From criminalization to care: a comparative rights-based policy review of HIV responses in South Asia
Praveen Hoogar

TL;DR
This paper reviews HIV responses in South Asia through a rights-based approach, highlighting the need to replace punitive laws with care-focused policies to improve health outcomes.
Contribution
The study introduces a comparative rights-based policy framework to evaluate and guide HIV responses in South Asia.
Findings
India and Nepal show better HIV outcomes where rights-based legal reforms have been implemented.
Criminalization of sex work and drug use persists across all four countries, hindering progress.
Structural barriers like stigma and limited service access are common across South Asia.
Abstract
South Asia faces concentrated HIV epidemics rooted in legal and social marginalization of key populations. Laws criminalizing same-sex relations, sex work, and drug use, combined with gaps in anti-discrimination protections and funding constraints for civil society organizations, undermine progress toward the UNAIDS 95-95-95 targets. This review applies a rights-based approach (RBA) to compare national policies and outcomes across India, Nepal, Pakistan, and Sri Lanka, and offers actionable regional guidance. A comparative analysis was performed using a five-dimension RBA framework: legal decriminalization, anti-discrimination protections, service access, community participation, and HIV outcomes. Data were synthesized from national legal documents, UNAIDS and Global Fund reports, published research, and community organization perspectives. Comparative findings are presented in a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1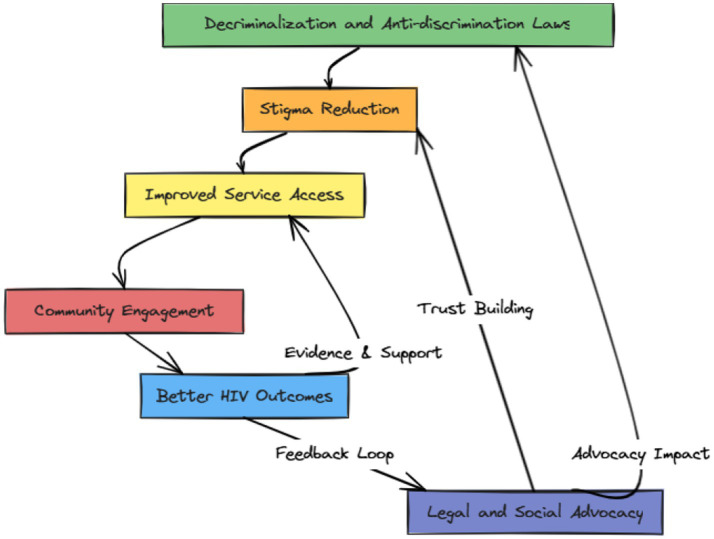 Figure 2
Figure 2| Dimension | India | Nepal | Pakistan | Sri Lanka |
|---|---|---|---|---|
| Legal decriminalization | Decriminalized same-sex conduct (2018); sex work and drug use remain criminalized under ITPA and NDPS Act; legal ambiguity on transgender sex work ( | No criminalization of same-sex relations; third gender legally recognized; interim recognition of same-sex marriage ( | Section 377 and Hudood laws criminalize same-sex relations, sex work, drug use; transgender protections under review ( | Colonial-era criminalization of same-sex conduct and sex work; no gender identity recognition ( |
| Anti-discrimination protections | HIV/AIDS Act (2017) prohibits discrimination in healthcare, employment, housing; lacks enforcement and SOGI coverage ( | Constitutional equality clauses cover SOGI; Gender and Sexual Minorities Rights Act stalled ( | Transgender Persons Act (2018) progressive but challenged; no protection for other key groups ( | No HIV or SOGI-specific protections; occasional narrow judicial relief ( |
| Service access | 1,700+ ART centers; PrEP pilots; harm reduction legal but police obstruct; PMTCT gaps in rural areas ( | District-level ART; NGO mobile testing; limited PrEP; harm reduction in cities; PMTCT gender bias constraints ( | Donor-dependent ART; no PrEP; fragmented harm reduction; PMTCT stigma and infrastructure gaps ( | Stable state-run ART; no PrEP/OST; centralized services; provider stigma deters key populations ( |
| Community participation | CSOs (Naz, DMSC) deliver services; FCRA restricts foreign funding; limited state planning inclusion ( | BDS, SPARSHA, YKP lead peer outreach; donor dependence; uneven provincial rollout ( | CSOs (Naz Male Health Alliance, GIA) under legal threat; 5% HIV budget for community services ( | Equal Ground, COJ consulted; no state funding; implementation roles minimal ( |
| HIV outcomes (95-95-95) | 81% diagnosed, 88% on ART, 97% suppressed; rural/trans gaps remain ( | ~80% ART coverage; data gaps on testing/suppression; strong NGO-supported outcomes ( | 48% diagnosed, 32% on ART; data missing on suppression; rising incidence among PWID/trans women ( | 82-86-85 cascade; lack of disaggregation masks criminalized group outcomes ( |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSex work and related issues · HIV/AIDS Research and Interventions · African Sexualities and LGBTQ+ Issues
Introduction
1
South Asia confronts a persistent HIV epidemic characterized by concentrated transmission among criminalized and marginalized populations, including men who have sex with men (MSM), sex workers, people who inject drugs (PWID), and transgender individuals. Despite regional adult HIV prevalence remaining below 1%, key population prevalence rates reach alarming levels—up to 29% among PWID in certain areas and 26% among MSM in urban centers. This epidemiological pattern reflects not merely biological vulnerability but the profound impact of punitive legal frameworks and discriminatory social structures that systematically exclude the most at-risk groups from life-saving services (1–3).
