When Patent Foramen Ovale (PFO) Can Cause Trouble—A Misplacement of Pacemaker Lead Into the Left Ventricle
Ayman Helal, Ibrahim Antoun, Mohammed El-Din, Mohsin Farooq

TL;DR
A pacemaker lead mistakenly placed in the left ventricle due to a patent foramen ovale is identified and corrected, highlighting the importance of careful monitoring during implantation.
Contribution
This case highlights the rare but critical complication of pacemaker lead misplacement into the left ventricle via a patent foramen ovale and emphasizes diagnostic and procedural strategies to prevent complications.
Findings
Pacemaker lead was found in the left ventricle after crossing a patent foramen ovale.
Right bundle branch block-like ECG morphology raised suspicion of left ventricular pacing.
Lead extraction and repositioning into the right ventricle was successfully performed.
Abstract
Misplacement of pacemakers lead into the left ventricle (LV) is a rare but clinically important complication, often facilitated by unrecognized intracardiac shunts such as a patent foramen ovale (PFO). Early recognition is essential to avoid systemic embolization and ensure safe device function. We report a man in his 70s with a background of bioprosthetic aortic valve replacement, coronary bypass grafting, hypertension, chronic kidney disease, Parkinson′s disease, and prostate cancer, who underwent permanent pacemaker implantation for symptomatic sinus pauses. Follow‐up echocardiography 1 year later, performed as part of surveillance of his aortic valve prosthesis, unexpectedly revealed that the ventricular lead had crossed a PFO and was positioned in the LV via the mitral valve. His 12‐lead ECG demonstrated a right bundle branch block‐like paced morphology, raising suspicion of LV…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
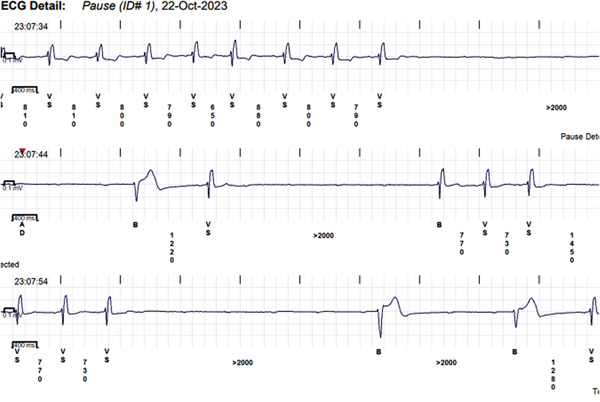 Figure 1
Figure 1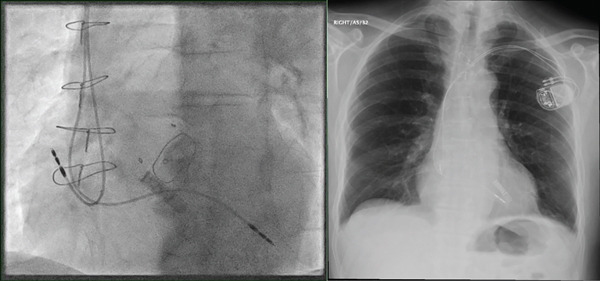 Figure 2
Figure 2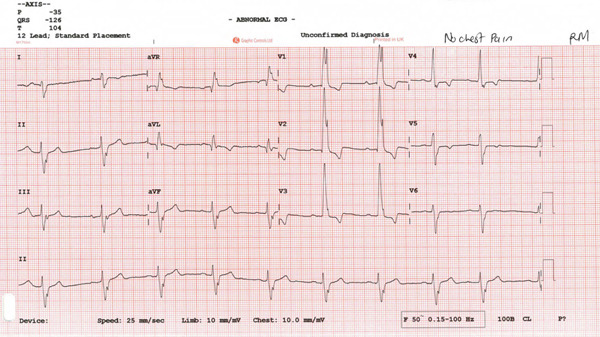 Figure 4
Figure 4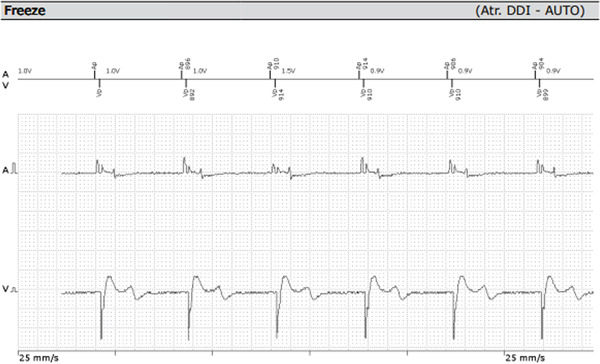 Figure 5
Figure 5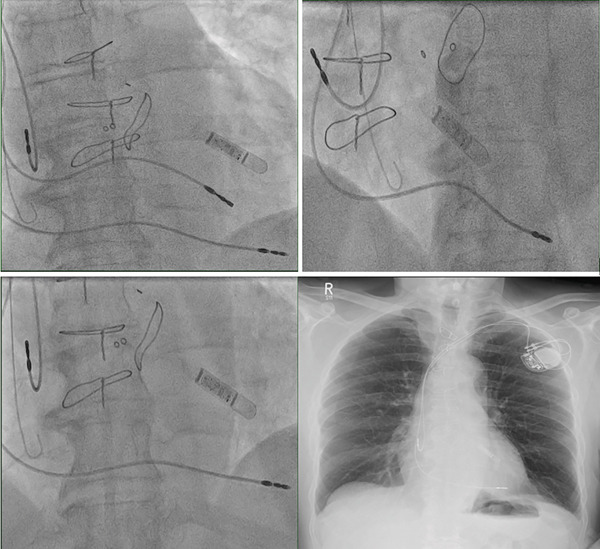 Figure 6
Figure 6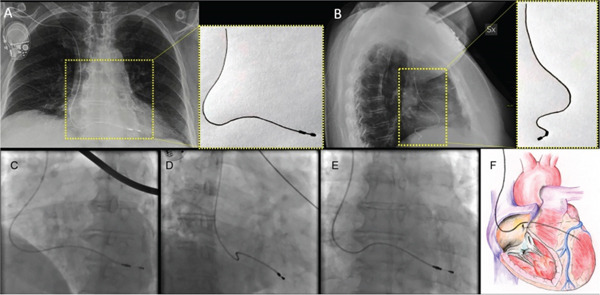 Figure 9
Figure 9|
|
|
|
|
|
|
|---|---|---|---|---|---|
| 0 to −90 | By V3, by V4, by V4, after V4 | RV septum or apex, RV septum or apex, posterior LV or coronary vein posterior LV or coronary vein | 86, 100, 26, 72 | 99, 92, 83, 100 | 95, 64, 36, 100 |
