Nodular pulmonary amyloidosis presenting as a localized manifestation of lymphoproliferative disease: A three-case series
Sanya Chandna, Rutvik Raval, Tanya Rangwala, Atul C. Mehta

TL;DR
This case series shows that nodular pulmonary amyloidosis can be linked to or precede B-cell lymphoproliferative disorders, highlighting the need for long-term monitoring.
Contribution
The study presents three cases where nodular pulmonary amyloidosis was followed by lymphoproliferative disease, suggesting a potential clinical link.
Findings
Nodular pulmonary amyloidosis may coexist with or precede lymphoproliferative disorders.
Surgical biopsy is often needed to detect underlying lymphoid proliferation masked by amyloid deposits.
Long-term monitoring is recommended to detect potential hematologic disorders early.
Abstract
Pulmonary amyloidosis presents in nodular, tracheobronchial, and diffuse alveolar-septal forms. Nodular pulmonary amyloidosis (NPA) is usually localized and asymptomatic. It is often linked to indolent B-cell lymphoproliferative disorders (LPD). The National Comprehensive Cancer Network recommends long-term follow-up and evaluation for low-grade B-cell lymphoproliferative disorders when specific clinical features are present. However, there are no established screening guidelines specifically for detecting lymphoma in patients with nodular pulmonary amyloidosis. We describe three patients with NPA who later developed LPD. A 53-year-old woman with biopsy-proven κ-type localized AL amyloidosis was later found to have monoclonal gammopathy of undetermined significance. A 63-year-old man with prior hairy cell leukemia had λ-type NPA and subsequently Epstein–Barr virus–positive Hodgkin…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
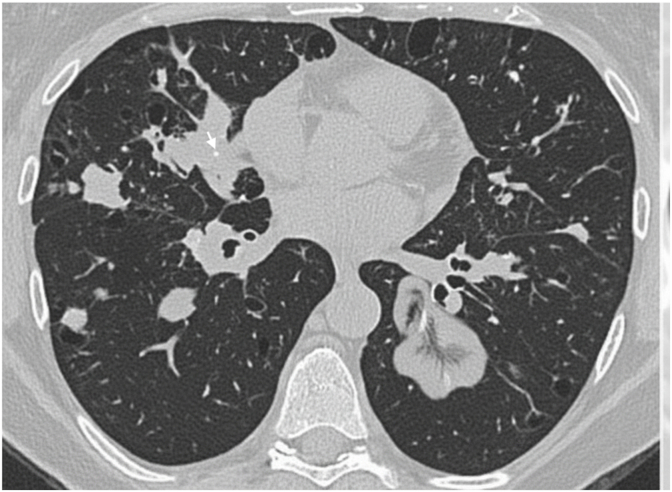 Figure 1
Figure 1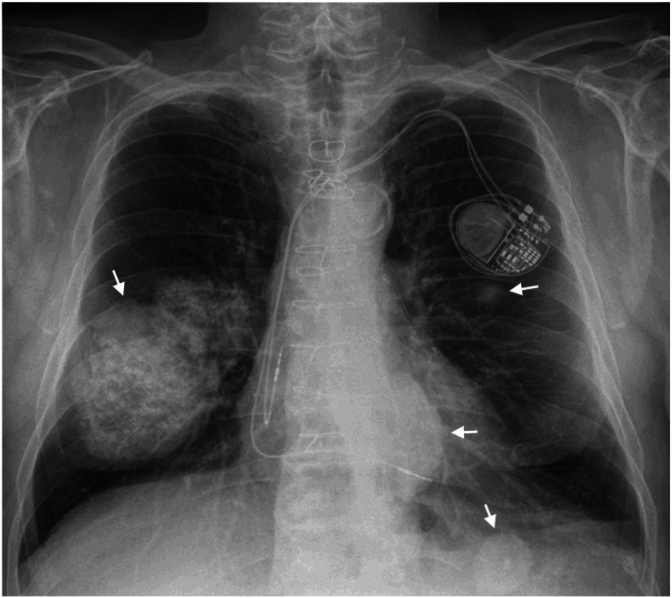 Figure 2
