Case Report: Xsens motion analysis and virtual reality–based rehabilitation in a national-level badminton player following MPFL reinjury leading to postoperative patellar fracture
Chaitali S. Vikhe, Nikita Bhusari, Swapnil U. Ramteke

TL;DR
A badminton player recovered from patellar issues using motion analysis and virtual reality rehabilitation after multiple surgeries.
Contribution
Demonstrates a multidisciplinary rehabilitation approach using Xsens and VR for post-surgical patellar recovery in athletes.
Findings
Rehabilitation improved pain-free range of motion, quadriceps strength, and proprioceptive precision.
KOOS and LEFS scores improved significantly, indicating functional recovery.
Xsens analysis showed restored gait symmetry and balance, enabling return to sport.
Abstract
Recurrent patellar dislocation presents a significant rehabilitation challenge, particularly in athletes engaged in high-demand, multi-directional sports such as badminton. This case report describes a complex presentation in a state-level athlete with multiple patellar dislocations, followed by medial patellofemoral ligament (MPFL) reconstruction and a subsequent comminuted patellar fracture. The case was further complicated by proprioceptive deficits, extension lag, sensory changes, and kinesiophobia, all of which limited the athlete's functional performance and return to sport. A 23-year-old male National-level badminton player reported persistent functional limitations after recurrent patellar dislocations and two surgeries (MPFL reconstruction and patellar fracture fixation using K-wires). Clinical examination revealed quadriceps atrophy, patellar hypomobility, altered…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2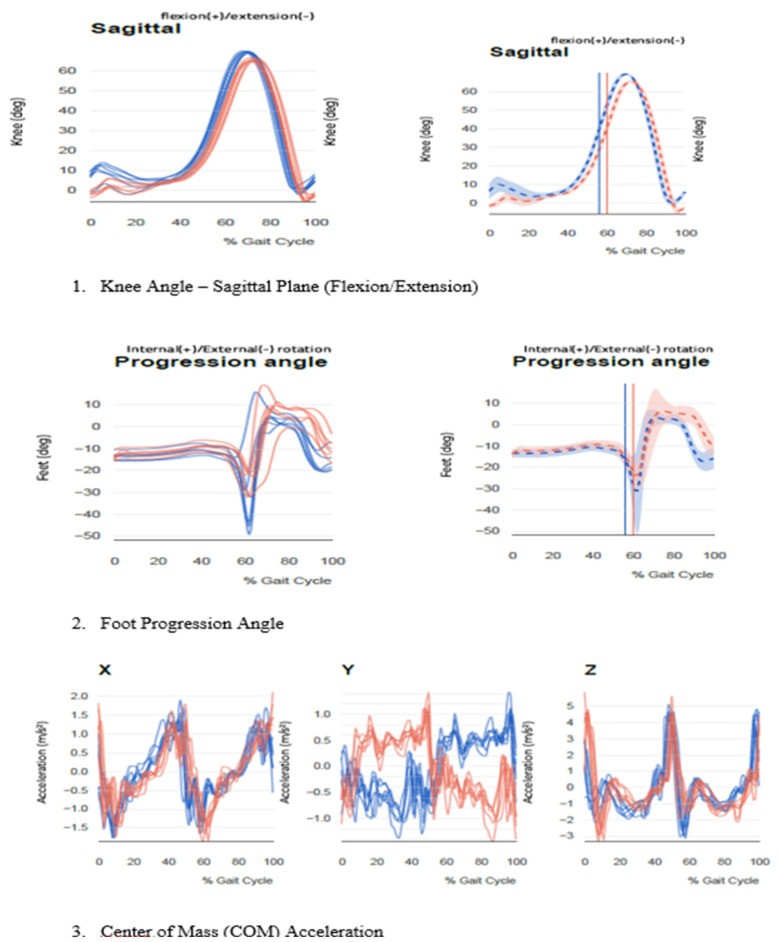 Figure 3
Figure 3 Figure 4
Figure 4| Domain | Assessment Tool/Method | Pre-Rehabilitation Findings | Post-Rehabilitation Findings | Interpretation |
|---|---|---|---|---|
| Pain | Numeric Pain Rating Scale (NPRS) | 7/10 during the activity | 0/10 during activity | Significant reduction in pain intensity |
| Knee ROM (Active) | Goniometer | 0°–90° | 0°–125° | Improved flexion range, nearing functional range |
| Extension Lag | Observation in a high sitting | 10° | 2° | Almost resolved; quadriceps strength improved |
| Quadriceps Strength | Manual Muscle Testing (MMT) | Grade 3+ | Grade 5 | Improved strength |
| Hip Abductor Strength | MMT | Grade 4 | Grade 5 | Full recovery in hip stability support |
| Patellar Mobility | Medial/lateral/superior glide palpation | Hypomobile (superior restriction) | Normalized mobility | Reduced risk of anterior knee pain recurrence |
| Joint Position Sense (JPS) | Goniometric repositioning task (30° angle) | 6.3° error | 2.1° error | Marked improvement in proprioceptive accuracy |
| Scar Sensitivity | Light touch, pressure palpation | Tender, hypersensitive over medial incision | None | Desensitization achieved |
| Kinesiophobia | Clinical interview (subjective) | Moderate fear of reinjury | None | Improved confidence in movement |
| Sensory Deficit | Monofilament, proprioception (manual) | Reduced light touch, altered proprioception over the peripatellar area | Intact | Suggests nerve recovery or cortical reorganization |
| Agility/Hop Test | Single-leg hop for distance | Unable to perform | Able to perform without compensation | Return of neuromuscular control and impact tolerance |
| Gait Parameter | Pre-Rehabilitation | Post-Rehabilitation | Normal Reference Range | Interpretation |
|---|---|---|---|---|
| Gait Speed | 0.96 m/s | 1.32 m/s | 1.2–1.4 m/s | Improved to normal; reflects restored confidence and propulsion |
