The effects of professional expertise on perceptions of treatment need in patients with class II division 1 malocclusion: a comparison between orthodontists, general dentists, and lay people in Germany
Sarah Bühling, Stefanie Neidhardt, Babak Sayahpour, Sara Eslami, Nicolas Plein, Stefan Kopp

TL;DR
This study shows that orthodontists, general dentists, and laypeople in Germany differ in how they perceive the need for orthodontic treatment in patients with certain dental misalignment.
Contribution
The study reveals how professional expertise influences perceptions of treatment need and facial harmony in class II division 1 malocclusion.
Findings
Orthodontists perceived treatment need at 4 mm overjet, while general dentists needed 6 mm.
Laypeople did not perceive treatment need at any overjet level.
Facial harmony perception correlated with treatment need perception across all groups.
Abstract
This study aimed to compare the perception of practitioners with varying levels of expertise and laypeople regarding the orthodontic treatment need and facial harmony in patients with increased anterior overjet. Three groups of observers (orthodontists, general dentists, and laypeople, in total n = 48) were asked to rate on images—using a 10-point visual analog scale (VAS)—the facial harmony and treatment need of a sample of 8 patients with class II division 1 malocclusion and overjets of 2, 4, 6, and 8 mm. Statistically significant differences were observed between the three groups of observers regarding patients with an overjet of 4 mm and above (p < 0.001). Treatment need was perceived at an overjet of 4 mm by orthodontists and 6 mm by general dentists, whereas laypeople did not perceive a need for treatment in any of the groups (p < 0.001). Regarding perception of facial harmony,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
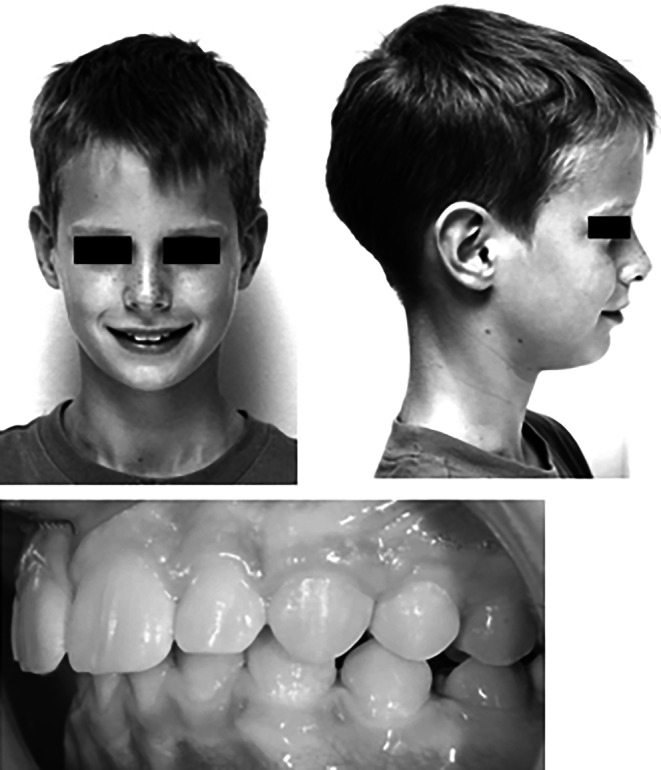 Figure 1
Figure 1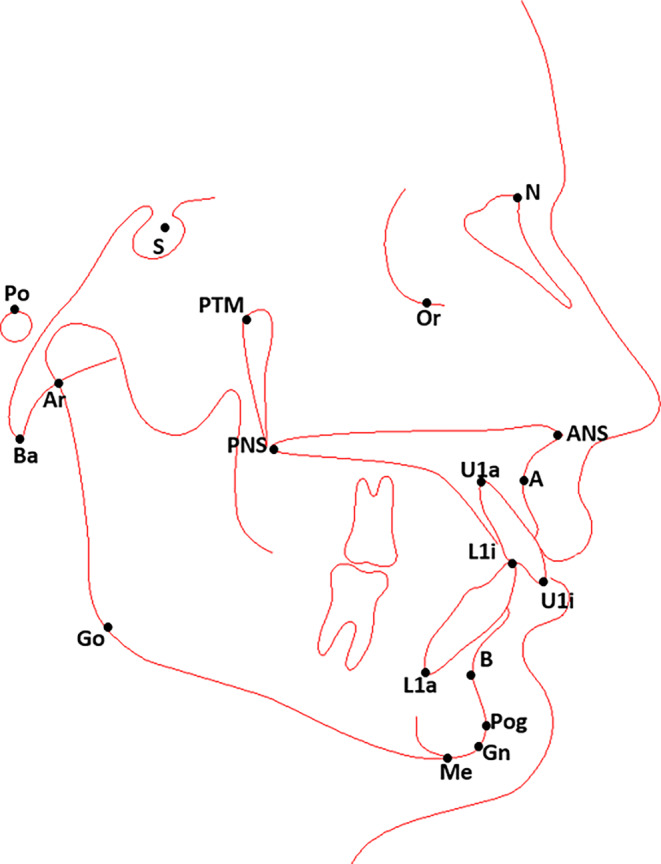 Figure 2
Figure 2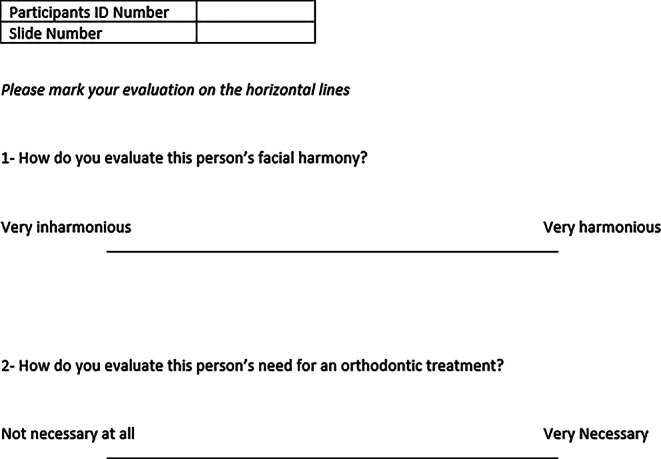 Figure 3
