Case report: Spatiotemporal HER2 heterogeneity in AFP-producing gastric cancer: navigating long-term survival with molecularly-guided therapy in a refractory case
Yanwen Diao, Haobo Yin, Xin Sun, Qian Dong, Jingdong Zhang

TL;DR
A rare case of aggressive gastric cancer showed long-term survival through targeted therapies and re-biopsy-guided treatment adjustments.
Contribution
Demonstrates the importance of re-biopsy and sequential precision therapy in managing HER2-heterogeneous AFPGC.
Findings
Anti-angiogenic and immunotherapy showed efficacy in AFPGC.
HER2 conversion detected via re-biopsy led to successful ADC treatment.
Sequential therapy achieved 79-month survival in a refractory AFPGC case.
Abstract
Alpha-fetoprotein-producing gastric cancer (AFPGC) is a rare, aggressive subtype with poor prognosis. We report a metastatic AFPGC case showing spatiotemporal human epidermal growth factor receptor 2 (HER2) heterogeneity. Following progression on first-line FLOT chemotherapy, the 65-year-old male received second-line apatinib plus programmed death-1 (PD-1) inhibitor. At progression (27 months), a lymph node biopsy revealed HER2 conversion from 1+ to 3 +. Third-line anti-HER2 antibody-drug conjugate (ADC) DP303c rapidly achieved partial response with normalized AFP. Despite treatment discontinuation due to neurotoxicity after 5 cycles, response persisted. Overall survival reached 79 months. This case highlights: 1) efficacy of anti-angiogenic and immunotherapy in AFPGC; 2) necessity of re-biopsy for detecting HER2 heterogeneity; and 3) potent activity of ADCs against HER2-converted…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
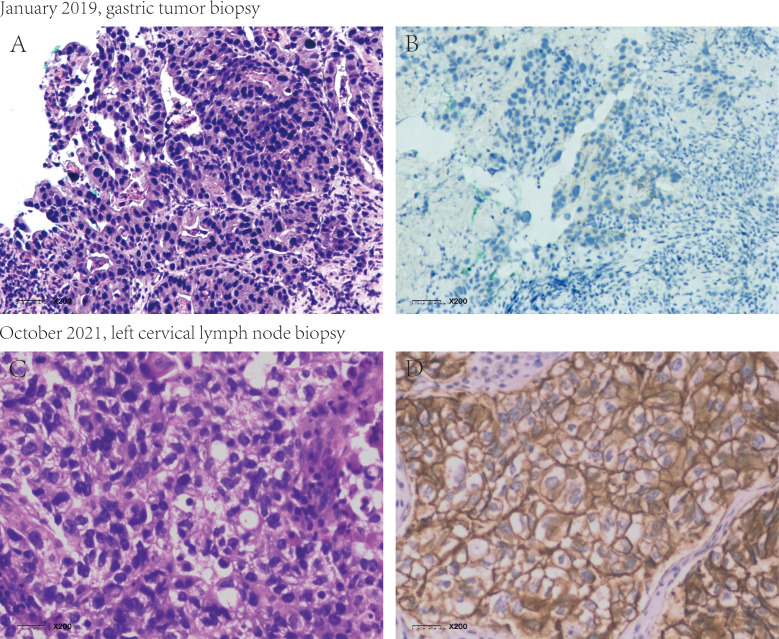 Figure 1
Figure 1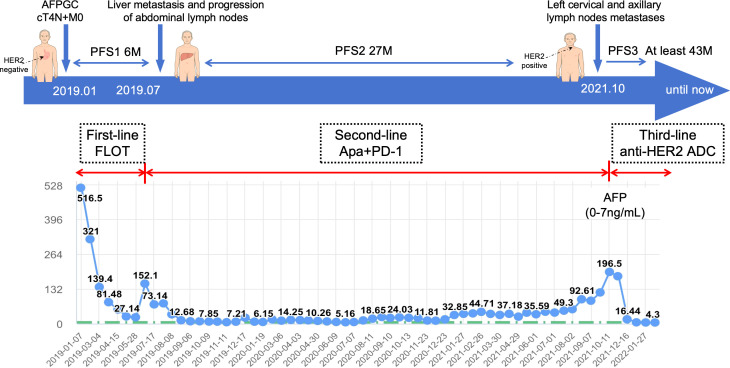 Figure 2
Figure 2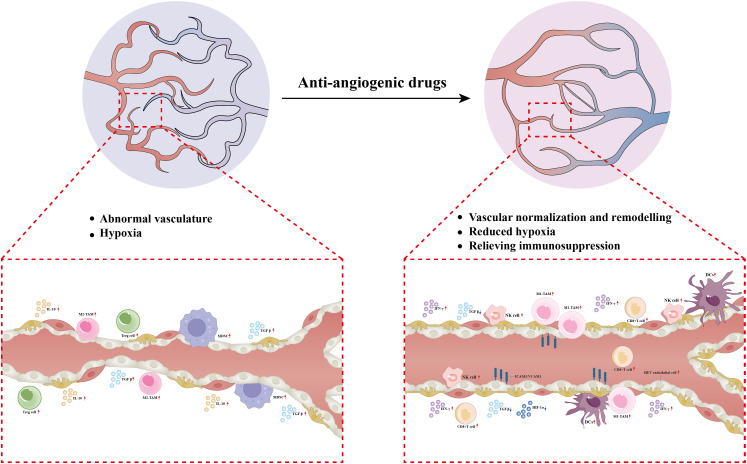 Figure 3
Figure 3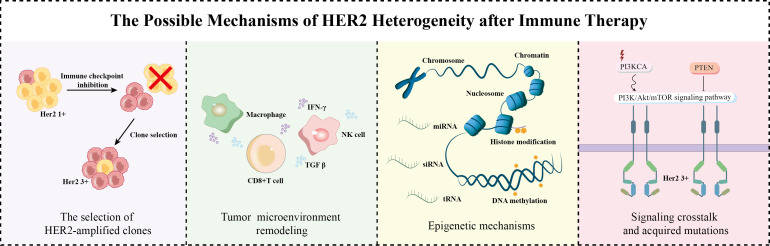 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHER2/EGFR in Cancer Research · Gastric Cancer Management and Outcomes · Testicular diseases and treatments
Introduction
Gastric cancer (GC) remains highly prevalent in China, with advanced disease exhibiting marked heterogeneity and poor prognosis, underscoring the need for molecular-level insights to guide treatment. AFPGC, a rare subtype representing 1.3%–15% of cases globally (1), is characterized by frequent liver metastasis, limited therapeutic options, and an unfavorable outlook. HER2 serves as a key therapeutic target in GC, though its heterogeneity—evidenced by discordance rates of 45%–79% by immunohistochemistry (IHC) and 23%–54% by in situ hybridization (ISH) (2), —complicates patient stratification and precise targeting. Here, we present a case of metastatic AFPGC with dynamic spatiotemporal HER2 heterogeneity, in which sequential molecularly-guided therapy enabled prolonged survival.