Figure 2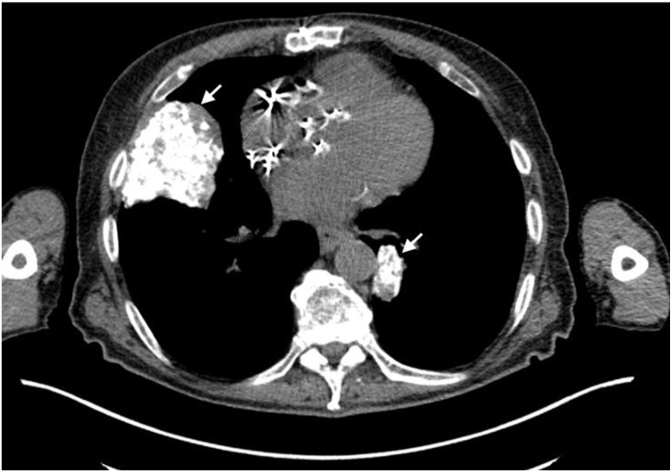 Figure 3
Figure 3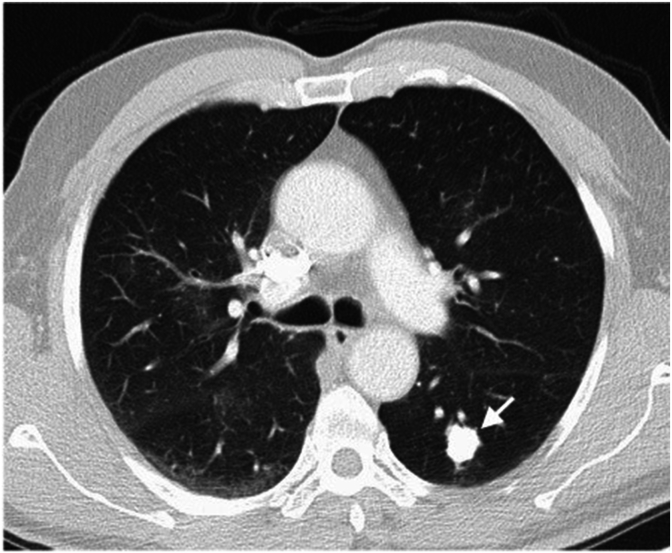 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmyloidosis: Diagnosis, Treatment, Outcomes · Multiple Myeloma Research and Treatments · Lung Cancer Research Studies
Abbreviations
NPA:Nodular Pulmonary AmyloidosisLPD:Lymphoproliferative DisordersCT:Computed TomographyMGUS:Monoclonal Gammopathy of Undetermined SignificanceVATS:Video-Assisted Thoracic SurgeryEBV:Epstein–Barr VirusCPAP:Continuous Positive Airway PressureEKG:ElectrocardiogramBALT:Bronchus-Associated Lymphoid TissueNSAIDs:Nonsteroidal Anti-Inflammatory DrugsMALT:Mucosa-Associated Lymphoid Tissue
Introduction
1
Amyloidosis is a heterogeneous group of diseases marked by the accumulation of misfolded proteins extracellularly. Amyloid is an insoluble protein that primarily consists of a β-sheet structure. It possesses a distinctive affinity for the Congo Red dye and exhibits an apple-green birefringence when viewed under polarized light microscopy. It is capable of affecting the body systemically, or it may be confined to a particular area. Localized amyloidosis commonly impacts the larynx, trachea, lung, skin, and urinary tract. In lung-related cases, three types exist - nodular, tracheobronchial, and diffuse alveolar-septal. The first two are typically associated with localized pulmonary amyloidosis [1,2]. Nodular pulmonary amyloidosis (NPA), more prevalent than tracheobronchial amyloidosis, is frequently misdiagnosed as a tumor. Many experts suggest that most instances of NPA stem from an underlying lymphoproliferative disorder (LPD) [3]. However, no studies have conclusively established nodular amyloidosis as a precursor to lymphoproliferative disorders.
We present a case series involving three patients diagnosed with NPA, subsequently developing LPD.
