Case report: preoperative radiological suspicion of atypical meningioma: A diagnostic challenge
Raisa Mahmudah, Namira Ammarin, Tasiya Ocvianty

TL;DR
This case report highlights the challenges in diagnosing an atypical meningioma using MRI before surgery.
Contribution
The report emphasizes the importance of advanced MRI techniques in preoperative identification of atypical meningiomas.
Findings
MRI features like cystic components and heterogeneous enhancement suggested an atypical meningioma.
Histopathological analysis confirmed the preoperative MRI suspicion of atypical meningioma.
Comprehensive MRI aids in surgical planning and decisions about adjuvant therapy.
Abstract
Atypical meningiomas represent a minority of intracranial meningiomas yet carry more aggressive biological behavior and higher recurrence rates, making preoperative differentiation essential for optimal management. We report a 56-year-old female presenting with progressive headaches, drowsiness, and vomiting, with no focal neurological deficits. Brain Magnetic Resonance Imaging (MRI) revealed a dural-based lesion at the posterior falx with cystic components, irregular margins, heterogeneous enhancement, disproportionate peritumoral edema, all suggesting atypicality. Subtotal resection followed by histopathological analysis confirmed a atypical meningioma. This case underscores the pivotal role of comprehensive MRI—including conventional sequences and advanced techniques—in identifying features of atypical meningioma even without definitive brain invasion, thereby guiding appropriate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
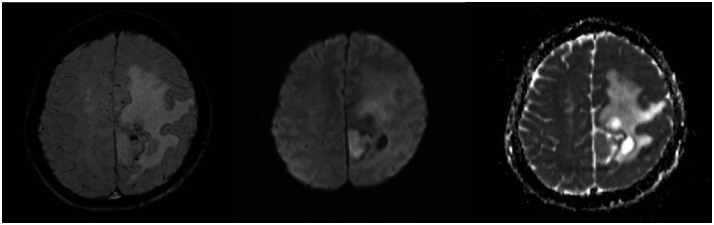 Figure 1
Figure 1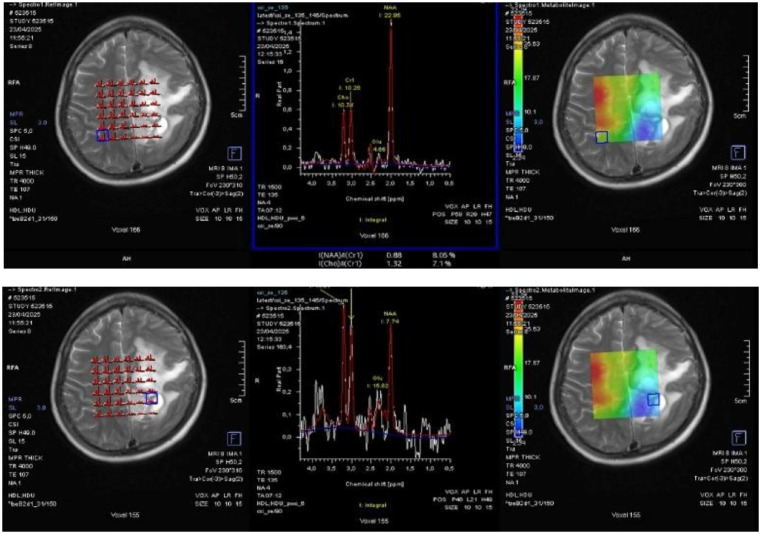 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMeningioma and schwannoma management · Glioma Diagnosis and Treatment · Neurofibromatosis and Schwannoma Cases
Introduction
Meningiomas are among the most common primary intracranial tumors. The majority are benign, but a significant proportion (5%-15%) are classified as atypical, exhibiting a more aggressive biological behavior and higher recurrence rates [1,2]. Preoperative differentiation between benign and atypical meningiomas is clinically significant, impacting surgical strategy and the potential need for adjuvant therapies. Neuroimaging, particularly advanced MRI techniques, has become crucial in identifying subtle characteristics that may suggest a higher grade. This report illustrates a case where comprehensive radiological assessment provided strong preoperative evidence for an atypical meningioma, despite the lack of clear brain invasion, at our institution in Bandung, Indonesia.
Case presentation
A 56-year-old female presented to the Neurosurgery Outpatient Clinic at Dr Hasan Sadikin General Hospital, Bandung. The primary complaints were progressively worsening headaches over the past one year, which had become constant and severe in the one weeks prior to presentation. The patient appeared drowsy, Glasglow Coma Scale (GCS) was 11. The complaint was also accompanied by two episodes of vomiting. There was no history of limb weakness, seizures, slurred speech, facial asymmetry, behavioral changes, or fever. Motor examination showed no evidence of lateralization. Sensory examination revealed a response to painful stimuli. Physiological reflexes were present bilaterally, and the Babinski reflex was negative on both sides. Initial laboratory investigations were within normal limits. A comprehensive Magnetic Resonance Imaging (MRI) scan of the brain with intravenous gadolinium contrast was subsequently performed a dural-based lesion in the posterior falx cerebri with surrounding cystic components, irregular margins, the lesion partly gives restricted diffusion on Diffusion-Weighted Imaging - Apparent Diffusion Coefficient (DWI-ADC), giving blooming artifacts on Susceptibility-Weighted Imaging (SWI) (Fig. 1). Post-contrast gives strong enhancement. MR spectroscopy demonstrated elevated choline ratio with decreased N-Acetylaspartate (NAA) (Fig. 2). These findings raised suspicion for an atypical meningioma, which was histopathologically confirmed as a World Health Organization (WHO) grade II (atypical) meningioma after subtotal resection [3].Fig. 1MRI of an atypical meningioma demonstrating areas of susceptibility on SWI (left), diffusion restriction on DWI (center), and corresponding low signal on the ADC map (right).Fig 1. Fig. 2MR spectroscopy shows elevated choline ratio with decreased NAA.Fig 2
Discussion
This case highlights the valuable contribution of advanced radiological imaging in differentiating atypical meningiomas from their more common benign counterparts, even in the absence of definitive brain invasion. Preoperative identification of features suggestive of atypicality is critical for optimal patient management.