| −90 to −180 | By V3 | LV apex and distal anterior LV | 85 | 100 | 100 |
| 90–180 | Proximal anterior and anterolateral LV | 100 | 97 | 90 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac pacing and defibrillation studies · Cardiovascular and Diving-Related Complications · Cardiac Arrhythmias and Treatments
1. Introduction
Patent foramen ovale (PFO), a remnant of fetal circulation, can occasionally result in significant clinical complications when undiagnosed. In this case, we report a patient in his 70s who had a pacemaker lead unintentionally placed in the left ventricle (LV) through a PFO instead of the right ventricle (RV). This rare occurrence underscores the importance of recognizing specific clinical and diagnostic signs during and after pacemaker implantation. We also discuss how to detect such misplacements early and present the patient′s management course, including lead extraction and repositioning.
1.1. Case Presentation
A patient in his 70s with a significant past medical history, including bioprosthetic aortic valve replacement (25 mm Hancock valve) and bypass graft (saphenous venous graft [SVG] to right coronary artery [RCA]) 7 years prior to presentation; additional comorbidities include hypertension, dyslipidemia, chronic kidney disease (CKD) Stage 3, idiopathic Parkinson′s disease, and prostate cancer treated with radiotherapy. He had pacemaker implantation 1 year prior to presentation. The pacemaker was indicated for syncope, which was correlated to sinus pauses by an implantable loop recorder Reveal LINQ device, Medtronic (Figure 1), which demonstrated ventricular standstill of 5–6 s.
Sinus pauses detected by an implantable loop recorder.
He underwent successful pacemaker implantation (Biotronik, Enitra 6 DR‐T), with a right atrial (RA) lead placed in the right atrium (Biotronik, Solia Pro MRI S 53, Bipolar) and the right ventricular (RV) lead intended for the RV apex (Biotronik, Solia Pro MRI S 60, Bipolar) (Figure 2).
Confirmation of the pacemaker leads placement by fluoroscopy and chest x‐ray.
However, the follow‐up echocardiography (indicated for the bioprosthetic valve annual follow up) 1 year postdevice implantation revealed that the RV lead had passed through the PFO and was positioned in the LV, crossing from the right atrium (RA) to the left atrium (LA) and then through the mitral valve into the LV (Figure 3).