Case presentation
2
Case 1
2.1
A 53-year-old Caucasian female with no significant medical history presented to the pulmonary clinic with a 4-month history of dyspnea on exertion and dry cough. She was a lifelong non-smoker and worked as a medical transcriptionist. CT chest revealed multiple bilateral lung nodules (Fig. 1). She was started on prednisone for presumed sarcoidosis. After three months, she reported subjective improvement. However, a repeat chest CT showed the persistence of bilateral lung nodules. She ultimately underwent a CT-guided core needle biopsy of a right upper lobe lung nodule. The pathological examination demonstrated amyloid deposition. Amyloid typing identified κ light chain as the amyloidogenic protein. Prednisone was tapered off. She also underwent extensive lab testing. Her complete blood count, kidney function, and calcium level were within normal limits. Serum-free light chain assay was normal. Serum protein electrophoresis was positive for M-protein (0.98 mg/dL). Serum immunofixation revealed mildly elevated IgG [1620 mg/dL (ref. 717–1411 mg/dL)] and κ level [1290 mg/dL (ref. 534–1267 mg/dL)]. A 24-h urine protein was normal, and no M-protein was identified on urine protein electrophoresis. Bone marrow biopsy showed no evidence of clonal plasma cells. Given a normal serum light chain assay, normal bone marrow biopsy, and lack of systemic involvement, she was diagnosed with localized AL amyloidosis involving the lung. She was also diagnosed with monoclonal gammopathy of undetermined significance (MGUS) based on positive serum M-protein. No treatment was initiated, and she continued follow-up with pulmonology and oncology as an outpatient.Fig. 1CT Chest shows multiple bilateral lung nodules, some with central calcifications (arrow).Fig. 1
Case 2
2.2
A 63-year-old Caucasian male with a significant history of hairy cell leukemia, treated with chemotherapy status post splenectomy, in remission, presented with bilateral enlarging lung nodules found on a routine chest x-ray. He was completely asymptomatic. He smoked 3–4 cigarettes per week for 10 years and worked as a skier. He mentioned that roughly around 10 years ago, he was found to have lung nodules on chest imaging done at an outside hospital. He underwent a VATS lung biopsy 4 years ago at the same hospital, which showed nodular amyloid degeneration. Due to enlarging lung nodules, he was concerned if he had developed lung malignancy and hence came to our clinic. The chest x-ray revealed enlarging nodules in the right and left lung, with the dominant nodule in the right middle lobe measuring 3.8 × 4.3 cm and a retrocardiac nodule is 2.8 cm (Fig. 2a, Fig. 2ba & b). He underwent a transbronchial biopsy of the right middle lobe nodule, consistent with nodular amyloidosis. Amyloid typing identified λ light chain as the amyloidogenic protein. A normal bone marrow biopsy confirmed the absence of systemic amyloidosis involvement, leading to a diagnosis of AL amyloidosis. He continued to follow up at the clinic and get surveillance imaging. A subsequent CT scan of the abdomen done after a few years revealed a notable increase in retroperitoneal lymphadenopathy. Consequently, a diagnostic laparoscopy was performed, during which an excisional biopsy of the retroperitoneal lymph node was conducted. The biopsy results indicated EBV-positive Hodgkin lymphoma, specifically the nodular sclerosis type, with focal involvement by hairy cell leukemia. Notably, the congo red stain tested negative for amyloid. Subsequently, he commenced chemotherapy treatment comprising brentuximab-vedotin, adriamycin, vinblastine, and dacarbazine. He is currently undergoing regular follow-ups at the clinic.Fig. 2aChest radiograph revealing multiple calcified bilateral pulmonary nodules (arrows) of varying size.Fig. 2aFig. 2bCT Chest confirming calcification in pulmonary nodules (arrows).Fig. 2b
Case 3
2.3
A 74-year-old Asian male with a medical history significant for bilateral calcified lung nodules, legionnaire's disease requiring prolonged hospitalization, obstructive sleep apnea on CPAP, hypertension, and hyperlipidemia presented to the emergency room with pleuritic chest pain and shortness of breath, which started a couple of hours prior. Vitals and lab work, including a complete blood count, comprehensive metabolic panel, troponin, and D dimer, were all normal. The EKG did not show any signs of acute ischemia. However, a chest x-ray revealed a significant left pneumothorax and left lung collapse. An 8 fr left anterior chest tube was inserted, but due to persistent pneumothorax, cardiothoracic surgery was consulted. A subsequent CT chest scan showed a large, loculated pneumothorax. The CT scan also shows calcified lung nodule (Fig. 3). The patient underwent