Conventional MRI sequences offered more granular detail. The heterogeneous enhancement observed on post-contrast T1-weighted images, a deviation from the typical homogeneous enhancement of benign meningiomas, was a significant finding pointing towards atypicality [4]. The disproportionate peritumoral edema on T2-weighted imaging was another prominent feature, strongly correlating with higher tumor grade and increased permeability of the tumor vasculature [5]. While clear brain invasion was not definitively seen, the focally irregular tumor-brain interface still raised a degree of suspicion regarding aggressive growth. The presence of prominent intralesional flow voids also suggested increased vascularity often seen in higher-grade tumors.
The advanced MRI techniques were particularly informative. DWI and ADC maps demonstrating restricted diffusion within the tumor are highly indicative of increased cellularity, a core feature of atypical and anaplastic meningiomas [6,7]. These quantitative imaging biomarkers offer objective data that complement subjective visual assessment.
Despite the absence of definitive brain invasion on imaging or confirmed histologically, the combination of extensive peritumoral edema, heterogeneous enhancement, collectively pointed towards a high probability of atypical meningioma. This comprehensive radiological assessment enabled the neurosurgical team to be well-prepared for a potentially more aggressive tumor, influencing the extent of resection planned and prompting the discussion of adjuvant radiotherapy postoperatively. Even with gross total resection, the atypical grade itself warrants consideration of adjuvant therapy due to the elevated recurrence risk [8].
Conclusion
This case emphasizes that atypical meningiomas often manifest distinct radiological features, even without overt brain invasion. A meticulous evaluation using conventional MRI, coupled with advanced techniques such as DWI/ADC, can provide crucial preoperative insights into tumor grade, alerting clinicians to the possibility of an atypical meningioma. Recognizing these imaging characteristics is paramount for guiding optimal surgical strategy and ensuring appropriate patient counselling and postoperative management, including the consideration of adjuvant therapies, to improve long-term outcomes for this more aggressive meningioma subtype.
Patient consent
We confirm that we have obtained written, informed consent from the patient for the publication of this case report. The patient has been thoroughly informed about the details that will be published and understands the implications of the publication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Louis D.N., Perry A., Wesseling P., Brat D.J., Cree I.A., Figarella-Branger D., Hawkins C., Ng H.K., Pfister S.M., Reifenberger G., Soffietti R., von Deimling A., Ellison D.W. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol 2021 Aug 2; 23 (8): 1231-1251. doi:10.1093/neuonc/noab 106.10.1093/neuonc/noab 106PMC 832801334185076 · doi ↗ · pubmed ↗
- 2Rogers L., Barani I., Chamberlain M., Kaley T.J., Mc Dermott M., Raizer J., Schiff D., Weber D.C., Wen P.Y., Vogelbaum M.A. Meningiomas: knowledge base, treatment outcomes, and uncertainties. A RANO review J Neurosurg 2015 Jan; 122 (1): 4-23. doi:10.3171/2014.7.JNS 131644.10.3171/2014.7.JNS 131644 PMC 506295525343186 · doi ↗ · pubmed ↗
- 3Liu X., Han T., Wang Y., Liu H., Huang X., Zhou J. Differentiating angiomatous meningioma from atypical meningioma using histogram analysis of apparent diffusion coefficient maps. Quant Imaging Med Surg 2023 Jul 1; 13 (7): 4160-4170. doi:10.21037/qims-22-1224. Epub 2023 May 8.10.21037/qims-22-1224 PMC 1034730437456320 · doi ↗ · pubmed ↗
- 4Nazir I.Rafiq S.Naseed M.Dar M.A.Shaheen F.Differentiation of typical and atypical meningiomas using magnetic resonance imaging J Clin Imaging Sci 11202121
- 5Koga T.Minami S.Ishimaru Y.Tanaka M.Kumabe T.Tominaga T.Atypical and anaplastic meningiomas: MR imaging with diffusion-weighted imaging and perfusion-weighted imaging AJNR Am J Neuroradiol 2952008854859
- 6Toh C.H.Castillo M.Wong A.M.C.Wei K.C.Wong H.F.Ng S.H.Wan Y.L.Differentiation between classic and atypical meningiomas with use of diffusion tensor imaging AJNR Am J Neuroradiol 2992008163016351858340910.3174/ajnr.A 1170 PMC 8118781 · doi ↗ · pubmed ↗
- 7Filippi C.G.Edgar M.A.UluǧA.M.Prowda J.C.Heier L.A.Zimmerman R.D.Appearance of meningiomas on diffusion-weighted images: correlating diffusion constants with histopathologic findings AJNR Am J Neuroradiol 2212001657211158890 PMC 7975551 · pubmed ↗
- 8Sun S.Q., Kim A.H., Cai C., Murphy R.K., De Wees T., Sylvester P., Dacey R.G., Grubb R.L., Rich K.M., Zipfel G.J., Dowling J.L., Leuthardt E.C., Leonard J.R., Evans J., Simpson J.R., Robinson C.G., Perrin R.J., Huang J., Chicoine M.R. Management of atypical cranial meningiomas, part 1: predictors of recurrence and the role of adjuvant radiation after gross total resection. Neurosurgery 2014 Oct; 75 (4): 347-54; discussion 354-5; quiz 355. doi:10.1227/NEU.0000000000000461.10.1227/NEU.0000000000000 · doi ↗ · pubmed ↗