Figure 3. Echocardiogram showing the ventricular lead crossing (yellow arrow) from the right atrium to left atrium through PFO then to left ventricle in different views: parasternal long axis (a), apical four‐chamber view (b), subcostal (c) views with colored Doppler imaging showing mild mitral regurgitation (d).(a)(b)(c)(d)
The patient remained asymptomatic since implantation, with normal biventricular function. His 12 leads ECG (which was performed following the echocardiogram to assess the device) clearly demonstrated right bundle branch block (RBBB) morphology of the paced QRS complex with an axis of −120° (Figure 4) denoting pacing from the left ventricle. The pacemaker device download did not demonstrate any arrhythmia; his pacemaker checks were all satisfactory (Figure 5).
Patient′s 12 leads ECG demonstrated right bundle branch block (RBBB) morphology of the paced QRS complex with an axis of −120° denoting pacing from the left ventricle.
Satisfactory pacemaker checks.
There was no clinical evidence of systemic embolization, but we started anticoagulation with apixaban, and we decided to proceed with lead extraction and replacement to correct this complication.
1.2. Management and Follow‐Up
The patient underwent lead extraction and repositioning of the pacemaker lead into the RV after 1 year of the original implantation. Anticoagulation therapy with apixaban was initiated to mitigate the risk of thromboembolic complications while awaiting lead revision [1]. Aspirin was suspended during this period to reduce bleeding risk. We implanted a new RV lead; we initially crossed the lead with a large knuckle through the tricuspid valve and advanced it toward the right ventricular outflow tract (RVOT) to ensure lead placement into the RV apex. On fluoroscopy, the LV and RV leads follow different orientations (Figure 6). We confirmed position via obtaining different fluoroscopic views including RAO (right anterior oblique) and LAO (left anterior oblique), then we explanted the LV lead. An Electrocardiogram (ECG) comparison between pacing form the LV and RV leads in the presenting case are demonstrated in Figure 7. It was exceedingly difficult to differentiate in this case; however, the biphasic complexes which is usually seen in RV septal rather than apical pacing should raise the suspicion. The patient tolerated the procedure well and remained stable postoperatively. The apixaban was stopped after the procedure and aspirin was started again. Patient was sent home on the same day.
Confirmation of leads position (top left: both the old LV lead and the new RV lead before LV lead extraction, top right: RV lead in LAO view, bottom left: RV lead in RAO view, and bottom right: post‐procedure chest x‐ray).
Figure 7. Pacing from the LV lead (a) compared with pacing from the RV lead (b) during the new lead placement. The biphasic complexes which are usually seen in RV septal rather than apical pacing should raise the suspicion of abnormal lead position.(a)(b)
2. Discussion
2.1. How to Suspect LV Lead Misplacement
Although pacemakers′ leads misplacement into the LV is rare, its consequences can be significant, including systemic thromboembolism and impaired LV function. Early detection and intervention are critical to preventing complications [1].
Key factors that can raise suspicion of lead misplacement include abnormal pacing patterns, unexpected ECG findings, and imaging discrepancies.
- ECG clues: Inappropriate lead placement can often be suspected from the ECG. When pacing from the RV, the QRS complexes are typically left bundle branch block (LBBB)‐like, with a rightward axis. However, in LV pacing, the QRS complexes may mimic RBBB with a leftward axis (Figure 8) [2]. Electrocardiographic localization of lead position that exhibits RBBB morphologies during pacing is summarized in Table 1 [3]. In the presenting case, the patient′s 12‐lead ECG showed an RBBB‐like pattern (Figure 4), indicating the possibility of LV pacing.
Figure 8ECG comparison between LV pacing in Panel a showing right bundle branch block morphology versus RV pacing in panel b which shows LBBB morphology.(a)(b)
- Fluoroscopy: Fluoroscopic guidance during pacemaker implantation is the gold standard for lead placement. However, subtle misplacements like PFO‐related LV positioning may not be immediately apparent, especially when the lead follows an unexpected path. Careful inspection of the lead trajectory is critical [4]. The LAO view is especially useful as it provides a clear perspective on the lead′s orientation and helps differentiate between a correct RV placement and an unintended LV position through a PFO. In the LAO view, RV leads should be directed toward the RV apex, whereas leads that deviate toward the left side of the heart or cross the septum may indicate incorrect positioning in the LV. By observing the trajectory of the lead during implantation, the operator can immediately suspect mispositioning and take corrective action [5]. The importance of different fluoroscopic views is demonstrated in Figure 9 [6].
In the upper box, patient′s chest x‐ray: posteroanterior (PA) view (A); latero‐lateral view (B) with blowup indicating the pathway of the lead in the two projections; in the lower box: fluoroscopic images, 40° left anterior oblique view (C); 30° right anterior oblique view (D); PA view (E); a schematic representation of the lead malpositioned in the left ventricle, based on the PA projection; the location of the coronary sinus is depicted by the dotted line (F) [6].