The relationship between law, human rights, and HIV outcomes has gained international recognition as a critical determinant of epidemic control. UNAIDS and the Global Commission on HIV and the Law demonstrate that countries criminalizing same-sex conduct show 11% lower HIV status awareness and 8% lower viral suppression rates compared to non-criminalizing jurisdictions. Similarly, criminalization of sex work correlates with 10% reduced status awareness and 6% lower viral suppression, while drug use criminalization associates with 14% poorer performance across both indicators. These findings underscore that achieving the UNAIDS 95-95-95 targets—95% of people living with HIV knowing their status, 95% of those diagnosed receiving antiretroviral therapy, and 95% of those on treatment achieving viral suppression—requires fundamental transformation of legal and policy environments (4–7).
The rights-based approach (RBA) to HIV has emerged as the predominant framework for addressing these structural determinants. Grounded in international human rights law and operationalized through UNAIDS guidance, the RBA recognizes that sustainable epidemic control demands enabling legal environments, meaningful community participation, protection from discrimination, and accessible services for all populations regardless of social status. The approach explicitly links health outcomes to social justice, emphasizing that HIV responses must simultaneously advance public health goals and uphold human dignity (7–10).
South Asia presents a compelling regional case study for examining rights-based HIV governance due to shared colonial legal inheritances that continue to criminalize key populations, coupled with diverse contemporary trajectories in legal and policy reform. India’s landmark 2018 Supreme Court decision in Navtej Singh Johar v. Union of India decriminalized same-sex conduct, representing a watershed moment for LGBTI rights in the region. Nepal’s 2015 constitution includes progressive provisions recognizing sexual and gender minorities, while its 2023 interim court recognition of same-sex marriage signals continued advancement. However, these progressive developments coexist with persistent criminalization of sex work and drug use across all South Asian countries, creating fragmented legal landscapes that complicate service delivery and rights protection (9–12).
Pakistan illustrates the complexity of legal reform in conservative contexts, where the 2018 Transgender Persons (Protection of Rights) Act represents some of the world’s most comprehensive transgender protections, yet faces implementation challenges amid religious opposition and judicial review. Meanwhile, Sri Lanka maintains colonial-era criminalization of same-sex conduct and sex work despite achieving relatively stable HIV epidemic indicators, highlighting the nuanced relationships between legal environments and health outcomes (13, 14).
This comparative review examines HIV policy environments across India, Nepal, Pakistan, and Sri Lanka through a structured rights-based framework encompassing five interdependent dimensions: legal decriminalization, anti-discrimination protections, service access, community participation, and HIV outcomes. These countries represent approximately 80% of South Asia’s HIV burden and offer diverse legal and political contexts for assessing how rights-based governance influences epidemic control (15, 16).
The study addresses three critical research questions that directly inform policy and practice. First, how do varying degrees of legal decriminalization affect HIV service uptake and health outcomes among key populations? Evidence suggests that removing punitive laws increases healthcare system trust and service utilization, but the mechanisms and magnitude of these effects require systematic examination. Second, what institutional arrangements and enforcement mechanisms are necessary to translate anti-discrimination legislation into meaningful protection for people living with HIV and key populations? Laws without implementation represent hollow victories that may actually worsen outcomes by creating false expectations. Third, how can community participation be meaningfully institutionalized within national HIV responses to ensure that affected populations drive policy and program development? Global evidence demonstrates that community-led interventions achieve superior outcomes, yet most national responses remain top-down and professionally dominated (17–19).
The analysis is particularly timely as countries approach the 2025 deadline for achieving 95-95-95 targets and negotiate post-2025 global AIDS strategies. Regional progress has been uneven, with India reporting 81-88-97% cascade achievement while Pakistan lags at 48-32-unknown%, largely reflecting differential attention to legal and structural barriers. Understanding the causal pathways between rights-based governance and epidemic control provides evidence-based guidance for legal reform, resource allocation, and program design that extends beyond South Asia to similar epidemiological and legal contexts worldwide (20–23).
The COVID-19 pandemic has further exposed and exacerbated existing vulnerabilities among criminalized populations, making rights-based approaches even more urgent. Lockdowns and enhanced law enforcement have disrupted harm reduction services, increased police harassment of sex workers and PWID, and limited access to HIV testing and treatment. These disruptions disproportionately affect precisely those populations that face the highest HIV burden, reinforcing the centrality of legal and structural interventions to epidemic resilience (24–26).