Figure 3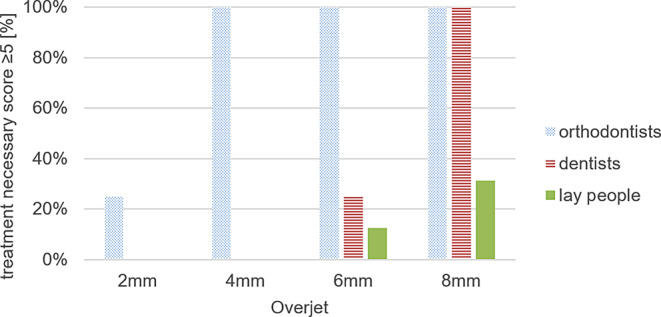 Figure 4
Figure 4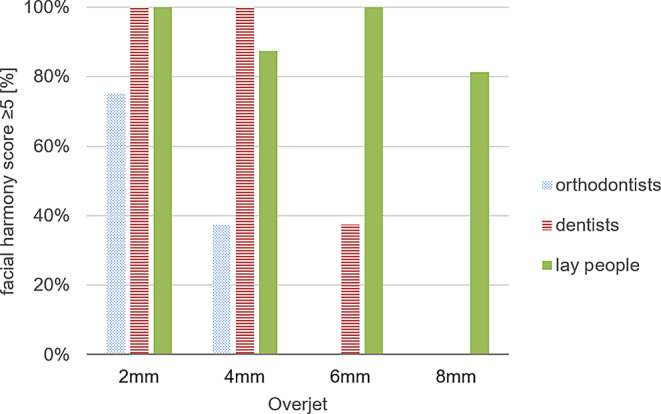 Figure 5
Figure 5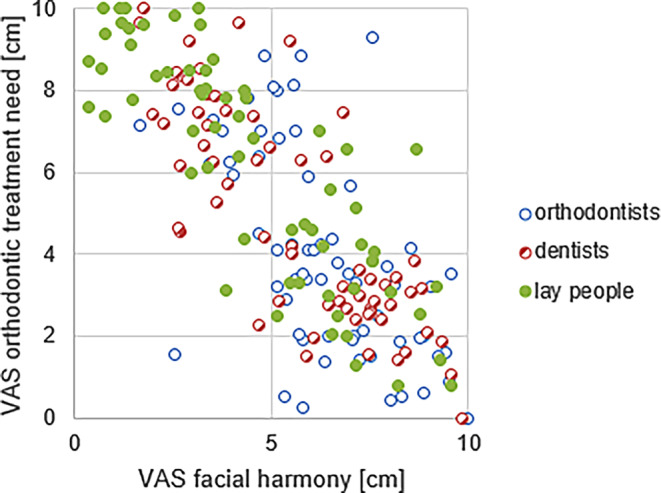 Figure 6
Figure 6- —Johann Wolfgang Goethe-Universität, Frankfurt am Main (1022)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthodontics and Dentofacial Orthopedics · Facial Rejuvenation and Surgery Techniques · Temporomandibular Joint Disorders
Introduction
Hallmark of class II division 1 malocclusions is the increased anterior overjet, which is accompanied with lip incompetency in more severe cases [1]. The patients are at risk of several health issues, including traumatic damage to the maxillary incisors, mouth breathing, which increases the risk of gingivitis and caries, and a higher likelihood of developing craniomandibular disorders [2–8]. Thus, reducing the increased anterior overjet in these malocclusions is a primary objective of orthodontic treatment.
Orthodontic indices with different cut-off values have been developed to assess the orthodontic treatment need of different malocclusions. While some indices focus solely on dental, occlusal, and functional factors, others also consider esthetic perception [9].
Since 2002, the German public health insurance system has utilized the Orthodontic Indication Group (KIG) system to determine the need for orthodontic treatment [9]. This system is focused exclusively on the dental malocclusion aspect and does not account for esthetic or functional considerations. Under this system, public insurance coverage for treatment costs in the class II malocclusion category is only provided for overjet values greater than 6 mm.
Despite the KIG system’s sole emphasis on dental malocclusion aspects, previous studies have demonstrated that orthodontists and general dentists consider both functional and esthetic factors when determining orthodontic treatment need [10–12]. On the other hand, laypeople tend to prioritize the esthetic aspect of malocclusions [11, 13–17].