Case presentation
In January 2019, a 65-year-old male presenting with gastric discomfort underwent gastroscopy, which revealed a mass in the gastric body and antrum with histopathological confirmation of adenocarcinoma. IHC showed HER2 1+ (clone 4B5) and intact mismatch repair proteins (MSH2+, MSH6+, MLH1+, PMS2+) (Supplementary Image 1). Next-generation sequencing (NGS) indicated microsatellite stable (MSS) status and no ERBB2 amplification. Abdominal CT revealed gastric wall thickening and multiple enlarged lymph nodes in the porta hepatis and along the lesser curvature. The initial diagnosis was cT4aN+M0 gastric cancer. FLOT therapy (docetaxel, oxaliplatin, 5-fluorouracil) was started on January 24, 2019. After seven cycles, disease progressed with new liver metastases and lesser curvature lymph nodes enlargement, yielding a PFS of 6 months. Serum AFP was initially elevated at 516.5 ng/mL (normal: 0–7 ng/mL), declined to 27.14 ng/mL during therapy, but rebounded to 152.1 ng/mL at progression, confirming AFPGC. On July 25, 2019, the patient entered our IIT (ClinicalTrials.gov NCT04006821) receiving apatinib plus a PD-1 inhibitor as second-line therapy. PR was achieved after four cycles and sustained (Supplementary Image 2), with regression of liver and abdominal nodal lesions and normalized AFP. Adverse events included grade 3 proteinuria (apatinib-related), controlled by dose reduction, and grade 3 hypophysitis (PD-1 inhibitor-related), improved to grade 1 with hormone replacement.In October 2021, AFP rose to 195 ng/mL. CT showed progression in left cervical, supraclavicular, and axillary nodes, with stable abdominal and primary lesions. Gastroscopy showed no malignancy. Second-line PFS was 27 months. PET-CT confirmed metastatic lymph nodes; mild gastric uptake was considered post-treatment change. No metabolically active metastases were detected in the liver. A left cervical node biopsy (October 15, 2021) confirmed metastatic gastric adenocarcinoma. IHC showed HER2 3+ (clone 4B5), PD-L1 CPS <1 (Dako 22C3), Ki67 80%+, and the intact Mismatch repair protein. NGS (YucoOne^®^ Pro+ panel; depth 2134.4×; tumor content 55%) confirmed ERBB2 amplification (copy number 37.3), indicating HER2 heterogeneity from primary (1+) to metastasis (3+) (Figure 1). Beginning November 24, 2021, the patient received five cycles of DP303c, a novel anti-HER2 ADC, within a clinical trial (ClinicalTrials.gov NCT04826107). PR was observed after two cycles, coinciding with a rapid decline in