This review contributes to both HIV policy scholarship and practical governance by operationalizing the rights-based approach through measurable indicators that can guide policy development and program implementation. Unlike previous analyses that focus on single countries or isolated legal reforms, this comparative approach identifies cross-cutting patterns and divergent strategies that illuminate both opportunities and constraints for rights-based HIV responses in diverse political contexts. The findings have immediate relevance for national AIDS programs, civil society organizations, international donors, and regional bodies seeking to accelerate progress toward epidemic control while advancing social justice and human rights (22, 23, 27).
Methods
2
Conceptual framework
2.1
This study operationalizes the rights-based approach (RBA) to HIV through a five-dimensional analytical framework synthesized from international human rights law, public health scholarship, and UNAIDS technical guidance. The RBA framework recognizes that effective HIV responses require addressing structural determinants of vulnerability, ensuring meaningful participation of affected communities, and protecting human dignity alongside achieving biomedical outcomes (28–30).
The five interdependent dimensions are:
Legal Decriminalization encompasses the removal or non-enforcement of punitive laws criminalizing same-sex relations, sex work, or drug use—behaviors often associated with elevated HIV risk among key populations. Decriminalization is hypothesized to enhance trust in healthcare systems, reduce stigma, and improve service uptake (31, 32).Anti-Discrimination Protections include constitutional provisions, statutory frameworks, and enforcement mechanisms that prohibit discrimination against people living with HIV (PLHIV) and key populations in healthcare, employment, housing, education, and other essential services. Effective protections require both legal text and institutional capacity for implementation (33, 34).Service Access encompasses availability, accessibility, acceptability, and quality of HIV prevention (PrEP, harm reduction), diagnostic (testing), treatment (ART), and care services, with particular attention to integration within broader health systems and tailored approaches for marginalized populations (35, 36).Community Participation refers to meaningful involvement of civil society organizations (CSOs) and affected populations in policy formulation, program design, implementation, monitoring, and advocacy, including adequate funding, legal space for operation, and genuine decision-making authority (5, 37).HIV Outcomes are measured through the UNAIDS 95-95-95 cascade indicators—percentage of PLHIV aware of their status, percentage of diagnosed individuals on antiretroviral therapy, and percentage of those on treatment achieving viral suppression—alongside epidemiological indicators including incidence, prevalence, and mortality, with disaggregation by key population groups where data permit (38, 39).
Country selection and rationale
2.2
India, Nepal, Pakistan, and Sri Lanka were selected through purposive sampling based on four criteria. First, all four countries experience concentrated HIV epidemics with prevalence exceeding 5% among at least one key population group, enabling examination of interventions targeting most-affected communities. Second, shared colonial legal heritage has resulted in similar criminalization patterns, particularly regarding same-sex conduct, providing comparable baseline legal frameworks. Third, divergent trajectories in contemporary legal reform—ranging from India’s decriminalization of same-sex conduct to Sri Lanka’s retention of colonial-era statutes—offer variation in the independent variable of interest. Fourth, collective representation of approximately 80% of South Asia’s HIV burden ensures regional relevance and policy impact (29, 30, 40–42).
Data sources and collection strategy
2.3
The review covered materials published and available between 2010 and 2024, reflecting the most active phase of rights-based and decriminalization reforms in the region. Where official policy or legal documents were not publicly accessible, information was cross-verified using secondary institutional sources and peer-reviewed publications to ensure completeness and accuracy. Data collection employed a systematic and multi-source approach to ensure comprehensiveness and reliability. Legal and policy documents included national constitutions, penal codes, HIV-specific legislation, national strategic plans, and related regulatory frameworks, accessed through government websites, legal databases, and policy repositories. Programmatic data were drawn from National AIDS Control Organization reports, UNAIDS country profiles and Global AIDS Monitoring reports, Global Fund grant documents and implementation letters, and WHO HIV country profiles. Published research comprised peer-reviewed articles identified through structured searches of PubMed, Scopus, and regional databases using terms combining “HIV,” “law,” “discrimination,” “key populations,” and country names, supplemented by grey literature from international organizations. Community perspectives were incorporated through published reports, advocacy documents, and policy submissions by leading regional CSOs, including Naz Foundation (India), Blue Diamond Society (Nepal), Naz Male Health Alliance (Pakistan), and Equal Ground (Sri Lanka) (35, 43–45).
The present study employed a narrative comparative review design, which allows for the integration of heterogeneous evidence—legal texts, policy frameworks, programmatic reports, and community perspectives—within a unified analytical lens. This approach is particularly suited to exploring complex, intersectional, and context-dependent relationships between law, ethics, and HIV governance that may not be fully captured through quantitative synthesis. It also contributes to theory development by linking policy evolution with rights-based and ethical frameworks across diverse socio-legal settings in South Asia.