| Cadence | 114.8 steps/min | 126.3 steps/min | 120–130 steps/min | Normal cadence regained, indicative of symmetrical limb movement |
| Step Length | L: 51.2 cm; R: 50.5 cm | L: 67.4 cm; R: 66.8 cm | 65–75 cm | Step symmetry and stride length normalized |
| Stance Phase | L: 39.5%; R: 43.6% | L: 59.3%; R: 60.1% | ∼60% | Balanced stance time, offloading corrected |
| Foot Strike Pattern | Toe strike bilaterally | Heel-to-toe | Heel-to-toe | Normalized strike pattern achieved |
| Peak Knee Flexion (Swing) | L: 69.7°; R: 66.4° | L: 78.2°; R: 76.9° | 75°–85° | Improved knee mobility during the swing phase |
| Knee Rotation | Excessive external rotation bilaterally | Mild ER within normal functional range | Neutral to mild ER | Compensation reduced; proprioception and control enhanced |
| Pelvic Obliquity | Elevated on the left side | Within 4° symmetry | <5° | Pelvic control restored |
| Foot Progression Angle | L: –50.3°; R: –32.7° | L: –13.2°; R: –11.6° | ∼10°–15° outward | Improved foot alignment reflects enhanced neuromuscular control |
| COM Acceleration | Reduced on the left side | Symmetric anterior-posterior shift | Symmetrical, stable | Restored balance and propulsion |
| Goal | Intervention | Rationale | Dosage & Frequency | Progression Criteria |
|---|---|---|---|---|
| Pain Management | Cryokinetics, TENS, Patellar taping, Soft tissue release | Alleviate discomfort, facilitate active participation | TENS: 10 min; Taping: 8 h max; Cryo: post-exercise | Pain 0/10 |
| Quadriceps Strength | TKE, Multi-angle SLR, Eccentric step downs, NMES | Restore extensor strength and patellar alignment | 3 × 10–15 reps; NMES 3x/week | Near-normal strength, no lag |
| ROM Restoration | Wall slides, Stationary cycling, MWM, Stretching | Achieve full flexion/extension without pain | ROM to 125° flexion within 6 weeks | Lag ≤2°, Flexion ≥125° |
| Core & Hip Control | Monster walks, Bridges, Side planks, Dead bug | Reduce dynamic valgus and trunk sway | 3 sets of 10–15, 3x/week | Maintained during single-leg tasks |
| VR-Enhanced Proprioception | Visual feedback balance tasks, Targeted movement control (via VR) | Increase accuracy in JPS, rebuild movement confidence | 20 min, 3x/week | JPS error ≤2.5° |
| Sensory Re-education | Texture desensitization, Tapping, Sensory discrimination tasks | Improve altered sensation and cutaneous awareness | 2x/day, 5–10 min | Return of intact sensation |
| Mindfulness Training | Breath focus, Body scan, Movement meditation | Reduce fear, enhance body awareness | 15 min/day, 5 days/week | Psychological readiness for loading |
| Functional Re-integration | Sit-to-stand, Walk-jog drills, Dynamic squats, Sports drills in VR | Reintroduce real-world activities and dynamic loads | Progressive, 10–30 min/day | Able to perform jog → sport-specific drills |
| Plyometric Agility | Double/single-leg hops, Crossover hops | Assess neuromuscular control and readiness to return | 3 × 5 reps, 3x/week | LSI ≥90%, no compensatory movement |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLower Extremity Biomechanics and Pathologies · Sports injuries and prevention · Knee injuries and reconstruction techniques
Introduction
1
Patellar instability is a common clinical concern in young, physically active populations, particularly athletes engaged in sports requiring rapid changes of direction, jumping, and deceleration, such as badminton, basketball, and soccer. Lateral patellar dislocation is the most frequent type, accounting for nearly 90% of cases, and often recurs if not managed appropriately (1–3). The incidence of first-time dislocation ranges from 5.8 to 77 per 100,000 persons per year, with adolescents and young athletes being most affected. Recurrence rates can be as high as 39%, particularly in individuals with anatomical or biomechanical risk factors (4, 5).