serum AFP from 195 ng/mL to 16.44 ng/mL after the first cycle and subsequent normalization. Treatment was discontinued on April 2, 2022, following the fifth cycle due to grade 3 neurotoxicity, which manifested as persistent limb numbness, tingling, and restricted movement. Grade 2 ocular symptoms (decreased vision and dryness) also occurred. Supportive care, including neurotrophic agents, gabapentin, and traditional Chinese medicine acupuncture, led to gradual neurological improvement over approximately two years, while ocular symptomsgradually improved following the administration of artificial tears and steroid eye drops.Follow-up confirmed sustained PR, normalized AFP, no endoscopic evidence of disease, and an overall survival of 79 months (January 2019–August 2025) with a good quality of life. (Figure 2).
Histopathological and HER2 IHC analysis of the primary gastric tumor and metastatic lymph node. (A, B) HE staining and HER2 IHC of the primary gastric tumor biopsy, showing HER2 1+ (negative). (C, D) H&E staining and HER2 IHC of the metastatic left cervical lymph node biopsy, showing HER2 3+ (positive). HER2 IHC was performed using the Roche anti-HER2 rabbit monoclonal antibody (clone 4B5) and scored according to gastric cancer ASCO/CAP guidelines
Timeline of the clinical course and AFP dynamics.
Discussion
AFPGC is a rare variant, often misdiagnosed due to nonspecific clinical presentation. It is defined by elevated serum AFP (>20 ng/mL) or immunohistochemical evidence of AFP expression, and is associated with larger tumor size, frequent vascular and lymphatic invasion, and high liver metastasis rates (33%–72%) (3–5). AFP level serves as an independent prognostic factor, with 5-year survival declining sharply from 45.8% (AFP <20 ng/mL) to 7.7% (AFP >300 ng/mL) (6, 7). HER2 positivity is more common in AFPGC and hepatoid adenocarcinoma (21.8%–37.5%) than in conventional gastric cancer (12%–18%) (8, 9). The tumor microenvironment frequently shows VEGF-C overexpression and prominent angiogenesis (10), suggesting susceptibility to anti-angiogenic agents such as apatinib and ramuciruma (5, 11).
Despite limited evidence, immunotherapy shows promise in AFPGC. While Li et al. reported improved PFS with ICIs plus chemotherapy (22.0 vs. 4.3 months), PD-L1 CPS proved unreliable in predicting response (12). Furthermore, Liu et al. described a functionally heterogeneous CD8+ T-cell population co-expressing activation and exhaustion markers in hepatoid adenocarcinoma, affirming the immune context of these tumors (13). However, further exploration is needed to identify optimal combination strategies or more reliable predictive biomarke.