Analytical approach
2.4
Analysis followed a structured comparative case study methodology. Document review and thematic coding were conducted using NVivo 12 software, with legal texts, policy documents, and research literature coded against the five RBA dimensions using both deductive codes derived from the conceptual framework and inductive codes emerging from the data. Cross-country comparison employed a constant comparative method to identify patterns, divergences, and causal relationships across dimensions and countries. Data triangulation verified findings by comparing information across source types, with particular attention to identifying consistencies and discrepancies between official policy documents and community organization assessments. The analysis culminated in development of a comparative assessment matrix (Table 1) summarizing key findings across all dimensions and countries, and a conceptual pathway diagram (Figures 1, 2) illustrating theorized relationships between RBA implementation and HIV outcomes (5, 36–39).
The rights-based HIV response circle (conceptual pathway diagram). Created by Praveen Hoogar.
Policy-outcome causal pathway. Created by Praveen Hoogar.
The RBA framework is visualized in two conceptual diagrams.
Results
3
Overview of rights-based approach implementation
3.1
The comparative analysis reveals significant heterogeneity in rights-based HIV policy implementation across South Asia, with countries demonstrating varied progress across the five analytical dimensions. India and Nepal exhibit partial advancement in legal decriminalization and constitutional protections, while Pakistan and Sri Lanka maintain more restrictive legal frameworks despite pockets of progressive legislation. All four countries demonstrate persistent gaps in enforcement mechanisms, funding allocation for community participation, and service accessibility for criminalized populations (46, 47).
Cross-cutting patterns emerge across the region. First, colonial-era legal frameworks continue to influence contemporary HIV policy environments, with Section 377 derivatives and vagrancy laws serving as primary instruments of criminalization. Second, civil society organizations function as de facto service providers filling state capacity gaps, yet operate under increasing legal and financial constraints. Third, urban–rural disparities in service access reflect broader health system inequalities, with key populations in remote areas facing compounded marginalization. Fourth, women within key population groups—female sex workers, women who inject drugs, and transgender women—experience intersectional discrimination that compounds HIV vulnerability.
Comparative assessment by dimension
3.2
Comparative assessment of rights-based HIV policy dimensions in South Asia shown in Table 1.
Legal decriminalization: progress and persistent barriers
3.3
India’s Navtej Singh Johar judgment decriminalized same-sex conduct in 2018, affirming privacy and dignity rights (14). However, sex work and drug use remain criminalized under separate statutes, producing a patchwork legal environment hindering universal service access (48). Nepal’s constitution enshrines non-discrimination for sexual and gender minorities, supplemented by judicial recognition of third gender and same-sex marriage in principle, yet lacks comprehensive implementing legislation (16, 49). Pakistan’s Transgender Persons Act offers broad protections but coexists with criminalization of MSM, sex workers, and PWID under penal and Hudood statutes, limiting its practical impact (50, 51). Sri Lanka’s colonial-era penal provisions continue unaltered, creating a hostile environment that deters service uptake despite robust general population services (52, 53).
Anti-discrimination protections: implementation gaps
3.4
India’s HIV/AIDS Act of 2017 prohibits discrimination but lacks robust enforcement mechanisms and omits explicit SOGI protections, undermining its efficacy (8, 54). Nepal’s constitutional guarantees remain largely aspirational without dedicated statutes or enforcement bodies (55, 56). Pakistan’s transgender law mandates non-discrimination for transgender persons, but legislative contestation and limited resources for oversight weaken its enforcement (50, 51). Sri Lanka lacks targeted legal protections, relying on ad hoc court rulings to address HIV-related discrimination (57, 58).
Service access: uneven progress and structural barriers
3.5
India’s decentralized ART network and emerging PrEP programs offer a model for integration, yet rural and gender-diverse populations face discrimination and policing barriers at harm reduction sites (55, 59). Nepal’s NGO-led mobile testing expands outreach but sustainability hinges on continued donor support (60, 61). Pakistan’s donor-reliant services and absence of PrEP perpetuate low coverage and retention, while Sri Lanka’s centralized, stigma-prone system excludes nocturnal and mobile key populations (62–64).
Community participation: constrained but critical
3.6
CSOs are critical service providers across the region; however, legal restrictions on foreign funding (India’s FCRA), donor dependence (Nepal, Pakistan), and lack of state support (Sri Lanka) curtail their scale and influence (61, 65–68). Evidence shows that properly resourced community-led responses outperform top-down models in achieving cascade targets among key populations (15, 69).
Practical strategies
4
The comparative analysis reveals four strategic pillars essential for advancing rights-based HIV responses in South Asia. These evidence-based recommendations address immediate implementation gaps while establishing foundations for long-term epidemic control and social justice advancement. Each pillar integrates lessons from successful interventions globally and regional innovations, providing actionable guidance for policymakers, program implementers, and civil society organizations (70).