Generally, facial symmetry as well as white and straight teeth are considered esthetically pleasing from the laypeople perspective [13, 18]. However, improvement of oral function does not necessarily contribute to the patient’s satisfaction [14, 17]. Orthodontic treatment need is not deemed necessary by laypeople as long as there is no crowding or spacing of teeth or only a large overjet and as long as there are no symptoms of temporomandibular disorder (TMD) [16, 17]. Thus, understanding of patients’ perception of facial harmony and orthodontic treatment need is crucial to ensure their satisfaction.
Understanding the perception of general dentists is also crucial, as they are important referral sources for orthodontists in the German healthcare system. They often identify the need for orthodontic treatment and refer patients to orthodontic offices during routine check-ups [16, 17].
Achieving a consensus among patients, general dentists, orthodontists, and healthcare providers regarding the need for orthodontic treatment would ensure a high level of healthcare quality and patient satisfaction [13, 14]. Conversely, disagreements on this topic may compromise the quality of care and result in patient dissatisfaction.
Therefore, the present study aimed to determine the differences in the perception of orthodontic treatment need and facial harmony of patients with different severities of increased anterior overjet from the perspective of orthodontists, general dentists and laypeople. Secondary aim was to determine whether there is a correlation between perceived facial harmony and the perceived treatment need.
Materials and methods
Study design and ethic approval
Ethic approval for this monocentric cross-sectional survey study was granted by the Institutional Review Board of Goethe University of Frankfurt am Main (no. 2024-1990). Informed consents were obtained from the patients or their legal guardians regarding publishing their data and photographs.