The medial patellofemoral ligament (MPFL) is the primary static stabilizer preventing lateral patellar displacement during the initial 30° of knee flexion. Injury to the MPFL occurs in nearly all first-time lateral dislocations, making it critical to assess and, when necessary, reconstruct during surgical intervention (6–8). Recurrent dislocations compromise patellofemoral congruency, damage articular cartilage, and predispose athletes to long-term complications such as early-onset osteoarthritis (9, 10). Predisposing factors include trochlear dysplasia, patella alta, increased tibial tubercle–trochlear groove distance, ligamentous laxity, and an elevated Q-angle, which increases lateral forces on the patella (11, 12).
High-demand sports like badminton impose significant biomechanical stress on the patellofemoral joint through high-speed lunges, multidirectional agility, eccentric loading, and single-leg landings (13–15). These activities require precise patellar tracking, neuromuscular control, and proprioception for both performance and injury prevention. Persistent instability can impair force generation, compromise alignment during rapid deceleration, and elevate the risk of re-injury, chronic pain, and kinesiophobia (16, 17).
This case is rare and clinically significant due to the combination of multiple factors: the patient is a national-level badminton athlete, experienced recurrent lateral patellar dislocations despite prior surgical intervention, sustained a subsequent traumatic patellar fracture, and had delayed or interrupted rehabilitation. These combined factors posed unique challenges for restoring knee function, proprioception, and return-to-sport capacity, distinguishing this case from typical patellar instability presentations.
The report details a phased, functionally graded, individualized rehabilitation protocol integrating pain management, neuromuscular retraining, plyometric control, proprioceptive re-education, and psychological readiness (18, 19). Clinical decisions were guided by objective outcome measures, including manual muscle testing, joint position sense, hop tests, the Balance Error Scoring System, agility assessments, and advanced biomechanical analysis using the Xsens motion capture system. These assessments provided quantitative data to guide progression, identify asymmetries, and validate readiness for high-demand athletic activity, emphasizing that optimal recovery in high-performance athletes involves not only tissue healing but also restoring confidence, coordination, and competitive readiness.
Case presentation
1.1
A 23-year-old male national-level badminton player presented to the Sports Physiotherapy Outpatient Department with persistent functional limitations following recurrent patellar dislocations and two surgical interventions. The patient provided informed consent for the use of clinical and therapeutic data for academic and publication purposes. He had no major comorbidities and had previously competed at the national level without limitations.
The initial injury occurred in April 2023 during a jump smash, leading to a spontaneous lateral patellar dislocation. Two recurrent dislocations followed in July 2023 and April 2024. MRI revealed a grade II medial patellofemoral ligament (MPFL) tear, and primary MPFL reconstruction using a semitendinosus graft was performed in May 2024. In July 2024, the patient sustained a patellar fracture during rehabilitation, necessitating a second surgery in August 2024 involving K-wire fixation and MPFL revision.