The combination of anti-angiogenic agents and immune checkpoint inhibitors(ICIs)has demonstrated considerable anti-tumor potential. Anti-angiogenic drugs targeting VEGF/VEGFR2 promote vascular normalization, alleviate hypoxia, and enhance the infiltration of CD8^+^ T cells (14, 15), and inducing high endothelial venules (HEVs) (16)—key components of tertiary lymphoid structures that support immune cell trafficking and activation. These agents further modulate the cytokine milieu by downregulating immunosuppressive factors such as HIF-1α and TGF-β, while enhancing the cytotoxicity of CD8^+^ T cells and NK cells (17–19). Additionally, they reduce recruitment of M2-type tumor-associated macrophages (TAMs) and regulatory T cells (Tregs), promote M1 polarization, and modulate immune-related genes such as ICAM-1, enhancing pro-inflammatory signaling including IFN-γ (20). These coordinated mechanisms enhance the depth and durability of immunotherapy responses (Figure 3). Given the promise of anti-VEGF and immunotherapy in AFPGC and its clinicopathological overlap with hepatocellular carcinoma, we initiated a clinical trial of apatinib plus a PD-1 inhibitor. This strategy provided a 27-month PFS in our second-line patient, remodeling the tumor immune microenvironment from an immune-excluded/desert to an immune-inflamed phenotype, thereby overcoming baseline PD-L1 negativity and microsatellite stability. Notably, the recent CAP 06 trial supports this strategy, reporting promising efficacy for a similar first-line regimen (21).
Proposed mechanism of synergistic effect between anti-angiogenic therapy and immunotherapy. Treg, Regulatory T Cell; MDSC, Myeloid-Derived Suppressor Cell; M2-TAM, M2-Polarized Tumor-Associated Macrophage; M1-TAM,M1-Polarized Tumor-Associated Macrophage; CD8+ T Cell, Cluster of Differentiation 8-positive T Lymphocyte; NK Cell, Natural Killer Cell; DCs, Dendritic Cell; HIF-1a, Hypoxia-Inducible Factor 1-alpha; TGF-b, Transforming Growth Factor-beta; IL-10, nterleukin-10;IFN-g, Interferon-gamma; ICAM-1, Intracellular Adhesion Molecule-1; VCAM-1, Vascular Cell Adhesion Molecule-1.
A striking feature of this case was the dynamic evolution of HER2 expression under therapeutic pressure. At progression, the patient developed extensive nodal metastases while other sites remained stable; a cervical node biopsy confirmed conversion from HER2-negative to HER2-positive status, revealing clear spatiotemporal heterogeneity.
HER2 heterogeneity in gastric cancer is well established, varying by subtype (higher in intestinal-type (22, 23) and showing 1%-14% primary-metastasis discordance (24). A meta-analysis reported 7% overall HER2 discordance, including 17% positive-to-negative and 4% negative-to-positive conversion (25). Mirroring this heterogeneity, 24%-35% of HER2-positive patients convert to negative post-trastuzumab (26), while studies like GASTHER1 (5.7%) (27) and GASTHER2 (4.0%) (28) demonstrate the reverse conversion. The clinical relevance is highlighted by a converted patient in GASTHER2 achieving 9.47 months PFS with T-DM1.
While the mechanisms underlying HER2 heterogeneity remain incompletely understood, sustained immune pressure may drive the selection of HER2-amplified clones.In this case, such pressure may have selected for HER2-amplified subclones with enhanced immune escape capabilities, progressively reshaping the overall HER2 expression profile (29). This process is further supported by observations in bladder urothelial carcinoma, where HER2 expression in recurrent tumors differs significantly from primary lesions (30, 31), underscoring the role of immune selection in modulating HER2 status (32). Concurrently, immune checkpoint inhibition remodels the tumor microenvironment, enabling cytokines—such as IFN-γ and TNF-α secreted by CD8^+^ T cells, NK cells, and macrophages—to exert dual regulatory effects on HER2 expression (33). In addition, potentially influencing HER2 expression via epigenetic mechanisms including promoter DNA methylation (34), histone modifications (35, 36), and non-coding RNA regulation (37, 38). Additional complexity arises from signaling crosstalk and acquired mutations in genes such as PIK3CA (39), collectively enhancing the plasticity of HER2 expression under immunotherapeutic pressure. Together, these mechanisms likely underlay the observed conversion of HER2 status in this patient following immunotherapy, as schematized in Figure 4.