Study groups, sample size calculation
Three groups were included in this study: orthodontists, general dentists, and laypeople. Sample size was calculated with the probability of error set at α = 5% and a power of 80%. For the determination of the effect size, it was assumed that the Mann–Whitney estimator for the comparison of the score values of laypeople to general dentists was approximately 0.7.
In addition, for the Mann–Whitney estimator, a value of 0.8 was assumed for the comparison of laypeople to orthodontists and a value of 0.65 for the comparison of the general dentists and the orthodontists.
Therefore, a sample size of 48 (16 participants per group) was calculated.
Participant recruitment
In all, 48 adult participants (16 orthodontists, 16 general dentists, and 16 laypeople with no experience in dentistry) with Caucasian ethnicity living in Germany were recruited. Their demographic information is shown in Table 1.Table 1. Participants’ descriptive dataDeskriptive Daten der TeilnehmerOrthodontistsGeneral dentistsLaypeopleN%N%N%Age, years31 ≤ 4116.25956.25850.041 ≤ 51956.25531.25425.051 ≤ 61425.016.2516.2561 <212.516.25318.75GenderMale956.251062.5850.0Female743.75637.5850.0
Sample images and questionnaire preparation
Sample images (Fig. 1) consisted of the two extra-oral photographs (smiling frontal view and profile at rest) as well as one intra-oral image of the occlusion (left side). They were taken from 4 boys and 4 girls who fulfilled the following inclusion criteria:
- Patients undergoing orthodontic therapy in the orthodontic department,
- Below 18 years of age,
- Anterior overjet of 2, 4, 6, and 8 mm,
- Skeletal class II division 1 malocclusion (ANB > 6°, U1-NA > 22°; Fig. 2),
- Lack of any visible crowding, irregularity or spacing,
- Lack of midline deviations of 0.5 mm or higher,
- Fully permanent dentition,
- Caucasian ethnicity, and
- Available and complete pretreatment diagnostic records including lateral cephalograms. Fig. 1. Sample image of a patient with increased overjetBeispielbild eines Patienten mit vergrößerter sagittaler FrontzahnstufeFig. 2Tracing of the lateral cephalogram. Following landmarks were used for the analysis: S sella turcica, N nasion, Ba basion, Or orbitale, P porion, ANS anterior nasal spine, PTM pterygomaxillary fissure, A A point, B B point, U1a upper incisor apex, U1i upper incisor edge, L1a lower incisor apex, L1i lower incisor edge, Me menton, Gn gnathion, Ar articulare, Go gonionDurchzeichnung des Fernröntgenseitenbildes. Folgende Referenzpunkte wurden für die Analyse verwendet: S Sella turcica, N Nasion, Ba Basion, Or Orbitale, P Porion, Spa Spina nasalis anterior, Pm Pterygomaxillare, A A-Punkt, B B-Punkt, Isa Incision superius apicale, Is Incision superius, Iia Incision inferius apicale, Ii Incision inferius, Me Menton, Gn Gnathion, Ar Articulare, Go Gonion
Patients with syndromes manifesting on the face, visible facial scars, missing anterior teeth, discolorations, braces, and large fillings or crowns on the anterior teeth and other malocclusions such as crossbite or anterior openbite were excluded.
The images were converted to black and white, printed on photographic paper and assembled into a slide containing a visual analog scale (VAS)-based questionnaire (Fig. 3), containing two questions:
- How do you rate this person’s facial harmony? (Left: very inharmonious, right: completely harmonious)
- How do you rate this person’s need for an orthodontic treatment? (Left: not necessary at all, right: very necessary) Fig. 3. QuestionnaireFragebogen
Observers’ rating of sample images
Participants were informed that they would be presented with several images and instructed to rate them on the VAS scale based on their perception of facial harmony and treatment necessity of each model using a pen with a fine 0.7 mm tip width (Fig. 3). The pictures were presented in a random manner to the participants and they received 1 min for evaluation of each patient.
Before conducting the study, four experienced orthodontists independently scored the images. One month later, the same orthodontists re-evaluated the images, and they reached a unanimous agreement that aligned with their initial assessments. This demonstrated a high level of consistency in image scoring, rendering reliability testing unnecessary.