Post-surgical rehabilitation history
1.1.1
The patient underwent a standard early postoperative physiotherapy program from August to November 2024 (approximately 10–12 weeks). Early rehabilitation focused on edema control, pain management, gradual ROM recovery, and quadriceps activation. However, adherence fluctuated due to academic commitments and relocation, and he discontinued therapy prematurely in late November 2024 before reaching functional strengthening and sports retraining phases. Because rehabilitation stopped before advanced stages, the patient did not attempt a structured return-to-sport (RTS) and instead self-limited activity to basic ADLs.
Between December 2024 and April 2025, the athlete engaged only in intermittent home exercises without supervision. He reported progressive stiffness, difficulty with single-leg loading, avoidance of dynamic drills, and increasing apprehension during cutting or landing tasks. Persistent limitations affected university sports participation, prompting his orthopedic surgeon and team physiotherapist to refer him back for comprehensive reassessment and rehabilitation in May 2025.
Status at Re-presentation (Pre-intervention assessment)
1.1.2
On returning in May 2025, the patient demonstrated significant functional impairments, including Genu valgum and inability to squat, reduced running tolerance, inability to sit cross-legged, incomplete knee extension and flexion, altered infrapatellar sensation, and fear of dynamic movements. These deficits are summarized in Table 1, which details pre-intervention ROM, muscle strength, functional capacity, and kinesiophobia scores.
A detailed biomechanical evaluation and 3D gait analysis using the Xsens Motion Capture System were performed pre- and post-rehabilitation (Table 2). Pre-intervention findings included decreased stance phase duration, reduced peak knee flexion during swing, excessive foot external rotation, reduced propulsion symmetry, and altered COM acceleration patterns.
Figures 1, 2 display pre- and post-operative radiographs. Figure 3 illustrates pre- and post-rehabilitation Xsens gait changes, demonstrating:
- Improved sagittal knee kinematics, including recovery from terminal extension lag and greater peak flexion in swing.
- Reduced excessive external foot progression angle, indicating improved limb alignment and neuromuscular control.
- Restored COM vertical acceleration symmetry, reflecting improved gait stability and propulsion.
Shows the lateral x-ray of the left knee demonstrates a displaced transverse fracture of the patella, located at the mid-patellar level and there is displacement of fracture fragments, with the superior and inferior poles no longer in anatomical alignment.
Shows the radiographs reveal a previously displaced transverse fracture of the patella that has been surgically stabilized.
Gait analysis using Xsens motion capture pre- and post-rehabilitation. (1) Knee joint angle in the sagittal plane shows increased peak flexion during swing and improved terminal extension at heel strike, indicating recovery from extension lag and enhanced functional mobility. (2) Foot progression angle reveals a significant reduction in excessive external rotation post-rehabilitation, reflecting improved lower limb alignment and neuromuscular control. (3) Center of Mass (COM) acceleration in the vertical (Z) direction demonstrates restored propulsion symmetry and improved gait stability.
Intervention
1.2
A multimodal, phase-wise rehabilitation protocol was administered over 12 weeks, focusing on neuromuscular control, functional mobility, proprioceptive retraining, psychological readiness, and sports-specific reconditioning.
A head-mounted Oculus Quest VR system was used to deliver immersive rehabilitation tasks. The selected VR applications provided interactive, gamified movement training and simulated sport-specific environments. Tasks included:
- Visual feedback balance and coordination exercises (dynamic joint repositioning, obstacle avoidance).
- Sports-specific lower limb movements (single-leg stance control, multidirectional lunges, virtual agility drills).
- Cognitive-motor dual tasks to enhance neuromuscular coordination under mental load.
- Mindfulness modules incorporating guided breathing and grounding tasks in immersive VR landscapes to reduce kinesiophobia and promote body awareness. Session Frequency: 3 times per week.
Duration: 20–25 min per session.
Progression Criteria: Ability to perform dynamic drills confidently with accurate proprioceptive control and minimal compensations. Table 3 shows Structured Rehabilitation Interventions for Post-MPFL Reconstruction and Patellar Fracture.
