Marsupialisation of a tunnel flap for a false oesophageal lumen post peroral endoscopic myotomy
Hasib Ahmadzai, Clarence Kerrison, Jun Young Kim, Brian Lam, Yong Sul Kim, Sunil Gupta, Michael J. Bourke

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
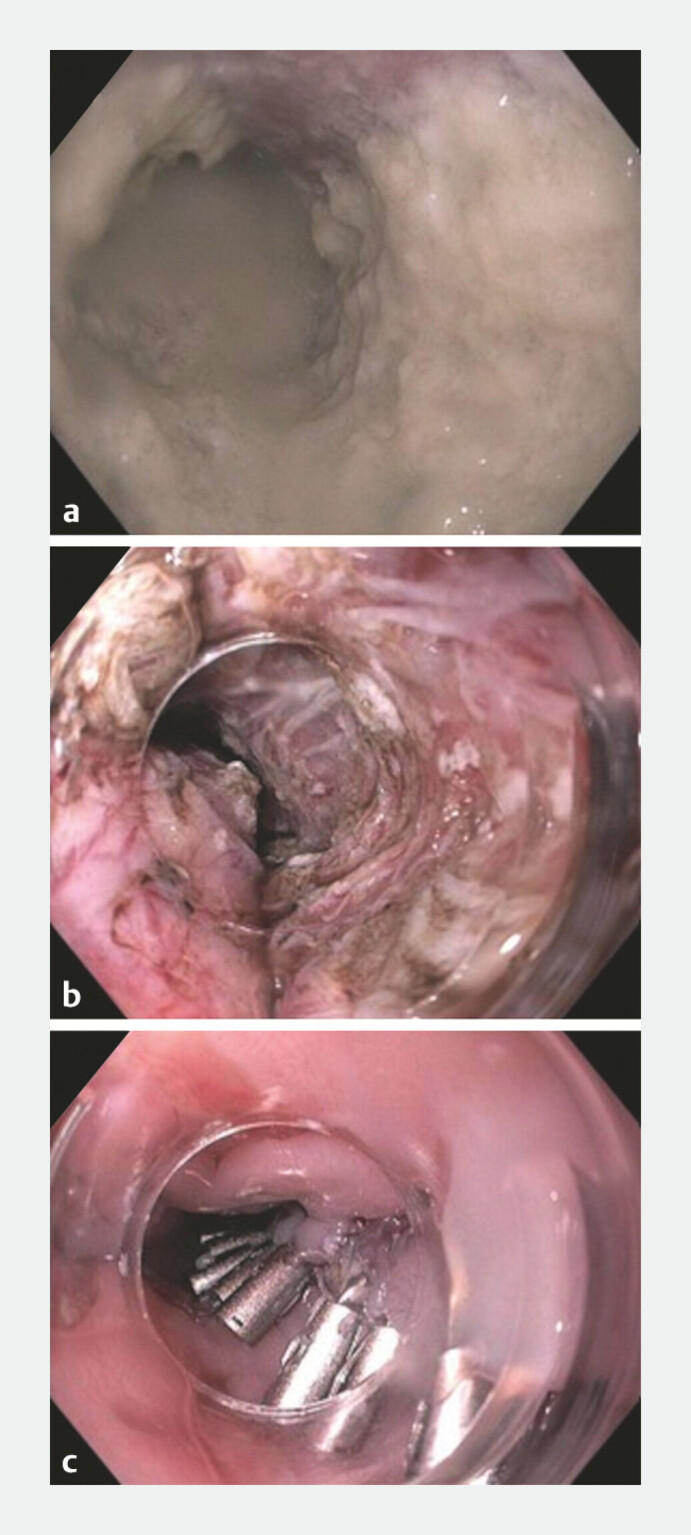 Fig. 1
Fig. 1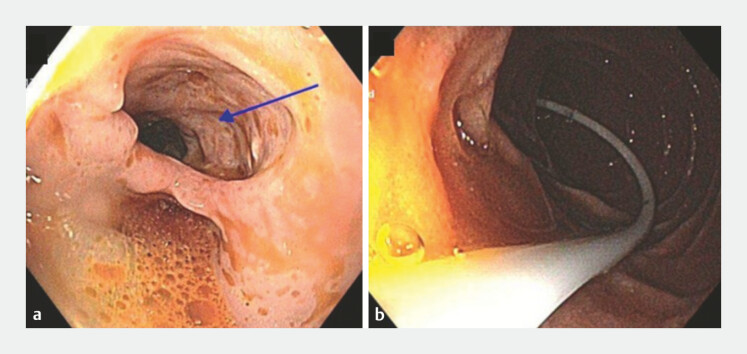 Fig. 2
Fig. 2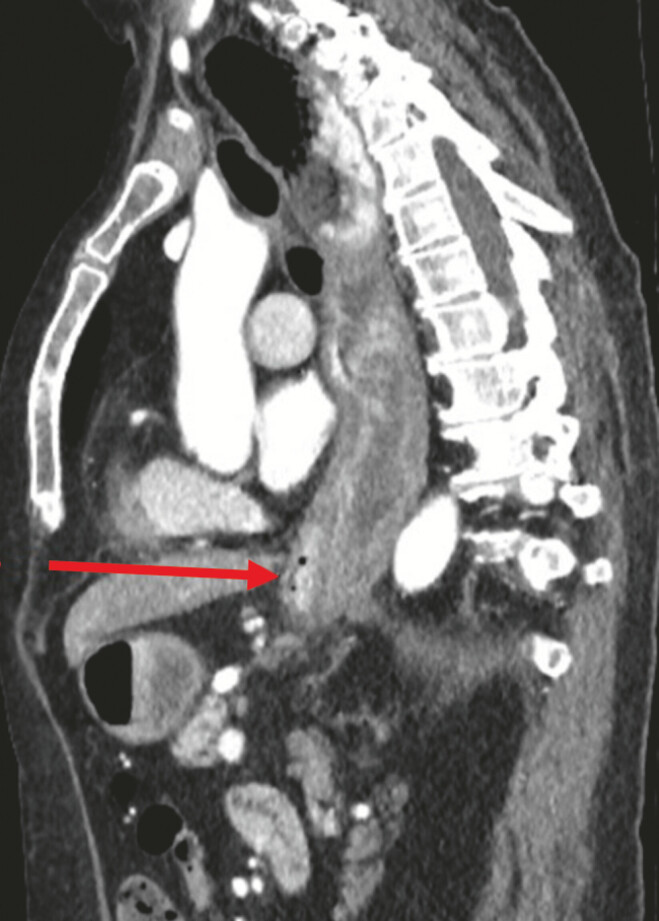 Fig. 3
Fig. 3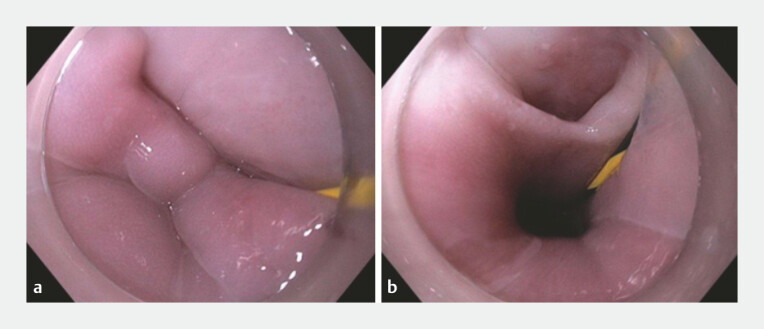 Fig. 4
Fig. 4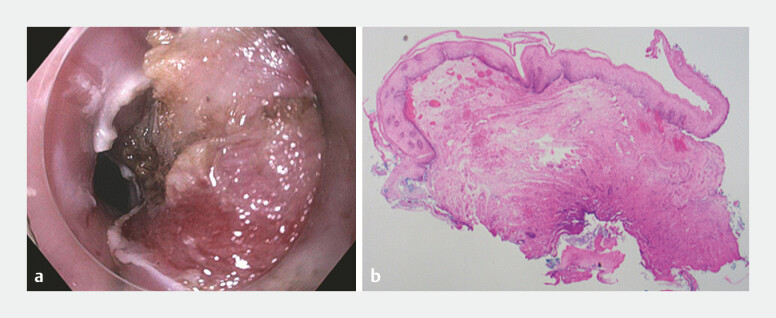 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Dysphagia Assessment and Management · Tracheal and airway disorders
A 68-year-old woman with type 2 achalasia, chronic oesophageal stasis, a thickened mucosal layer, and an Eckardt score of 8 underwent an uncomplicated peroral endoscopic myotomy (POEM; Fig. 1 ). One-month post-POEM, she developed recurrent dysphagia, regurgitation and aspiration. Repeat gastroscopy revealed dehiscence of the oesophageal mucosotomy (tunnel orifice) and formation of a long false lumen ( Video 1 ). This was consistent with the original submucosal tunnel, with its wall being a mucosal flap and a healed post-myotomy muscularis propria layer.