Legal reform and decriminalization
4.1
Immediate actions (1–2 years)
4.1.1
Legal audits should be conducted across all four countries to identify discriminatory statutes, regulations, and enforcement practices that impede HIV service access (71). These assessments must engage legal experts, affected communities, and health practitioners to document gaps between law and practice. Judicial and law enforcement sensitization programs should be implemented, drawing on successful models from Thailand and the Philippines where targeted training reduced discriminatory enforcement (46, 72).
Non-enforcement policies for health-seeking behaviors represent achievable interim measures. Portugal’s decriminalization model demonstrates that redirecting law enforcement resources from criminalization to health support can reduce HIV incidence by up to 18% within 5 years (73). South Asian countries should pilot designated safe zones around healthcare facilities and harm reduction sites, with clear protocols prohibiting arrests for possession of small quantities of drugs or condoms (74).
Medium-term reforms (3–5 years)
4.1.2
Comprehensive legal reform requires sustained political commitment and strategic litigation. India’s successful Section 377 challenge provides a regional template for constitutional arguments based on dignity, privacy, and equality (14). Similar strategic litigation should be pursued in Sri Lanka and Pakistan, supported by regional legal networks and international human rights organizations (75).
Gender recognition frameworks should be expanded beyond Pakistan’s model to all countries, incorporating self-identification principles and comprehensive anti-discrimination protections (76). Nepal’s constitutional provisions provide strong foundations for implementing legislation that covers all sexual and gender minorities (77). Regional harmonization of legal standards can accelerate domestic reform processes through peer learning and shared advocacy (78).
Long-term vision (5+ years)
4.1.3
Full decriminalization of same-sex conduct, sex work, and drug use represents the ultimate goal for enabling HIV responses. Evidence from multiple jurisdictions shows that decriminalization reduces HIV incidence by 20%–33% among key populations within a decade (6). Regional coordination through SAARC or similar mechanisms should establish common legal frameworks and mutual recognition of legal protections for mobile populations (66).
Human rights monitoring mechanisms must be strengthened through national human rights institutions with specific mandates for HIV and LGBTI issues (79). These bodies should have investigative powers, complaint procedures, and authority to recommend legal and policy reforms. Parliamentary committees on health and human rights should conduct regular reviews of discriminatory laws and their health impacts (80).
Health system transformation
4.2
Immediate actions (1–2 years)
4.2.1
Service decentralization and integration represent urgent priorities for improving access among marginalized populations. Community health worker programs should be expanded to include HIV testing, counseling, and adherence support, following successful models from Rwanda and Malawi (81, 82). Mobile testing units operated by civil society organizations should receive government funding and legal authorization to operate without harassment (83).
Healthcare worker training on non-discrimination and cultural competency must be mandated and regularly refreshed. Evidence from multiple settings shows that structured sensitization programs can reduce healthcare stigma by 40%–60% when implemented systematically (84). Training curricula should address unconscious bias, legal obligations, and clinical best practices for serving key populations (85).
Differentiated service delivery models should be rapidly scaled, including extended dispensing intervals, community-based distribution, and self-testing programs (86). These approaches have demonstrated superior retention and viral suppression outcomes among key populations while reducing healthcare system burden (87).
Medium-term reforms (3–5 years)
4.2.2
Universal access to pre-exposure prophylaxis (PrEP) should be achieved for all key populations, following WHO guidelines and successful implementation experiences from Thailand, Kenya, and Brazil (62, 88). Financing mechanisms should combine government funding, international support, and innovative approaches such as social insurance schemes (89).
Comprehensive harm reduction services must be scaled to reach at least 80% of people who inject drugs, incorporating opioid substitution therapy, needle-syringe exchange, overdose prevention, and integrated healthcare (63). Legislative reforms should remove barriers to harm reduction implementation, including prescription requirements and facility licensing restrictions (90).
Mental health and gender-affirming care should be integrated into HIV services, addressing the psychosocial needs that often complicate treatment adherence (91). Training programs for healthcare providers should include competencies in trauma-informed care, gender dysphoria management, and substance use disorders (92).
Long-term vision (5+ years)
4.2.3
Universal health coverage frameworks should explicitly include HIV prevention, testing, treatment, and care services with guaranteed access regardless of legal status, documentation, or social identity (94). Financial protection mechanisms should eliminate user fees and transportation barriers that disproportionately affect marginalized populations (95).
Quality assurance systems must ensure that services meet international standards for clinical care, human rights compliance, and patient satisfaction (96). Regular audits should assess discrimination, waiting times, and treatment outcomes across different population groups (97). Performance-based financing should incentivize providers to achieve equity indicators alongside clinical targets (98).
Funding equity and community empowerment
4.3
Immediate actions (1–2 years)
4.3.1
Budget allocations for key population programs should be increased to minimum thresholds of 30% of total HIV spending, consistent with UNAIDS recommendations and epidemiological evidence (99). Transparent budgeting processes should engage affected communities in priority-setting and resource allocation decisions (100).
Civil society capacity building programs should receive sustained funding to strengthen organizational development, financial management, and advocacy capabilities (101). South–South learning exchanges should facilitate knowledge transfer between successful community organizations across the region (102).