Results
2
Following the implementation of a comprehensive rehabilitation protocol that included conventional physiotherapy, proprioceptive neuromuscular training, and immersive virtual reality (VR)-based therapy using Oculus Quest, the patient demonstrated substantial improvements across clinical, functional, psychological, and biomechanical parameters. As shown in Table 1, pain intensity during activities decreased from 7/10 to 0/10 on the Numeric Pain Rating Scale (NPRS), indicating complete pain resolution. Knee active range of motion improved from a restricted 0°–90° to a functional 0°–125°, and the observed extension lag reduced from 10° to just 2°, reflecting significant gains in quadriceps control and joint mobility.
Manual Muscle Testing (MMT) revealed strength recovery in both the quadriceps and hip abductors, with grades improving from 3+ and 4 to full strength (Grade 5), respectively. Proprioceptive accuracy, as measured through joint position sense (JPS), showed marked enhancement with a decrease in error from 6.3° to 2.1°. Patellar mobility normalized from an initially hypomobile superior glide restriction, reducing the risk of anterior knee stress recurrence. The patient also achieved full desensitization over previously hypersensitive surgical scars, along with restored light touch and proprioception around the peripatellar area, suggestive of peripheral nerve recovery or cortical reorganization. Notably, psychological improvements were observed, including the complete resolution of moderate kinesiophobia and a return of movement confidence.
Functionally, the patient progressed from being unable to perform a single-leg hop shown in Figure 4 to executing it without compensatory patterns, indicating restored neuromuscular control and impact tolerance. These findings are summarized in Table 1.
Assessment of hop test performance before rehabilitation.
Three-dimensional motion analysis conducted with Xsens technology. As illustrated in Figure 3, post-rehabilitation gait analysis revealed significant improvements in key biomechanical parameters. The knee sagittal angle (Figure 3.1) displayed a marked increase in peak flexion during the swing phase (from 66.4° to 76.9° on the right), and restoration of terminal extension at heel strike, reflecting enhanced quadriceps strength and reduced extension lag. The foot progression angle (Figure 3.2) improved notably, with external rotation reducing from −50.3° to −13.2° on the left side, indicating better limb alignment and dynamic control. Additionally, the COM vertical acceleration (Figure 3.3) exhibited more symmetrical and stable patterns across the gait cycle, suggesting restored balance and propulsion mechanics.
Further confirmed the biomechanical improvements achieved post-rehabilitation (Table 2). Gait speed increased from 0.96 m/s to 1.32 m/s, aligning with the normative range of 1.2–1.4 m/s. Cadence improved from 114.8 to 126.3 steps/min, and step length increased bilaterally (L: 51.2 cm–67.4 cm; R: 50.5 cm–66.8 cm), indicating improved stride symmetry and propulsion mechanics. Stance phase distribution, previously asymmetrical (L: 39.5%; R: 43.6%), was normalized to 59.3% and 60.1%, respectively. The patient's foot strike pattern shifted from a compensatory toe strike bilaterally to a heel-to-toe pattern, and peak knee flexion during the swing phase improved bilaterally, approaching the normative range of 75°–85°. Abnormal external knee rotation, elevated pelvic obliquity, and altered foot progression angles (L: −50.3°; R: −32.7°) all normalized post-intervention, indicating enhanced limb alignment and motor control. Center of mass acceleration, previously reduced on the left side, became symmetrical, reflecting improved balance and coordinated propulsion.
The integration of immersive VR training via Oculus Quest further supported neuromuscular re-education and psychological engagement. Virtual rehabilitation tasks simulated dynamic sporting scenarios, enabling safe, graded exposure to movement, which contributed to improved proprioceptive feedback, sensory integration, and movement confidence. The patient showed increased responsiveness during virtual body-awareness tasks and improved agility and reaction time during virtual sports drills, suggesting the effectiveness of VR in bridging the gap between clinic-based therapy and sport-specific demands.
Patient-reported outcome measures also reflected significant recovery. The KOOS score increased from 62 to 100, indicating complete functional normalization across pain, symptoms, activities of daily living, and sport/recreation subscales. The Lower Extremity Functional Scale (LEFS) improved from 55 to 80, reflecting near-complete restoration of lower limb function. Moreover, the Tampa Scale for Kinesiophobia (TSK) decreased from 68 to 30, denoting a reduction in fear-avoidant behaviors and enhanced psychological readiness for return to sport.