Achalasia changes with food contamination and aperistalsis in a . Peroral endoscopic myotomy performed in b , with clip closure following the POEM procedure in c . POEM, peroral endoscopic myotomy.
Mucosotomy dehiscence is found 1 month following a POEM procedure. Marsupialisation of the tunnel mucosal flap is performed with resolution of the patient’s symptoms. POEM, peroral endoscopic myotomy.Video 1
A nasojejunal feeding tube was endoscopically placed for feeding ( Fig. 2 ). A computed tomographic scan with oral contrast showed minimal passage of contrast into the distal third of the oesophagus and no mediastinal leak ( Fig. 3 ). Despite a conservative approach, repeat gastroscopy after a further 4 weeks demonstrated a persistent false lumen, a dilated proximal oesophagus containing food debris and oesophageal candidiasis ( Fig. 4 ).
Formation of a false lumen from the open POEM tract (blue arrow) in a and insertion of a nasojejunal feeding tube in b . POEM, peroral endoscopic myotomy.
A sagittal CT scan with oral contrast showing no mediastinal leak with a dilated oesophagus (red arrow). CT, computed tomography.
A false lumen with a Jagwire passing into the open POEM tract in a and insertion of the Jagwire through the POEM tract into the stomach in b . POEM, peroral endoscopic myotomy.
Three months post-POEM procedure, we proceeded with endoscopic marsupialisation of the false lumen. The tunnel was completely epithelialised. There was a small fistula back into the oesophagus at the level of the gastro-oesophageal junction (GOJ). A 0.035-inch Jagwire was placed into the false lumen, through the distal opening and into the stomach ( Fig. 5 ). An endoscopic knife was used to dissect the mucosal flap, using the wire as a guide down to the GOJ. Redundant mucosal tissue at the site of the incision was then resected with the EMR technique using a 10 mm hot snare. Repeat gastroscopy 7 months post-POEM showed a healthy appearing scar without evidence of a false lumen. The lower oesophageal sphincter opened easily ( Video 1 ). Reassuringly, the patient’s symptoms had resolved following this, with an Eckardt score of 0.
Marsupialisation of the tunnel flap in a and histology of the resection mucosal flap in b , showing dense fibrosis in submucosa with no definite muscularis propria seen.
Dehiscence of a submucosal tunnel mucosotomy site leading to a false lumen is a rare complication of POEM 1 2 3 . Symptom recurrence post-POEM warrants further endoscopic evaluation. Herein, we have demonstrated a novel technique of guidewire-assisted marsupialisation and eliminated the false lumen and the associated symptoms.
Endoscopy_UCTN_Code_TTT_1AQ_2AD_3AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sidhu M Tate D Bourke MJ 1147 Resolution of a Persistent Mucosal Defect After Peroral Endoscopic Myotomy (POEM) With Clip Closure Gastrointest Endosc 202285 AB 153
- 2Nabi Z Reddy N Ramchandani M Adverse events during and after per-oral endoscopic myotomy: prevention, diagnosis, and management Gastrointest Endosc 20188741728987545 10.1016/j.gie.2017.09.029 · doi ↗ · pubmed ↗
- 3Bhandari S Parekh D Bhandari S Endoscopic management of mucosal incision site dehiscence following peroral endoscopic myotomy Endosc Int Open 202210 E 1307 E 130810.1055/a-1889-422236118646 PMC 9473839 · doi ↗ · pubmed ↗