- Imaging: Postimplantation echocardiography is important in confirming lead position, especially in patients with abnormal ECGs or unclear symptoms. The echocardiogram in this case clearly showed the lead traversing the PFO and entering the LV through the mitral valve. This imaging modality remains essential in identifying anatomical abnormalities contributing to lead misplacement, such as a PFO. [7] More dedicated imaging techniques can also be considered including CT and MRI to confirm the leads position [8, 9].
2.2. Extracting the Misplaced Lead
Lead extraction in patients with LV lead placement requires careful planning, particularly due to the risk of thromboembolism. Anticoagulation therapy before extraction is essential [9]. In this case, the patient was commenced on apixaban prior to the procedure to reduce thromboembolic risk. The extraction was performed uneventfully, and the new lead was correctly positioned in the RV. This was confirmed by fluoroscopy and postoperative ECG, chest X‐ray, and echocardiogram.
3. Conclusion
This case highlights the importance of thorough evaluation during pacemaker implantation, particularly in patients with anatomical variations such as a PFO. Early detection of LV lead misplacement is crucial to preventing complications, and clinicians should be vigilant for abnormal pacing patterns and imaging findings postimplantation. Anticoagulation and careful procedural planning are key to successful lead extraction and repositioning in these patients.
Consent
Patient consent has been obtained.
Disclosure
This work contained no materials from other sources.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding
No funding was received for this manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Solan A. N. , Solan M. J. , Bednarz G. , and Goodkin M. B. , Guidelines for the Management of Patients With Cardiac Pacemakers and Implantable Cardioverter Defibrillators, Europace. (2019) 21, no. 3, 478–487.
- 2Rovera C. , Golzio P. G. , Corgnati G. , Conti V. , Franco E. , Frea S. , and Moretti C. , A Pacemaker Lead in the Left Ventricle: An “Unexpected” Finding?, Journal of Cardiology Cases. (2019) 20, no. 6, 228–231, 10.1016/j.jccase.2019.08.012, 2-s 2.0-85072020151.31762840 PMC 6859553 · doi ↗ · pubmed ↗
- 3Coman J. A. and Trohman R. G. , Incidence and Electrocardiographic Localization of Safe Right Bundle Branch Block Configurations During Permanent Ventricular Pacing, American Journal of Cardiology. (1995) 76, no. 11, 781–784, 10.1016/S 0002-9149(99)80226-4, 2-s 2.0-0028801177, 7572654.7572654 · doi ↗ · pubmed ↗
- 4Sriramoju A. , Iyengar S. K. , and Srivathsan K. , Navigating Complications in Cardiac Pacemakers: A Comprehensive Review and Management Strategies, Reviews in Cardiovascular Medicine. (2024) 25, no. 8, 10.31083/j.rcm 2508299, 39228480.PMC 1136698739228480 · doi ↗ · pubmed ↗
- 5Hanafy D. A. , Soesanto A. M. , Setianto B. , Immanuel S. , Raharjo S. B. , Herqutanto , Amir M. , and Yuniadi Y. , Identification of Pacemaker Lead Position Using Fluoroscopy to Avoid Significant Tricuspid Regurgitation, Journal of Clinical Medicine. (2023) 12, no. 14, 10.3390/jcm 12144782, 37510897.PMC 1038121937510897 · doi ↗ · pubmed ↗
- 6Antoun I. , Helal A. , Farooqui A. , Farooq M. , and El-Din M. , Right Ventricular Lead Migration to the Abdominal Cavity: A Case Report of An Unexpected Journey, European Heart Journal – Case Reports. (2025) 9, no. 4, ytaf 179, 10.1093/ehjcr/ytaf 179, 40290158.40290158 PMC 12032392 · doi ↗ · pubmed ↗
- 7Solano J. , Admed D. , Ahmed A. , Abbas S. , Ahmed A. , and Antony R. , Navigating Misplaced Leads: A Case of Left Ventricle (LV) Lead Placement via a Patent Foramen Ovale (PFO) in a Dual-Chamber Permanent Pacemaker (PPM), Cureus. (2025) 17, no. 4, e 82835, 10.7759/cureus.82835.40416171 PMC 12101873 · doi ↗ · pubmed ↗
- 8Antoun I. , Helal A. , Farooqui A. , Farooq M. , and El-Din M. , Right Ventricular Lead Migration to the Abdominal Cavity: A Case Report of an Unexpected Journey, European Heart Journal-Case Reports. (2025) 9, no. 4, ytaf 179, 10.1093/ehjcr/ytaf 179.40290158 PMC 12032392 · doi ↗ · pubmed ↗