Taken together, these outcomes—supported by data from Tables 1, 2—highlight the effectiveness of a comprehensive, individualized rehabilitation program incorporating conventional physiotherapy, technology-assisted VR, proprioceptive training, and psychological support in facilitating successful recovery and return to sport following MPFL reconstruction and patellar fracture fixation.
Discussion
3
Recurrent patellar dislocation is a debilitating condition, particularly among young athletes engaged in high-impact, multi-directional sports such as badminton, which demands rapid acceleration, deceleration, sudden directional changes, jumping, and landing (20, 21). These complex movement patterns require optimal joint alignment, proprioceptive acuity, and neuromuscular coordination. Any instability in the patellofemoral joint compromises the kinetic chain, leading to compensatory mechanisms and increasing the risk of further injuries or performance deficits.
This case is clinically significant because it illustrates the compounded challenges following recurrent patellar dislocations, MPFL insufficiency, and subsequent complications, including a patellar fracture. Such injuries result in structural deficits (e.g., patellar maltracking, reduced mobility), neuromuscular dysfunction (e.g., quadriceps weakness, extension lag), proprioceptive disturbances, and psychological barriers such as kinesiophobia. Consequently, the athlete's confidence, agility, and functional performance were markedly reduced.
Traditional rehabilitation methods for recurrent patellar instability generally focus on quadriceps strengthening, VMO activation, proprioceptive exercises, and gradual return-to-sport drills. Early mobilization and progressive resistance training are emphasized to prevent stiffness, quadriceps inhibition, and maltracking (22–26). Studies by Nomura et al. and Sappey-Marinier et al. highlight the importance of timely rehabilitation, VMO activation, and patellar alignment exercises to support ligament healing (27, 28). Standard functional criteria, such as limb symmetry index (LSI) > 90% and functional testing (Hop tests, T-Test, BESS), are commonly used to guide safe return to sport (29).
However, in this case, post-operative immobilization due to a patellar fracture, along with delayed or interrupted rehabilitation, led to pronounced quadriceps atrophy, proprioceptive deficits, and functional decline. These challenges deviated from standard recovery trajectories and required a more nuanced, multidisciplinary approach.
Enhanced rehabilitation strategy in this case
3.1
A phased, individualized protocol addressed both biomechanical and biopsychosocial factors. Interventions included VMO activation, neuromuscular electrical stimulation, proprioceptive retraining, agility drills, mindfulness training, and functional testing. Early identification of sensory deficits and asymmetries enabled tailored intervention planning. Immersive Virtual Reality (VR) using Oculus Quest was integrated in later phases to simulate high-speed, dynamic sports environments, improve motor planning, enhance sensory integration, and reduce kinesiophobia. This innovative approach complemented traditional methods, providing engagement, neuroplasticity benefits, and confidence-building, which are often not addressed in conventional rehabilitation.
Gait analysis using Xsens confirmed biomechanical recovery, with improvements in gait speed, cadence, stride length, foot progression angles, and center-of-mass acceleration. These improvements reflected restored neuromuscular symmetry, motor relearning, and readiness for return to play.
Psychological and neurological components were systematically addressed through mindfulness, functional exposure, and sensory re-education. These interventions were critical in overcoming fear of re-injury, altered infrapatellar sensation, and proprioceptive errors—factors often underreported in patellofemoral injury literature but pivotal in this case.
Key challenges included:
- Delayed rehabilitation post-MPFL reconstruction, causing missed conditioning opportunities.
- Surgical re-intervention and immobilization leading to quadriceps inhibition and scar formation.
- Psychological barriers limiting early progression.
- Sensory impairments affecting postural control and agility.
- Need for cautious, individualized return-to-sport criteria due to layered impairments. Key lessons and clinical implications:
- Rehabilitation must be athlete-specific, goal-oriented, and incorporate psychosocial components.
- Delayed or incomplete rehabilitation increases risk of functional decline and re-injury.
- Functional and sensory testing should be embedded into clinical pathways for decision-making.