VAS score analysis
All questionnaires were analyzed by one examiner. Answers on the 100 mm VAS score were analyzed using a standard metric ruler with a precision of 0.5 mm. The score was rounded to the next whole millimeter. A score ≥ 5 meant that the participant considered that orthodontic treatment for this patient was necessary or that the face was seen as harmonious [19].
Statistical analysis
BiAs software version 11.06 (BiAS for Windows; Epsilon Verlag GmbH, Frankfurt, Germany) was used for the statistical analysis of this study. The statistical analysis was done by the Institute for Biostatistics and Mathematical Modeling at Johann Wolfgang Goethe University in Frankfurt am Main. The nonparametric Kruskal–Wallis test was used to examine the differences between the groups. The Χ^2^ consistency table test was used to show possible relationships of the categorical data. If the test was weak, the Craddock–Flood Χ^2^ test was used. Spearman’s rank correlation was used to quantify the association between two subjects (orthodontic treatment need, facial harmony). The confidence level was set at α = 5% and the power at 80%.
Results
Perception of orthodontic treatment need
Tables 2 and 3 as well as Fig. 4 display the mean values of perceived treatment need VAS score ratings by participants for each patient.Table 2. Perception of orthodontic treatment need in each group of patients by participants. Visual analog scale (VAS) scores are shown by their mean value, standard deviation (SD), minimum (Min), maximum (Max)Wahrnehmung des kieferorthopädischen Behandlungsbedarfs bei den einzelnen Patientengruppen durch die Teilnehmer. Gezeigt werden VAS(visuelle Analogskala)-Bewertungen mit Mittelwert, Standardabweichung (SD), dem niedrigsten (Min) und dem höchsten Wert (Max)Patient’s overjetGroupMeanSDMinMaxp value^a^2 mmOrthodontists3.852.490.59.30.122General dentists2.211.710.04.3Laypeople2.421.370.64.14 mmOrthodontists7.361.245.98.9< 0.001General dentists2.351.360.03.4Laypeople2.781.371.44.86 mmOrthodontists7.871.316.210.0< 0.001General dentists6.542.264.09.6Laypeople3.222.051.35.68 mmOrthodontists8.601.227.010.0< 0.001General dentists8.211.686.010.0Laypeople4.402.510.87.8^a^ p value of Kruskal–Wallis test. Statistical significance is at p ≤ 0.001Table 3Frequencies of the dichotomized visual analog scale (VAS) score regarding the perception of treatment need. Score summarizes the number of ratings greater and equal to or less than 5Häufigkeiten der dichotomisierten VAS(visuelle Analogskala)-Bewertung bezüglich des wahrgenommenen Behandlungsbedarfs. Der Score fasst die Anzahl der Bewertungen zusammen, die höher oder gleich bzw. niedriger als 5 sindPatient’s overjetVAS scoreOrthodontistsGeneral dentistsLaypeoplep value^c^N%N%N%2 mm≥ 5425.00000< 0.01^a^< 51275.016100161004 mm≥ 51610000000.00^b^< 50016100161006 mm≥ 5161001275.0212.50.00^b^< 500425.01487.58 mm≥ 51610016100531.25< 0.01^a^< 500001168.75^a^ p-value of Craddok–Flood test^b^ Χ^2^-contingency table test^c^ Statistical significance is p ≤ 0.001Fig. 4Perceived treatment need depending on stage of overjet. Percentage of all ratings with a score ≥ 5 are shown for each group (orthodontists, dentists, laypeople)Wahrgenommener Behandlungsbedarf in Abhängigkeit vom Stadium des Overjet. Der Prozentsatz aller Bewertungen mit einem Wert ≥ 5 wird für jede Gruppe (Kieferorthopäden, Zahnärzte, Laien) dargestellt
No statistically significant differences were found in the ratings of patients with an overjet of 2 mm (p = 0.122). None of the participants recognized a need for orthodontic treatment in patients with an anterior overjet of 2 mm, although the orthodontist group showed notable discrepancies in their assessments of the 2 mm overjet.