Legal reforms should remove barriers to civil society operations, including foreign funding restrictions, registration requirements, and reporting obligations that impede service delivery (103). India’s FCRA revisions and similar restrictions in other countries require immediate review and liberalization (65).
Medium-term reforms (3–5 years)
4.3.2
Sustainable financing mechanisms should reduce dependence on international donors through domestic resource mobilization, innovative financing instruments, and social enterprise development (104). Community-led organizations should receive multi-year funding commitments that enable long-term planning and program continuity (105).
Institutional frameworks for community participation should be established within national AIDS programs, including reserved seats on governing boards, formal consultation mechanisms, and community scorecards for program monitoring (106). These structures should have decision-making authority rather than merely advisory roles (107).
Long-term vision (5+ years)
4.3.3
Community-led responses should become the dominant model for key population programs, with civil society organizations receiving direct funding and implementation authority (101). Global Fund and other donors increasingly recognize community leadership as essential for achieving epidemic control (108).
Social enterprise development should enable community organizations to generate revenue through fee-for-service arrangements, social businesses, and cooperative enterprises (109). This diversification reduces donor dependence while building organizational sustainability (110).
Regional collaboration and knowledge sharing
4.4
Immediate actions (1–2 years)
4.4.1
A South Asia Rights-Based HIV Policy Forum should be established under joint SAARC-UNAIDS auspices to facilitate policy dialogue, technical assistance, and advocacy coordination ADDIN. This platform should convene policymakers, civil society leaders, and technical experts for regular knowledge exchange.
Cross-border collaboration protocols should be developed for high-mobility populations, including migrant workers, sex workers, and people who inject drugs. These agreements should ensure continuity of HIV services and mutual recognition of treatment records across national boundaries.
Medium-term reforms (3–5 years)
4.4.2
Regional monitoring frameworks should harmonize indicators, data collection methods, and reporting standards to enable comparative analysis and peer learning. Technical assistance mechanisms should support countries with weaker systems to adopt best practices from regional leaders.
Joint advocacy campaigns should address shared challenges such as colonial-era laws, religious opposition, and donor funding constraints. Regional coalitions of civil society organizations should coordinate messaging and mutual support for legal reform efforts.
Long-term vision (5+ years)
4.4.3
Regional integration of HIV responses should achieve seamless service provision for mobile populations, shared procurement, and supply chain management, and coordinated epidemic surveillance. These efficiencies can reduce costs while improving outcomes for the most vulnerable populations.
South–South technical cooperation should position the region as a global leader in rights-based HIV responses, sharing innovations with other regions facing similar legal and cultural contexts. Regional expertise in community mobilization, legal reform, and service integration offers valuable lessons for sub-Saharan Africa, Eastern Europe, and the Middle East.
Discussion
5
This comparative review affirms that legal environments and structural determinants are central to HIV epidemic control in South Asia. Countries enacting rights-based legal reforms demonstrate measurably better outcomes, while those retaining punitive statutes face persistent service gaps and rising incidence among key populations (173). The findings highlight four critical themes: (1) legal determinants as health drivers, (2) the implementation gap, (3) structural stigma in health systems, and (4) community participation as a catalyst for progress.
Legal determinants as health drivers
5.1
The analysis corroborates international evidence that decriminalization of same-sex conduct, sex work, and drug use is associated with significant improvements in HIV service uptake and outcomes (111–113). India’s 2018 repeal of Section 377 led to an 11% increase in testing among MSM within 2 years, reflecting enhanced community trust and reduced fear of arrest (14, 114). Nepal’s constitutional protections and judicial recognition of third gender status correspond with near-universal ART coverage among transgender individuals in urban centers (15, 115). Conversely, Pakistan’s mixed legal landscape—progressive transgender law amidst criminalization of other key populations—yields uneven outcomes: high uptake among transgender persons in pilot sites but low overall cascade performance (10, 116). Sri Lanka’s continued criminalization of LGBTI and sex work populations correlates with service avoidance and unreported transmission clusters despite robust general population services (18, 63).
The implementation gap
5.2
A consistent theme is the gap between legal reform and practical enforcement. Laws without implementation mechanisms risk creating illusory protections that undermine community confidence. In India, the HIV/AIDS Act (2017) legally prohibits discrimination but lacks designated enforcement bodies and suffers from low awareness among healthcare workers, limiting its impact (8, 54). Pakistan’s Transgender Persons Act mandates anti-discrimination safeguards yet faces regulatory vacuums and budgetary shortfalls for the National Commission for Transgender Persons, curtailing its operational capacity (50, 51). Nepal’s stalled Gender and Sexual Minorities Rights Act exemplifies how progressive constitutional language can stagnate without legislative follow-through (55). Addressing this gap requires not only law reform but also strengthened institutions, capacity building for rights commissions, and dedicated funding for enforcement and monitoring (117, 118).