VATS with left upper lobe bullectomy, left upper and lower lobe wedge resection, and left talc pleurodesis. The patient was already undergoing regular outpatient monitoring with a pulmonologist for the surveillance of his calcified lung nodules. Notably, he worked as an accountant and had no history of smoking. An infectious workup for the lung nodules done as an outpatient revealed negative results. While undergoing VATS, a biopsy of the lung nodule was performed as well. Pathology results showed extranodal marginal zone lymphoma of bronchus-associated lymphoid tissue (BALT lymphoma) and nodular amyloidosis with ossification. There were no signs of systemic amyloidosis. The patient continued regular follow-ups for surveillance imaging, which consistently showed stable CT chest findings. Additionally, he also followed up with an oncologist who did not recommend any specific treatment. Three years later, the patient experienced an upper gastrointestinal bleed due to the use of nonsteroidal anti-inflammatory drugs and steroids. An esophagogastroduodenoscopy revealed mucosa-associated lymphoid tissue (MALT lymphoma). Immunostaining was negative for Helicobacter pylori. Oncology team suggested no immediate treatment and opted for continued surveillance. The patient continues to follow up with both oncology and pulmonology for ongoing monitoring.Fig. 3CT Chest revealing calcified left lower lobe nodule (arrow).Fig. 3
Discussion
3
NPA is form of localized pulmonary amyloidosis. Most patients are asymptomatic, and the condition is often found incidentally on imaging. When symptoms do occur, they may include cough, wheezing, shortness of breath, or recurrent infections [1]. Reports suggest that about 30–50 % of NPA cases are linked to an underlying LPD, most commonly low-grade B-cell lymphomas such as MALT lymphoma [[3], [4], [5], [6]]. In some cases, lung nodules may be the first sign of the disease [6,7]. The amyloid in these patients forms because a small group of abnormal B cells produces excess monoclonal light chains, sometimes heavy chains. These misfold and deposit in the lung as AL-type amyloid [3,4]. Distinguishing nodular pulmonary amyloidosis from lymphoma can be difficult because the heavy amyloid deposits often hide the underlying lymphoid process. Accurate diagnosis usually requires combining morphology, immunostains, and molecular studies. A surgical biopsy is often needed instead of a transbronchial biopsy, since larger tissue samples are usually required to detect a lymphoproliferative disorder that may be hidden by the amyloid deposits [8,9]. Localized AL amyloidosis generally has a favorable outcome and rarely progresses to systemic disease [10]. Treatment options include surgical removal, bronchoscopic debulking, and laser-based therapies [1]. Even in cases associated with lymphoma, the overall prognosis is usually favorable, although long-term monitoring is needed. The current literature shows that NPA is often associated with LPD, but no studies have definitively shown that NPA itself acts as a precursor to lymphoma.
Our first patient with lung nodules was initially misdiagnosed with sarcoidosis. A biopsy confirmed the diagnosis of NPA, and prednisone was tapered off. However, she was later diagnosed with MGUS. The second patient had a previous history of hairy cell leukemia, which was in remission. During routine screening, lung nodules were discovered. He was entirely asymptomatic. A biopsy confirmed the diagnosis of NPA. Given the lack of symptoms, monitoring was the chosen approach. Subsequently, after a few years, this patient was diagnosed with Hodgkin's lymphoma. The third patient, who was being monitored for lung nodules, underwent a biopsy solely due to developing a pneumothorax that required a VATS procedure. Incidentally, this procedure led to the diagnosis of both NPA and Bronchus Associated Lymphoid Tissue Lymphoma (BALToma). A few years later, this patient experienced a gastrointestinal bleed due to non-steroidal anti-inflammatory drugs and steroids and was incidentally diagnosed with gastric Mucosa-associated lymphoid tissue lymphoma (MALToma).
Although evidence is limited, our series raises the question of whether NPA may represent a precursor of a clonal B-cell process that becomes clinically apparent as lymphoma over time. It is possible that the lymphoma was present from the start, but was too small or subtle to detect at the time NPA was diagnosed. Chronic antigenic stimulation from infections, autoimmune disease, or ongoing inflammation may promote this clonal B-cell proliferation over time. One prior study also described a patient who developed MALT lymphoma eight years after excision of a cutaneous AL amyloidoma, supporting the idea that progression can occur [11].