Proposed mechanisms underlying HER2 heterogeneity. PI3K, Phosphatidylinositol 3-kinase; Akt, Protein Kinase B; mTOR, Mammalian Target of Rapamycin; PTEN, Phosphatase and Tensin Homolog.
This single-case report, while demonstrating encouraging outcomes, has inherent limitations that preclude broad generalizability. The survival benefit observed requires validation in larger prospective AFPGC cohorts. Additionally, the documented HER2 heterogeneity and clonal evolution, though supported by longitudinal biomarker assessment, warrant further investigation through multi-region sequencing or in vitro models. Notwithstanding these limitations, this case emphasizes the clinical value of repeat biopsy at progression to identify new targetable alterations such as HER2 conversion. Treatment with the novel anti-HER2 ADC DP303c resulted in manageable but clinically significant ocular and neurological toxicities, highlighting the need for vigilant monitoring and multidisciplinary management to maintain therapeutic continuity.
Conclusions
The combination of anti-angiogenic agents and ICIs demonstrates efficacy in AFPGC. Our patient achieved sustained response with apatinib plus PD-1 inhibitor in the second-line setting, with manageable safety profile. Given gastric cancer’s heterogeneity, repeat biopsy upon progression proved crucial - revealing HER2 conversion that guided successful third-line anti-HER2 ADC therapy. This sequential precision approach enabled long-term survival in refractory metastatic AFPGC, highlighting the importance of dynamic biomarker-guided individualized treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Intire KR Waldmann TA Moertel CG Go VL . Serum alpha-fetoprotein in patients with neoplasms of the gastrointestinal tract. Cancer Res. (1975) 35:991–6., PMID: 46783 · pubmed ↗
- 2Wada R Hirabayashi K Ohike N Morii E . New guidelines for HER 2 pathological diagnostics in gastric cancer. Pathol Int. (2016) 66:57–62. doi: 10.1111/pin.12390, PMID: 26814046 · doi ↗ · pubmed ↗
- 3Luo B Wu Z Hu C Xie W He J Liu H . Alpha fetoprotein (AFP)-producing gastric cancer: clinicopathological features and treatment strategies. Cell bioscience. (2025) 15:82. doi: 10.1186/s 13578-025-01424-8, PMID: 40495217 PMC 12153134 · doi ↗ · pubmed ↗
- 4Hirajima S Komatsu S Ichikawa D Kubota T Okamoto K Shiozaki A . Liver metastasis is the only independent prognostic factor in AFP-producing gastric cancer. World J gastroenterol. (2013) 19:6055–61. doi: 10.3748/wjg.v 19.i 36.6055, PMID: 24106406 PMC 3785627 · doi ↗ · pubmed ↗
- 5Li N Bai C Zhang R Ma L Ren X Zhang J . Efficacy and safety of apatinib for the treatment of AFP-producing gastric cancer. Trans Oncol. (2021) 14:101004. doi: 10.1016/j.tranon.2020.101004, PMID: 33383486 PMC 7777135 · doi ↗ · pubmed ↗
- 6Lin HJ Hsieh YH Fang WL Huang KH Li AF . Clinical manifestations in patients with alpha-fetoprotein-producing gastric cancer. Curr Oncol (Toronto Ont). (2014) 21:e 394–399. doi: 10.3747/co.21.1768, PMID: 24940098 PMC 4059802 · doi ↗ · pubmed ↗
- 7Zhan Z Chen B Yu J Zheng J Zeng Y Sun M . Elevated serum alpha-fetoprotein is a significant prognostic factor for patients with gastric cancer: results based on a large-scale retrospective study. Front Oncol. (2022) 12:901061. doi: 10.3389/fonc.2022.901061, PMID: 35847953 PMC 9277009 · doi ↗ · pubmed ↗
- 8He F Fu Y Sun Q Geng P Zheng Z Pu X . Integrated clinicopathological and immunohistochemical analysis of gastric adenocarcinoma with hepatoid differentiation: an exploration of histogenesis, molecular characteristics, and prognostic markers. Hum pathol. (2021) 115:37–46. doi: 10.1016/j.humpath.2021.02.003, PMID: 33636206 · doi ↗ · pubmed ↗