Structural stigma in health systems
5.3
Stigma within healthcare remains a potent barrier despite legal protections. Studies in India and Sri Lanka document high levels of provider prejudice toward sex workers, PWID, and transgender individuals, leading to delayed presentation and poor retention (13, 119, 120). Training programs reduce discriminatory attitudes by up to 60% when combined with institutional accountability measures, yet most countries lack mandatory, standardized non-discrimination curricula for health cadres (84, 121). Structural stigma also manifests in service location and design—centralized hospital-based ART services in Sri Lanka and Pakistan exclude rural and mobile populations, while harm reduction programs in India are subject to police raids, deterring PWID from accessing needle-syringe exchange and OST (59, 62, 122, 123). Health system transformation must prioritize culture change through leadership engagement, inclusive policies, and routine monitoring of stigma indicators alongside clinical outcomes (124, 125).
Community participation as a catalyst
5.4
Civil society organizations (CSOs) have been the linchpin of effective HIV responses, especially in reaching marginalized groups. Peer-led outreach by the Durbar Mahila Samanwaya Committee in India and Blue Diamond Society in Nepal has achieved high testing and retention rates among female sex workers and transgender persons, respectively (15, 61, 126). However, CSOs often operate under restrictive legal frameworks and with inadequate funding; Pakistan allocates only 5% of its HIV budget to community services, undermining scale-up potential (16, 66). Evidence indicates that every 10% increase in community-led service funding correlates with a 5% improvement in cascade outcomes among key populations (127). Institutionalizing community participation requires formal governance mechanisms—reserved seats on national AIDS boards, budgetary earmarks, and co-creation of program strategies—to ensure that affected populations shape the services designed for them (69, 107).
Comparative and global implications
5.5
South Asia’s experience underscores that legal change is necessary but not sufficient; it must be accompanied by robust implementation, stigma reduction, service redesign, and community empowerment to realize full public health benefits. The causal pathway from rights-based governance to epidemic control is evidenced by regional correlations between RBA score (aggregated dimension ratings) and 95-95-95 achievements: higher RBA scores align with stronger cascade performance (128, 129). This framework offers a model for other regions, such as Eastern Europe and Central Asia, where punitive laws and service gaps mirror South Asian challenges (130, 131).
Policy recommendations revisited
5.6
The four strategic pillars—legal reform, health system transformation, funding equity, and regional collaboration—offer synergistic opportunities. Modeling from decriminalization in Portugal and harm reduction in Ukraine suggests that integrating these pillars can reduce HIV incidence by 30%–45% over a decade (132, 133). Policymakers should prioritize intersecting interventions, such as combining decriminalization pilots with community-led service expansion and anti-stigma training, to maximize impact and generate politically salient successes early in the reform process (134).
Strengths and limitations
5.7
This study’s strength lies in its comprehensive, comparative approach, integrating legal analysis, policy review, program data, and community perspectives across four diverse national contexts. Employing a structured RBA framework ensures consistency and facilitates actionable insights. Limitations include reliance on secondary sources, variable data quality across countries, and limited disaggregation of outcome data for key populations. Future research should incorporate primary qualitative studies with affected individuals and service providers to deepen understanding of implementation barriers and facilitators (135, 136).
Balancing legal mandates and public health ethics
5.8
While legal reforms such as decriminalization, anti-discrimination statutes, and constitutional protections are critical milestones in advancing the rights of people living with HIV (PLHIV), they cannot by themselves guarantee meaningful change. Evidence from national and regional contexts demonstrates that statutory protections often coexist with coercive practices such as mandatory HIV testing, travel restrictions, and punitive disclosure requirements. These measures, although frequently justified in the name of protecting public health, can in practice undermine autonomy, confidentiality, and equitable access to care, thereby reinforcing stigma rather than alleviating it (137, 138).
A rights-based approach therefore requires more than the enactment of laws; it demands the integration of public health ethics into policy design and implementation. Ethical principles of justice, non-maleficence, autonomy, and solidarity provide the normative foundation to ensure that legal reforms advance health equity. For example, laws that prohibit discrimination must be accompanied by provider training, community engagement, and mechanisms of accountability to prevent violations in healthcare settings. Similarly, protections for key populations must be enforced through supportive rather than punitive health systems that build trust with marginalized communities.
By aligning legal frameworks with ethical imperatives, governments can move beyond symbolic compliance toward reforms that tangibly reduce stigma, expand access, and improve health outcomes. This balance between the structural guarantees of law and the lived realities of ethical practice is central to achieving sustainable progress in HIV prevention and care.
Conclusion
6
This comparative rights-based policy review demonstrates that legal and structural reforms are fundamental to HIV epidemic control in South Asia. Countries that have implemented progressive decriminalization—such as India’s repeal of Section 377 and Nepal’s constitutional recognition of third gender status—show substantial improvements in HIV diagnosis, treatment uptake, and viral suppression among key populations. Conversely, Pakistan and Sri Lanka’s retention of punitive laws correlates with persistent service gaps and rising incidence among MSM, PWID, and transgender individuals (14, 15).
