Pioneering Endoscopic Submucosal Dissection in the West: Technique Introduction With a Comprehensive Case Report on the First Application for Oropharyngeal Squamous Cell Carcinoma
Ken Namikawa, Einar Stefan Bjornsson, Helgi Kristinn Sigmundsson, Geir Tryggvason, Sigfus Thor Nikulasson, Jon Gunnlaugur Jonasson, Magnus Konradsson

TL;DR
This paper reports the first Western use of endoscopic submucosal dissection for oropharyngeal cancer, highlighting its potential in Western medicine.
Contribution
The first documented case of ESD for oropharyngeal SCC in the Western world is presented.
Findings
A Caucasian female with superficial oropharyngeal SCC underwent successful ESD with tumor-free margins.
The case demonstrates the feasibility and safety of ESD for oropharyngeal SCC in a Western setting.
The report emphasizes the need to expand the gastroenterologist's role to include pharyngeal surveillance.
Abstract
Endoscopic submucosal dissection (ESD) for pharyngeal squamous cell carcinoma (SCC) has predominantly been performed in Asia but interest in this procedure is growing in the West. This report details the first known Western application of ESD for oropharyngeal SCC. A Caucasian female with superficial oropharyngeal SCC detected during endoscopic surveillance post-ESD for esophageal SCC underwent successful en-bloc resection without complications. Pathology confirmed SCC in situ with tumor-free margins. This case underscores the importance of mindset to include the pharynx in upper gastrointestinal endoscopy during surveillance within the gastroenterologist's domain and the potential for broader application of ESD in the West.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
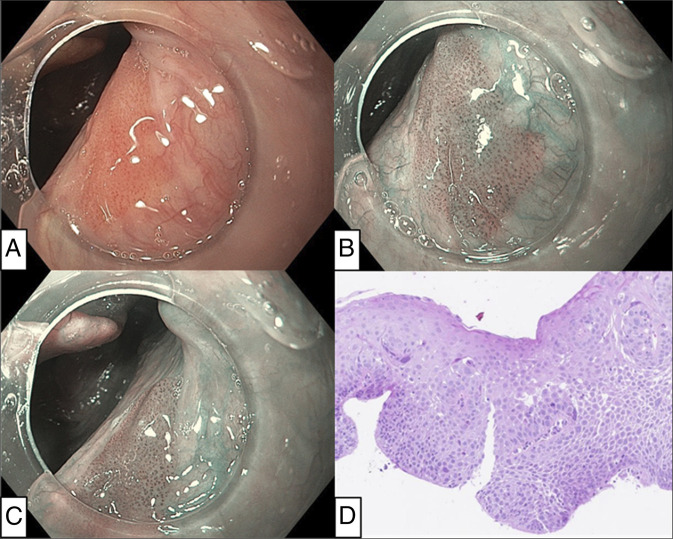 Figure 1
Figure 1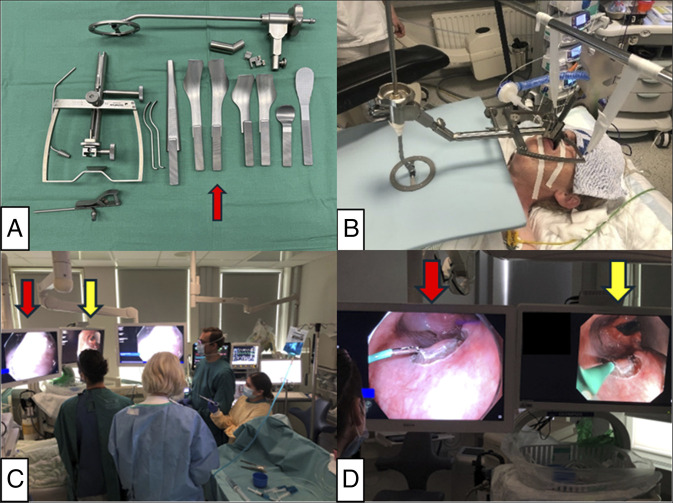 Figure 2
Figure 2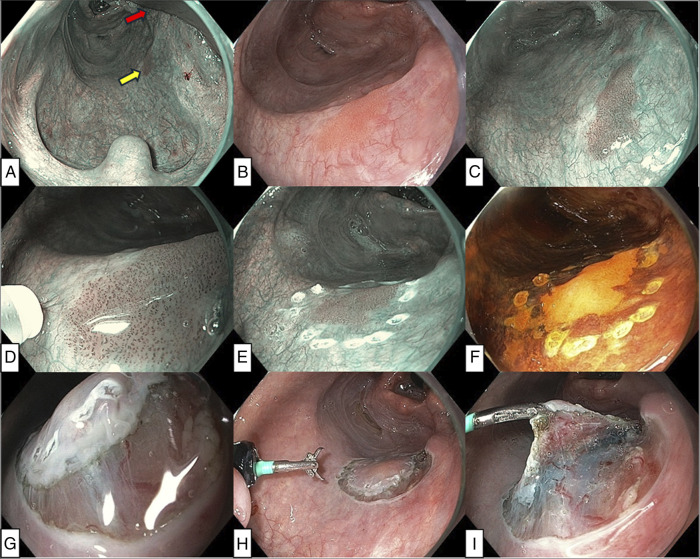 Figure 3
Figure 3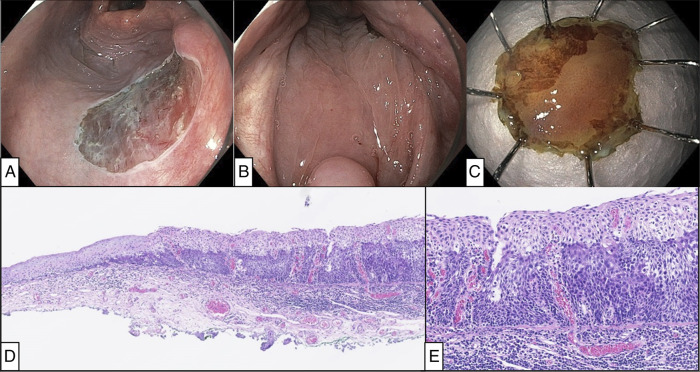 Figure 4
Figure 4| Characteristics | |
| Scope | • Dual Focus gastroscope (EVIS EXERA III GIF-HQ190; Olympus Co. Ltd., Tokyo, Japan) |
| Attachment of scope | Mounted distal attachment cap (D-201-11802; Olympus) |
| Electrical surgical unit | VIO 3 (ERBE Elektromedizin, Tübingen, Germany) |
| Marking | Forced Coagulation mode (Effect 2) |