Currently, there are no guidelines recommending routine screening for LPD in patients with NPA. Given the known association between localized AL amyloidomas and B-cell neoplasms, future recommendations could include periodic surveillance to detect hematologic malignancies earlier. In developing such recommendations, several factors should be considered. Risk stratification could include the presence of monoclonal proteins, clonal B-cell populations on biopsy, multiple or progressive nodules, or clinical symptoms suggestive of lymphoma. Follow-up should incorporate periodic clinical evaluation, laboratory studies such as serum and urine protein electrophoresis, immunofixation, and serum free light-chain assays, as well as imaging to monitor nodule progression. Adequate tissue sampling and careful pathological review are essential to detect subtle lymphoproliferative processes that may be obscured by amyloid deposits. Finally, patient education regarding symptoms that should prompt evaluation and clearly defined follow-up intervals is an important component of any surveillance strategy. Larger studies are needed to establish evidence-based guidelines for early detection and intervention in this patient population.
Conclusion
4
There are no guideline-directed surveillance intervals for screening patients with localized amyloidoma for lymphoproliferative disorders. Although progression to systemic amyloidosis is uncommon, the potential development of an underlying lymphoproliferative disorder warrants long-term follow-up. Ongoing monitoring should include periodic clinical evaluation, serial testing for monoclonal proteins, assessment of organ function, and imaging when clinically indicated.
CRediT authorship contribution statement
Sanya Chandna: Writing – review & editing, Writing – original draft, Conceptualization. Rutvik Raval: Writing – review & editing, Writing – original draft. Tanya Rangwala: Writing – original draft. Atul C. Mehta: Writing – review & editing, Supervision, Data curation, Conceptualization.
Ethical approval
None.
Consent
Written consent is available upon request.
Guarantor
Dr. Atul C. Mehta (Corresponding Author).
Funding
None.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Patel H.Sheikh A.Medarametla G.D.Uncommon presentation of undiagnosed B-Cell lymphoproliferative disorder as nodular pulmonary amyloidosis J. Med. Cases 14120233610.14740/JMC 402636755997 PMC 9881482 · doi ↗ · pubmed ↗
- 2Ding F.Li Y.Balasubramanian S.A unique case of combined nodular and tracheobronchial amyloidosis Oxford Med Case Reports 20212202110.1093/omcr/omaa 134PMC 788514933614045 · doi ↗ · pubmed ↗
- 3Grogg K.L.Aubry M.C.Vrana J.A.Theis J.D.Dogan A.Nodular pulmonary amyloidosis is characterized by localized immunoglobulin deposition and is frequently associated with an indolent B-cell lymphoproliferative disorder Am. J. Surg. Pathol.373201340641210.1097/PAS.0B 013E 318272 FE 1923282974 · doi ↗ · pubmed ↗
- 4Ryan R.J.Sloan J.M.Collins A.B.Mansouri J.Raje N.S.Zukerberg L.R.Ferry J.A.Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue with amyloid deposition: a clinicopathologic case series Am. J. Clin. Pathol.13712012 Jan 516410.1309/AJCPI 08WAKYVLHHAPMID: 2218047822180478 · doi ↗ · pubmed ↗
- 5Lim J.K.Lacy M.Q.Kurtin P.J.Kyle R.A.Gertz M.A.Pulmonary marginal zone lymphoma of MALT type as a cause of localised pulmonary amyloidosis J. Clin. Pathol.5482001 Aug 64264610.1136/jcp.54.8.642PMID: 11477123; PMCID: PMC 173150411477123 PMC 1731504 · doi ↗ · pubmed ↗
- 6Dacic S.Colby T.V.Yousem S.A.Nodular amyloidoma and primary pulmonary lymphoma with amyloid production: a differential diagnostic problem Mod. Pathol.1392000 Sep 93494010.1038/modpathol.3880170 PMID: 1100703211007032 · doi ↗ · pubmed ↗
- 7Upadhaya S.Baig M.Towfiq B.Al Hadidi S.Nodular Pulmonary Amyloidosis with Primary Pulmonary MALT lymphoma Masquerading as Metastatic Lung Disease 201710.1080/20009666.2017.1343075 Published online PMC 553824628808514 · doi ↗ · pubmed ↗
- 8Filippi N.Diotti C.Donghi S.M.Galetta D.Sedda G.Sandri A.De Camilli E.Guarize J.Spaggiari L.Diagnostic and therapeutic implications of pulmonary lymphoma associated with nodular amyloidosis Ann. Thorac. Surg.10752019 Maye 325e 32710.1016/j.athoracsur.2018.09.037Epub 2018 Nov 2. PMID: 3039585230395852 · doi ↗ · pubmed ↗