However, statistically significant differences were recorded at overjets of 4, 6, and 8 mm between the groups (p < 0.001).
The first treatment need was identified by orthodontists at the overjet of 4 mm with a mean VAS score of 7.36, while neither dentists nor laypeople recognized the need for treatment at this overjet.
The treatment need of patients with an overjet of 6 mm was recognized by both general dentists (mean value 6.54) and orthodontists (mean value 7.87).
Interestingly, orthodontists’ perceived treatment need did not increase with the severity of malocclusion. In contrast to general dentists and orthodontists, 87.5% of laypeople did not perceive any treatment need at the overjet of 6 mm, and the highest VAS score in this regard was only 5.6.
The orthodontists and general dentists were in agreement that an overjet of 8 mm required treatment, as indicated by their mean VAS scores of 8.60 and 8.21, respectively. However, there was considerable variability among laypeople’s ratings of patients with an overjet of 8 mm, ranging from a minimum VAS score of 0.8 to a maximum of 7.8. Despite this variability, the mean VAS score for laypeople in this group was 4.40, indicating that they did not perceive a treatment need.
Perception of facial harmony
Table 4 and Fig. 5 illustrate observers’ ratings regarding the patients’ facial harmony. Starting with an overjet of 4 mm, significant differences were recorded between the groups regarding the perceived facial harmony (p ≤ 0.001).Table 4. Perception of facial harmony in each group of patients by participants. Visual analog scale (VAS) score are shown by their mean value, standard deviation (SD), lowest value (Min), highest value (Max)Wahrnehmung der Gesichtsästhetik bei den einzelnen Patientengruppen durch die Teilnehmer. Gezeigt werden die VAS(visuelle Analogskala)-Bewertungen mit ihrem Mittelwert, der Standardabweichung (SD), dem niedrigsten (Min) und dem höchsten Wert (Max)Patient’s overjetGroupMeanSDMinMaxp value^a^2 mmOrthodontists5.752.012.58.10.006General dentists7.421.925.810.0Laypeople7.542.165.110.04 mmOrthodontists4.482.311.65.9< 0.001General dentists7.711.495.29.8Laypeople7.271.774.79.36 mmOrthodontists3.011.261.64.9< 0.001General dentists4.351.892.66.8Laypeople7.001.813.69.48 mmOrthodontists1.921.190.33.5< 0.001General dentists2.821.490.24.3Laypeople6.532.254.39.6^a^ p value of Kruskal–Wallis test. Statistical significance is at p ≤ 0.001Fig. 5Perceived facial harmony depending on stage of overjet. Percentage of all ratings with a score ≥ 5 are shown for each group (orthodontists, dentists, laypeople)Wahrgenommene Gesichtsästhetik in Abhängigkeit vom Stadium des Overjet. Der Prozentsatz aller Bewertungen mit einem Wert ≥ 5 wird für jede Gruppe (Kieferorthopäden, Zahnärzte, Laien) dargestellt
Faces showing an overjet of 2 mm were mostly considered harmonious by the group of orthodontists (mean value 5.75) but some of them considered the face as inharmonious (minimum 2.5, maximum 8.1). Patients with an overjet of 4 mm or higher were regarded as inharmonious by the majority of orthodontists (4 mm overjet, mean value 4.48; 6 mm overjet, mean value 3.01; 8 mm overjet, mean value 1.92).
General dentists regarded faces with an overjet of 2 mm (mean value 7.42) and 4 mm (mean value 7.71) as harmonious. From an increase in the overjet to 6 mm, the faces were considered to be inharmonious (6 mm overjet, mean value 4.35; overjet of 8 mm, mean value 2.82).
