., “Tepotinib in Non–Small‐Cell Lung Cancer With MET Exon 14 Skipping Mutations,” New England Journal of Medicine 383 (2020): 931–943, 10.1056/NEJ Moa 2004407.32469185 PMC 8422679 · doi ↗ · pubmed ↗
- 3F. Kashizaki , S. Okazaki , N. Tsuchiya , H. Chen , H. Koizumi , and K. Takahashi , “Effective Treatment of MET Exon 14 Skipping Mutation‐Positive Non‐Small Cell Lung Cancer Using Capmatinib Following Serious Maculopapular Rash Caused by Two MET Inhibitors: A Case Report,” AME Case Reports 8 (2024): 42, 10.21037/acr-23-181.38711889 PMC 11071010 · doi ↗ · pubmed ↗
- 4K. Kunimasa , T. Kawamura , M. Tamiya , et al., “Capmatinib Successfully Overcomes Tepotinib‐Induced Intolerable Peripheral Edema,” Thoracic Cancer 12, no. 24 (2021): 3426–3428, 10.1111/1759-7714.14205.34695875 PMC 8671889 · doi ↗ · pubmed ↗
- 5L. W. Tseng , J. W. Chang , and C. E. Wu , “Safety of Tepotinib Challenge After Capmatinib‐Induced Pneumonitis in a Patient With NSCLC Harboring MET Exon 14 Skipping Mutation: A Case Report,” International Journal of Molecular Sciences 23, no. 19 (2022): 11809, 10.3390/ijms 231911809.36233109 PMC 9570266 · doi ↗ · pubmed ↗
- 6M. H. Hashiguchi , T. Sato , H. Yamamoto , et al., “Successful Tepotinib Challenge After Capmatinib‐Induced Interstitial Lung Disease in a Patient With Lung Adenocarcinoma Harboring MET Exon 14 Skipping Mutation: Case Report,” JTO Clinical and Research Reports 3, no. 2 (2021): 100271, 10.1016/j.jtocrr.2021.100271.35252894 PMC 8888201 · doi ↗ · pubmed ↗
- 7Y. Zhang , Y. Wang , L. Li , et al., “Safety and Efficacy of Gumarontinib in NSCLC: Phase I/II Trial,” Cancer Chemotherapy and Pharmacology 90 (2022): 821–829, 10.1007/s 00280-022-04480-6. · doi ↗
- 8K. Sonehara , K. Tateishi , K. Yoh , et al., “Real‐World Study of EGFR‐TKI Rechallenge With Another TKI After First‐Line Osimertinib Discontinuation in Patients With EGFR‐Mutated NSCLC: A Subset Analysis of the Reiwa Study,” Thoracic Cancer 16, no. 2 (2025): e 15507, 10.1111/1759-7714.15507.39644181 PMC 11735459 · doi ↗ · pubmed ↗