Achieving the UNAIDS 95-95-95 targets by 2025 and beyond requires sustained action across four strategic pillars: (1) legal reform and decriminalization to remove punitive barriers and enable harm reduction, (2) health system transformation to decentralize services, scale differentiated delivery, and institutionalize non-discrimination, (3) funding equity and community empowerment to ensure at least 30% of HIV resources reach community-led programs, and (4) regional collaboration to harmonize policies and share best practices across borders. Modelling from diverse jurisdictions suggests that integrated implementation of these pillars can reduce HIV incidence by up to 45% over a decade and accelerate progress toward universal viral suppression.
Structural stigma within healthcare settings remains a critical barrier; provider training and accountability measures must be prioritized to create truly inclusive services for all populations, irrespective of legal status or social identity. Legal protections without enforcement mechanisms offer limited benefit and may erode community trust if unaccompanied by institutional capacity-building for rights commissions and judicial bodies (8).
Civil society organizations are indispensable in reaching hidden and criminalized groups, yet operate under restrictive legal and funding constraints. Formalizing community participation within national HIV governance structures—through reserved seats, budget earmarks, and decision-making authority—will leverage their unique capacity for peer-led outreach and advocacy.
The implementation gap between law reform and practice underscores the need for continuous monitoring and evaluation of legal environment indicators alongside epidemiological outcomes. National human rights institutions and parliamentary committees should conduct regular reviews of discriminatory laws, service access inequities, and enforcement practices, ensuring real-world accountability for legal reforms.
In conclusion, sustainable HIV epidemic control in South Asia demands a rights-based governance paradigm that integrates legal reform, service innovation, community leadership, and regional cooperation. By aligning policy with human rights principles and empirical evidence, South Asian nations can not only achieve the 95-95-95 goals but also advance social justice, equity, and health for all. Failure to act on these interconnected strategies risks perpetuating cycles of criminalization, stigma, and poor health outcomes—undermining both public health imperatives and fundamental human rights.
This comparative analysis demonstrates that rights-based reforms are essential for moving from a punitive, criminalization-centered model of HIV governance toward one rooted in care, dignity, and equity. However, legal mandates alone cannot guarantee transformative change. As evidence from Iran and across Asia and the Middle East illustrates, statutory protections often remain under-implemented or coexist with coercive measures such as mandatory testing and travel restrictions, which undermine the very rights they claim to protect.
To be effective, rights-based reforms must be accompanied by an explicit commitment to public health ethics. Principles of justice, autonomy, non-maleficence, and solidarity provide the ethical grounding necessary to ensure that legal reforms reduce stigma, minimize discrimination, and promote equitable access to services. By aligning legal frameworks with ethical practice—through confidentiality protections, non-discriminatory service delivery, and community-based interventions—governments can ensure that reforms are not merely symbolic but deliver tangible improvements in the lives of people living with HIV.
Ultimately, achieving the transition from criminalization to care requires striking a balance between the structural guarantees provided by law and the lived realities shaped by ethical practice. Only when legal mandates and public health ethics converge can HIV responses advance health equity and human rights in meaningful and sustainable ways.
Limitations
7
As this work is based on a narrative review, certain methodological constraints should be acknowledged. The synthesis may be influenced by interpretive or confirmation bias, and findings are dependent on the availability and quality of publicly accessible documents. Although triangulation across multiple data sources was applied to enhance reliability, the absence of quantitative synthesis and formal inclusion–exclusion procedures limits reproducibility. Nevertheless, this approach provides valuable conceptual depth and theoretical insight into how legal and policy reforms intersect with public health ethics and human rights in the region.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1UNAIDS. Global AIDS Update 2024. Geneva: UNAIDS (2024).
- 2WHO. HIV/AIDS in the South-East Asia region: Progress and challenges. New Delhi: WHO SEARO (2023).
- 3UNAIDS. UNAIDS Data 2024. Geneva: UNAIDS (2024).
- 4Beyrer C Baral SD Griensven F Goodreau SM Chariyalertsak S Wirtz AL. Global epidemiology of HIV infection in men who have sex with men. Lancet. (2012) 380:367–77. doi: 10.1016/S 0140-6736(12)60821-622819660 PMC 3805037 · doi ↗ · pubmed ↗
- 5UNDP UNAIDS. HIV and the law: Risks, Rights & Health (2012): Global commission report. New York: UNDP (2012).
- 6UNAIDS. Criminalization and HIV: Policy brief and evidence summaries. Geneva: UNAIDS (2024).
- 7Shannon K Strathdee SA Goldenberg SM Duff P Mwangi P Rusakaniko S. Global epidemiology of HIV among female sex workers: influence of structural determinants. Lancet. (2015) 385:55–71. doi: 10.1016/S 0140-6736(14)60931-425059947 PMC 4297548 · doi ↗ · pubmed ↗
- 8Government of India. The HIV and AIDS (prevention and control) act. New Delhi: Ministry of Law & Justice (2017).