Laypeople perceived all of the faces as harmonious regardless of the overjet (2 mm, mean value 7.54; 4 mm, mean value 7.27; 6 mm, mean value 7.0; 8 mm, mean value 6.53). However, a minimal drop in evaluations towards disharmony could be found with the increase of overjet (Table 5).Table 5. Frequencies of the dichotomized visual analog scale (VAS) rating regarding the facial harmony. Score summarizes the number of ratings higher or lower than 5Häufigkeiten der dichotomisierten VAS(visuelle Analogskala)-Bewertung bezüglich der Gesichtsästhetik. Der Score fasst die Anzahl der Bewertungen zusammen, die höher oder niedriger als 5 sindPatient’s overjetVAS scoreOrthodontistsGeneral dentistsLaypeoplep value^c^N%N%N%2 mm≥ 51275.01610016100< 0.05^a^< 5425.000004 mm≥ 5637.5161001487.5< 0.001^a^< 51062.500212.56 mm≥ 500637.5161000.00^b^< 5161001062.5008 mm≥ 500001381.25< 0.001^a^< 51610016100318.75^a^ p-value of Craddok–Flood test^b^ Χ^2^-contingency table test^c^ Statistical significance is p ≤ 0.001
Correlation of facial harmony and treatment need
To quantify the correlation between perceived orthodontic treatment need and considered harmony of the face, the Spearman’s rank correlation was used and a value of 0.662 was obtained with a p-value < 0.001. Consequently, the correlation was found to be statistically significant. With an increasing VAS for perceived treatment need, the VAS for harmony of the face decreased (Fig. 6). This correlation can be found in the ratings within all three groups.Fig. 6. Correlation between facial harmony and perceived orthodontic treatment need. All ratings for each group (orthodontists, dentists, laypeople) are shown. VAS visual analog scaleKorrelation zwischen Gesichtsästhetik und wahrgenommenem kieferorthopädischen Behandlungsbedarf. Alle Bewertungen für jede Gruppe (Kieferorthopäden, Zahnärzte, Laien) werden dargestellt. VAS visuelle Analogskala
Discussion
The results of the present study showed significant differences between orthodontists, general dentists, and laypeople regarding their perception of treatment need and facial harmony in patients with class II division 1 malocclusions.
Differences in perception of treatment need in groups with different professional experience have been shown in previous studies and our findings confirm these results [20–24]. However, we have added the perception of facial harmony to our methodology, as the ideal image of facial and dental features may differ significantly between dental professionals and laypeople [20, 25]. Laypeople may recognize an increased overjet but still perceive the face as esthetically pleasing. There is still no accurate definition of a “beautiful face” as all people seem to have different points of view [10, 20, 26]. Nevertheless, a strong correlation was observed between the perception of facial harmony and treatment need by all participants. The increase in VAS rating for the perceived treatment need correlated with the decrease in VAS rating for facial harmony (Spearman’s rank correlation yielded a p-value < 0.001). These results are consistent with former studies that attempted to define standards for beautiful facial features [10, 20, 26].
Similar to other studies, orthodontists in our study displayed a more critical evaluation of the patient’s facial harmony and treatment need compared to general dentists and laypeople, as they identified a treatment need at an overjet of 4 mm [22, 27, 28]. It is noteworthy that this threshold is lower than the German public health insurance (KIG system) guideline, which considers a treatment indication at an overjet above 6 mm [29].
Previous studies have shown that orthodontists tend to have a more critical perception of orthodontic treatment needs, which can be attributed to their higher expertise and knowledge in the field of orthodontics [3, 6, 7]. Orthodontic specialists possess a more comprehensive understanding of the detrimental effects of an increased overjet and its accompanying lip incompetency on dental and oral health, such as risk of trauma and development of temporomandibular disorders [2, 4, 5]. Kuroda et al. [12] suggest that the recognition of need for orthodontic treatment of an enlarged overjet increases with increasing experience in the field of orthodontics.
