Four-branched hybrid stent placement using multi-hole-covered self-expandable metallic stents for Bismuth type IV malignant hilar biliary obstruction
Shinya Kawaguchi, Shinya Endo, Tatsunori Satoh

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
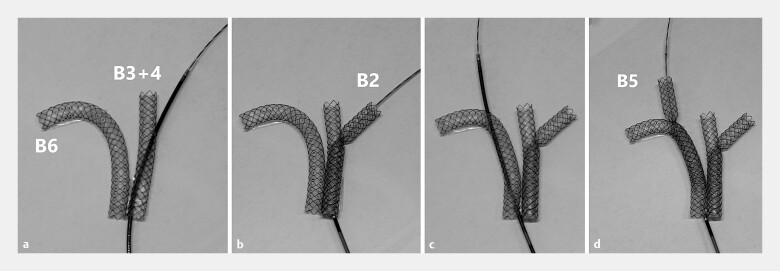 Fig. 1
Fig. 1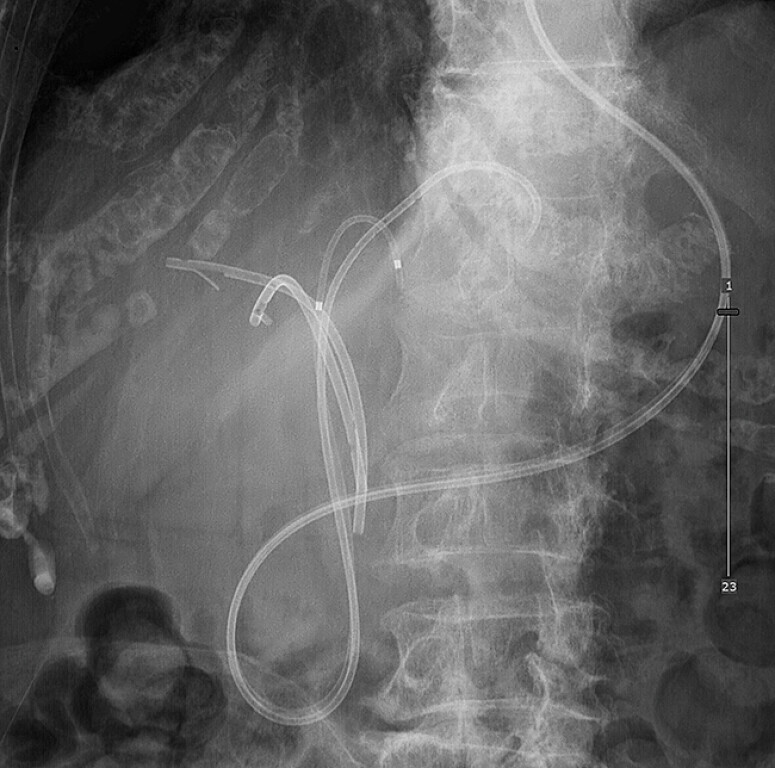 Fig. 2
Fig. 2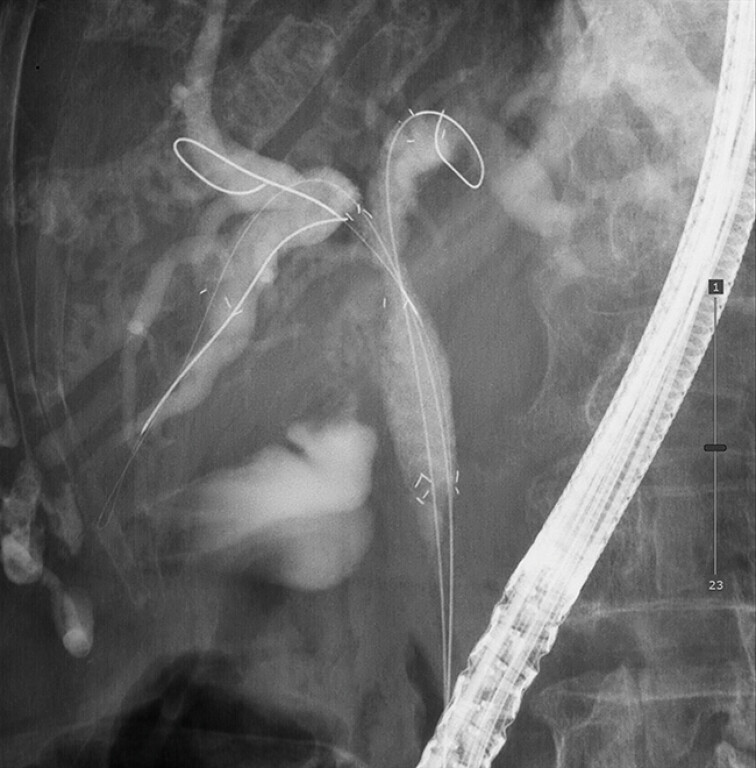 Fig. 3
Fig. 3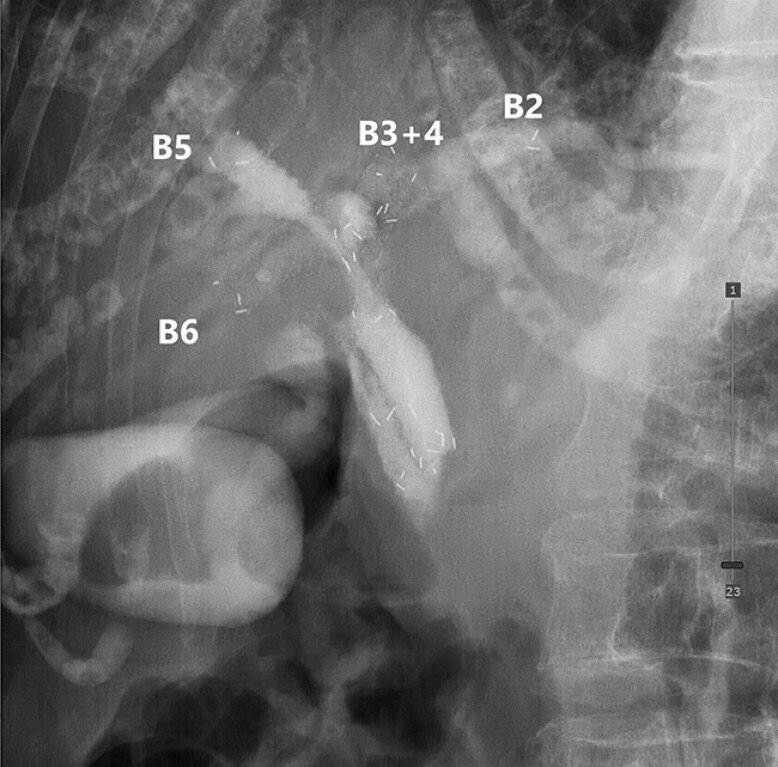 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Cholangiocarcinoma and Gallbladder Cancer Studies · Pediatric Hepatobiliary Diseases and Treatments
Hybrid stent placement during endoscopic retrograde cholangiopancreatography (ERCP), combining side-by-side (SBS) and stent-in-stent (SIS) techniques allows multi-segmental drainage of complex malignant hilar biliary obstruction (MHBO 1 2 ). Conventionally, uncovered self-expandable metallic stents (SEMSs) are used. A multi-hole-covered SEMS (MHSEMS; HANAROSTENT Biliary Multi-hole Benefit; M.I. Tech Co., Ltd, Pyeongtaek, South Korea) has recently been developed, designed with side holes to facilitate branch access, prevent side-branch occlusion, tumour ingrowth, and stent migration, while maintaining removability 3 4 5 . Here, we describe the first case of hybrid SBS and SIS placement using four MHSEMSs, achieving four-branched drainage in a bismuth type IV MHBO ( Fig. 1 ).
