Endoscopic ultrasound-free lumen apposing metal stent recanalization of a complete ileal J-pouch stenosis restoring intestinal continuity
Pietro Graceffa, Alba Sparacino, Emanuele Bracciamà, Fabio Cartabellotta, Cosimo Callari, Antonino Granata

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
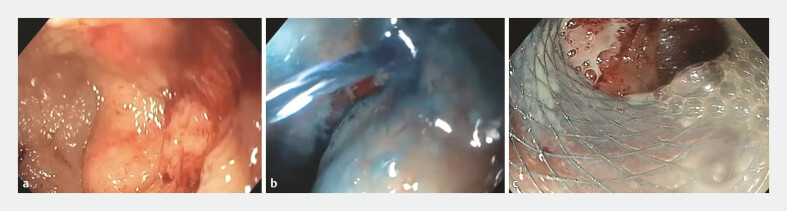 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Gallbladder and Bile Duct Disorders · Gastrointestinal Bleeding Diagnosis and Treatment
Benign strictures after ileal pouch–anal anastomosis occur at the pouch inlet, mid-pouch, or anastomosis and may impair pouch function and quality of life. Endoscopic therapies – including balloon dilation and stricturotomy – are effective and organ-sparing, but recurrence and technically inaccessible strictures remain challenging 1 2 . Self-expanding metal stents have been explored in benign large-bowel obstruction with encouraging efficacy and acceptable adverse events in selected patients 3 . For “complete” anastomotic occlusions, combined antegrade–retrograde “rendezvous” techniques have been described; more recently, lumen-apposing metal stents (LAMSs) have enabled endoscopic re-anastomosis, typically with EUS guidance 4 5 .
We present an EUS-free recanalization of a complete J-pouch afferent-limb stenosis ( Video 1 ).
EUS-free, wire- and fluoroscopy-guided deployment of a 16 × 20-mm LAMS across a complete J-pouch afferent-limb stenosis, restoring pouch continuity.Video 1
A 45-year-old man with a history of ulcerative colitis underwent total colectomy with ileal J-pouch construction 13 years prior, complicated by an anastomotic fistula requiring ileostomy. The patient subsequently developed chronic pouchitis for which vedolizumab therapy was initiated.
A follow-up endoscopy demonstrated a complete stenosis of J-pouch with an afferent limb in the absence of an endoscopically visible communication ( Fig. 1 a ). An endoscopic exploration of the efferent limb through the stoma was therefore performed in an unsuccessful attempt to visualize the communication with the pouch. A diagnostic maneuver was conducted by injecting saline and methylene blue into the efferent limb through the stoma, resulting in dye visualization within the pouch, confirming the presence of a fistulous tract ( Fig. 1 b ). A guidewire was introduced from the pouch into the afferent limb under endoscopic guidance. In order to restore intestinal continuity, we first performed an endoscopic dilation of the fistulous tract of up to 15 mm and then a LAMS 16 × 20 mm (Niti-S HOT SPAXUS Stent) was safely deployed over a guidewire across the stenosis under fluoroscopic guidance. The exploration of the afferent limb through the LAMS confirmed the successful endoscopic reanastomosis ( Fig. 1 c ). The procedure was well tolerated and the patient subsequently successfully underwent complete recanalization with the removal of ileostomy.
a An endoscopic view of complete pouch occlusion. b Fistulous tract identification. c Post-deployment traversal confirming restored patency.
The procedure was performed using a colonoscope with a 3.7 mm working channel. The SPAXUS stent is preloaded on an electrocautery-enhanced delivery system, featuring an electrocautery tip designed to penetrate the target organ tissue. The system has a 10 Fr delivery profile and a working length of 180 cm and is compatible with therapeutic endoscopes with a working channel diameter of 3.7 mm or larger.
This EUS-free, wire- and fluoroscopy-guided LAMS approach may offer a minimally invasive option to re-establish pouch continuity in select complex postoperative scenarios where conventional dilation or rendezvous is impractical. Careful selection and fluoroscopic control are essential.
Endoscopy_UCTN_Code_TTT_1AQ_2AF
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bharadwaj S Shen B Medical, endoscopic, and surgical management of ileal pouch strictures (with video)Gastrointest Endosc 201786597310.1016/j.gie.2017.01.04328189635 · doi ↗ · pubmed ↗
- 2Segal JP Adegbola SO Worley GHTA systematic review: the management and outcomes of ileal pouch strictures J Crohns Colitis 20181236937510.1093/ecco-jcc/jjx 15129155985 · doi ↗ · pubmed ↗
- 3Fardanesh A George J Hughes D The use of self-expanding metallic stents in the management of benign colonic obstruction: a systematic review and meta-analysis Tech Coloproctol 2024288510.1007/s 10151-024-02959-739028327 PMC 11271435 · doi ↗ · pubmed ↗
- 4Ngamruengphong S Mohapatra S Runge TM Recanalization of a complete coloanal anastomotic obstruction using a combined antegrade-retrograde rendezvous technique Endoscopy 202052 E 312E 31410.1055/a-1104-511932106316 · doi ↗ · pubmed ↗
- 5Guzik P Aka A Skef W Novel use of lumen-apposing metal stent for recanalization of complete stenosis of colo-colonic anastomosis Endoscopy 20235501 E 470E 47110.1055/a-2013-182036828024 PMC 9957675 · doi ↗ · pubmed ↗