Our results showed that laypeople did not perceive a need for orthodontic treatment or lack of facial harmony in patients with increased overjet, even though they registered the worsening of the overjet. It is important to note that the patients showed straight teeth and lacked visible irregularities or spacings. Angle class II malocclusion has previously been determined as esthetically pleasing in laypeople’s eyes [30]. This was also confirmed in the present study and underlines the laypeople’s focus on esthetic aspects of the malocclusion as opposed to the functional aspects [16, 31]. Previous studies have defined when there is a general need for orthodontic treatment by comparing various malocclusions of the teeth [24, 32]. However, the bases for the decisions of the individual respondents were not specified in these studies. Thus, it was never made clear as to the basis of which malocclusions of the teeth the decision for a necessary treatment was made [33, 34]. In the study by Prahl-Andresen et al. [35], profile drawings and color photographs of dentures were evaluated by orthodontists, general dental practitioners, and parents. The parents found significantly more of the photographs to be acceptable, whereas the opinions of the orthodontists and general dental practitioners differed only for certain malocclusions of the teeth; both groups rated more photographs as unacceptable than the parents’ group. Dentists often assess the need for treatment here as necessary only when the malocclusion feature is more pronounced and so are slightly less sensitive compared to orthodontists [35, 36]. Kokich et al. [36] compared the opinions of orthodontists, general dental practitioners, and laypeople on the minimal changes acceptable in the shape, size, and position of the anterior teeth and surrounding soft tissue; they concluded that the orthodontists were very sensitive to changes from the ideal, while the laypeople did not always detect them, even in the presence of major changes. These observations also confirm the results of this study.
Furthermore, patients do not seem to be aware of the complex interrelationships of an enlarged overjet and symptoms linked to craniomandibular disorders (CMD) [21, 37].
Therefore, it is vital to create awareness about the topic from the patient’s point of view. General dentists have an essential role in this regard, being the primary contact and referral source for orthodontic treatment in the German healthcare system.
Compared to the orthodontists, general dentists showed a higher threshold for treatment need and identification of lack of facial harmony. They considered patients with an overjet of 6 mm or larger to be in need of treatment, which is in line with the guidelines of the KIG system. This could be explained through the dental curriculum in Germany. Classification of orthodontic treatment need based on KIG system is integrated in the dental curriculum of undergraduate orthodontic program in Germany and, thus, shapes the dental students’ perception of malocclusions’ severity. This could potentially lead to a diagnostic bias in general dentists, which would compromise their ability in detection and referral of patients with malocclusions below KIG threshold values. However, further studies are required to provide clarity on this assumption of bias in orthodontic diagnosis of general dentists in Germany.
Laypeople are not familiar with the functional aspects that orthodontists consider in deciding treatment needs. The lack of awareness in laypeople combined with general dentists’ failure to identify orthodontic treatment needs in certain patients can pose a risk of undiagnosed conditions like upper incisors’ susceptibility to traumatic injury and higher risk of developing CMD symptoms [12, 38]. Even though the evidence regarding the etiological role of dental malocclusions in development of CMD remains controversial and a recent literature review reported the absence of an association for the majority of occlusal traits [39], the source of the controversy appears to lay in the lack of standardization and partly insufficient scientific rigor of heterogeneous methods of CMD diagnosis [40, 41]. Since CMD can severely affect the quality of life, creating awareness about occlusion’s importance at a young age is crucial [7, 37, 42].
Limitations
The authors acknowledge that different factors such as ethnicity, age, and personal preferences can influence one’s perception of facial attractiveness. To minimize these effects, we used faces of the same ethnic background and presented them in black and white. However, individual differences remain. Although the use of digitally manipulated photos of one single patient instead of images of different patients would have made the model photos more homogeneous, real patient pictures were used to avoid the artificial appearance associated with digitally manipulated images. This precaution was taken to mitigate any potential negative impact on observers’ perceptions caused by the presence of manipulated photos.
The use of a visual analog scale allowed for more accurate analysis of data but had the potential for variation in the interpretation of the scale. The study also recognizes the potential bias introduced by the Hawthorne effect and the exclusion of certain subjects.
Conclusion
This study showed that orthodontic treatment need and facial harmony are evaluated differently by orthodontists, general dentists, and laypeople. While orthodontists perceived a treatment need for patients with an overjet of 4 mm or larger, the general dentists perceived a treatment need at an overjet of 6 mm or more, which corresponds with German KIG system.
In absence of incisor crowding or irregularities, laypeople’s perception of treatment need or facial inharmony was not significantly affected by the increase in overjet.
The results of the present study underline the importance of patient education regarding the functional aspects of malocclusions with increased anterior overjet and suggest the possible presence of bias in diagnostic abilities of general dentists in Germany.