Bench-top photograph demonstration of hybrid stent placement combining side-by-side (SBS) and stent-in-stent (SIS) techniques using multi-hole-covered self-expandable metallic stents (MHSEMSs). a The first and second MHSEMSs were deployed into B3 + 4 and B6 in an SBS configuration, followed by the preparation of the third-branch insertion through the side hole. b The third MHSEMS was inserted into B2 using the SIS technique through the side hole of the left stent. c Preparation of the fourth-branch insertion through the side hole. d The fourth MHSEMS was inserted into B5 using the SIS technique through the side hole of the right stent, completing the four-branched hybrid stenting.
A 91-year-old woman with bismuth type IV hilar cholangiocarcinoma initially received two inside plastic stents for the drainage of the right and left hepatic ducts. She was readmitted with acute cholangitis. Bile cultures from both drained and previously undrained intrahepatic ducts (a right hepatic duct during inside stent placement and a left hepatic duct during endoscopic nasobiliary drainage [ENBD]; Fig. 2 ) yielded methicillin-resistant Staphylococcus aureus, necessitating four-branched drainage. Intravenous antibiotics were administered before stent exchange. During ERCP, all previously placed stents and ENBD tubes were removed. Two MHSEMSs (8 mm × 6 cm and 8 cm) were then deployed at B3+4 and B6 in a SBS configuration ( Fig. 3 ). From each SBS stent, a guidewire was advanced through a side hole into the contralateral intrahepatic ducts (B2 and B5, respectively) using an uneven double-lumen cannula (PIOLAX, Kanagawa, Japan) and a radifocus guidewire (Terumo, Tokyo, Japan), which facilitated side-hole passage and enabled SIS deployment of an additional MHSEMS (8 mm × 6 cm; Video 1 , Fig. 4 ). Both technical and clinical success were achieved with no adverse events. The patient maintained an uneventful course without stent-related adverse events for 3 months.
A fluoroscopic image before the current procedure showing two inside plastic stents placed at B5 (right anterior) and B6 (right posterior) ducts, and two 5 Fr endoscopic nasobiliary drainage tubes placed in B3 + 4 and B2.
Side-by-side deployment of multi-hole-covered self-expandable metallic stents at B3 + 4 and B6 across the malignant hilar biliary obstruction.
Hybrid side-by-side and stent-in-stent placement techniques using multi-hole-covered self-expandable metallic stents for four-branched drainage in a bismuth type IV malignant hilar biliary obstruction.Video 1
A final fluoroscopic view demonstrating successful four-branched drainage: stent-in-stent placement from the B3+4 stent to B2 and from the B6 stent to B5, resulting in four fully expanded multi-hole-covered self-expandable metallic stents.
These findings suggest that the MHSEMS may expand therapeutic options for advanced MHBO.
Endoscopy_UCTN_Code_TTT_1AR_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yamada M Ogura T Okuda A Hybrid stent deployment combining side-by-side and stent-in-stent for advanced malignant hilar biliary obstruction Endosc Int Open 20175 E 1231 E 123510.1055/s-0043-118659 · doi ↗
- 2Maruki Y Hijioka S Wu SYS Novel endoscopic technique for trisegment drainage in patients with unresectable hilar malignant biliary strictures (with video)Gastrointest Endosc 20209276376910.1016/j.gie.2020.03.00332169434 · doi ↗ · pubmed ↗
- 3Maruyama H Tanoue K Kurokawa T Stent-in-stent deployment above the papilla to treat malignant hepatic hilar biliary obstruction using novel fully covered multi-hole metal stent Endoscopy 20235501 E 1062 E 106410.1055/a-2158-777637734411 PMC 10513778 · doi ↗ · pubmed ↗
- 4Ogura T Uba Y Kanadani T Stent-in-stent deployment for malignant hilar obstruction using multi-hole stent can prevent tumor ingrowth during 6-month cholangioscopic follow-up Endoscopy 20255701 E 99E 10039909411 10.1055/a-2518-5430 PMC 11798663 · doi ↗ · pubmed ↗
- 5Toyonaga H Hayashi T Sasaki T Side-by-side and stent-in-stent combination placement of three multi-hole metallic stents for malignant hilar biliary obstruction Endoscopy 20225401 E 556E 55710.1055/a-1793-680434911112 · doi ↗