- Interdisciplinary collaboration among orthopedic surgeons, physiotherapists, and sports psychologists enhances outcomes.
- Technology-based tools, such as VR and motion analysis systems (e.g., Xsens), provide objective, engaging platforms to complement traditional rehabilitation and facilitate neuro-muscular recovery.
Limitations and contingency
3.2
This case report has several inherent limitations. First, as a single-case study, the findings may not be generalizable to all athletes or patients with recurrent patellar dislocation and post-surgical complications. Second, the absence of a control or comparison group limits the ability to definitively attribute improvements solely to the VR-assisted or multidisciplinary interventions. Third, some assessments, such as psychological readiness and proprioception, may be influenced by subjective factors, despite using validated scales.
Contingency planning was critical throughout rehabilitation. Potential setbacks—including delayed healing, post-surgical complications, quadriceps inhibition, and kinesiophobia—were mitigated through phased, individualized interventions, frequent monitoring of functional and biomechanical parameters, and adjustments to exercise intensity. Close collaboration with orthopedic surgeons, physiotherapists, and sports psychologists allowed for rapid response to emerging issues, ensuring safe progression and minimizing the risk of re-injury.
Overall, while this case provides valuable insights into complex knee rehabilitation, caution is advised in extrapolating these findings beyond similar clinical scenarios, and further studies with larger cohorts are warranted to validate these outcomes.
Conclusion
4
This case highlights the clinical complexity of recurrent patellar dislocation complicated by MPFL insufficiency, reconstruction, and traumatic patellar fracture in a competitive athlete. Individualized, multidisciplinary rehabilitation including strength training, proprioceptive retraining, mindfulness, and VR-assisted interventions led to meaningful improvements in pain, range of motion, muscle strength, proprioception, psychological readiness, and functional performance. Objective measures (KOOS, LEFS, TSK, JPS error, gait metrics) confirmed recovery and guided safe return-to-play. The case underscores the value of evidence-based, technology-enhanced rehabilitation and the importance of timely, goal-directed interventions for successful reintegration into high-performance sport.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Parikh SN Veerkamp M Redler LH Schlechter J Williams BA Yaniv M Patellar instability in young athletes. Clin Sports Med. (2022) 41(4):627–51. 10.1016/j.csm.2022.05.00536210163 · doi ↗ · pubmed ↗
- 2Dennis ER Gruber S Marmor WA Shubin Stein BE. Evaluation and management of patellar instability. Ann Joint. (2022) 7:2. 10.21037/aoj-2020-02PMC 1092928138529132 · doi ↗ · pubmed ↗
- 3Adachi N. Diagnosis and treatment of patellar instability. Orthop J Sports Med. (2024) 12(10 Suppl 3):2325967124 S 00382. 10.1177/2325967124 S 00382 · doi ↗
- 4Vermeulen D van der Valk MR Kaas L. Plaster, splint, brace, tape or functional mobilization after first-time patellar dislocation: what’s the evidence? EFORT Open Rev. (2019) 4(3):110–4. 10.1302/2058-5241.4.18001630993012 PMC 6440297 · doi ↗ · pubmed ↗
- 5Olds M Ellis R Donaldson K Parmar P Kersten P. Risk factors which predispose first-time traumatic anterior shoulder dislocations to recurrent instability in adults: a systematic review and meta-analysis. Br J Sports Med. (2015) 49(14):913–22. 10.1136/bjsports-2014-09434225900943 PMC 4687692 · doi ↗ · pubmed ↗
- 6Krebs C Tranovich M Andrews K Ebraheim N. The medial patellofemoral ligament: review of the literature. J Orthop. (2018) 15(2):596–9. 10.1016/j.jor.2018.05.0029881201 PMC 5990246 · doi ↗ · pubmed ↗
- 7Luxenburg D Rizzo MG. Anatomy, bony pelvis and lower limb: medial patellofemoral ligament. In: Stat Pearls. Treasure Island (FL): Stat Pearls Publishing (2023).35593802 · pubmed ↗
- 8Huber C Zhang Q Taylor WR Amis AA Smith C Hosseini Nasab SH. Properties and function of the medial patellofemoral ligament: a systematic review. Am J Sports Med. (2020) 48(3):754–66. 10.1177/036354651984130431091114 · doi ↗ · pubmed ↗