| Mucosal incision | Endo Cut I mode (Effect 1, Duration 2, Interval 5) |
| Dissection | • Endo Cut I mode (Effect 1, Duration 2, Interval 5) |
| Hemostasis | Soft Coagulation mode (Effect 5) |
| ESD knife | Dualknife J (KD-650U; Olympus) |
| Injection solutions | • 0.9% sodium chloride |
| Retractor | FK-WO Laryngo-Pharyngoscope Retractor (Olympus Europa SE & Co. KG, Hamburg, Germany) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Esophageal Cancer Research and Treatment · Head and Neck Cancer Studies
INTRODUCTION
Pharyngeal squamous cell carcinoma (SCC) patients often present with advanced stage malignancy, which is associated with poor prognosis.^1,2^ By contrast, superficial pharyngeal SCC is potentially curable with endoscopic submucosal dissection (ESD), which offers a minimally invasive and function-preserving local resection.^3–5^ ESD for pharyngeal SCC is established in Asia, but despite a growing interest, to the best of our knowledge, the application of ESD for oropharyngeal SCC in the West has not yet been reported.^3–7^ This paper details the use of ESD technique as treatment with intention for cure of superficial pharyngeal cancer and its outcome through the first case report for oropharyngeal SCC in the West.
CASE REPORT
A 74-year-old White female, with a history of alcohol overconsumption (moderate to severe alcohol disorder with episodes of binging over 40-year periods) and 40 pack-year smoking, had been under surveillance for 5 years after ESD for esophageal SCC. A tumor was identified on the right side of the oropharynx by surveillance upper gastrointestinal (GI) endoscopy, and the biopsy showed conventional SCC (Figure 1).
Endoscopic and histopathological images of oropharyngeal squamous cell carcinoma at diagnosis. (A) The gastroscope with attachment cap revealed a reddish flat lesion in white light imaging. (B) The lesion was more clearly visualized under narrow band imaging. (C) The location of the tumor was at the edge of the right palatopharyngeal arch, according to a relative positional relation to the epiglottis. (D) The biopsy specimen showed severe atypia amounting to conventional squamous cell carcinoma in situ (hematoxylin & eosin stain).
ESD was performed with assistance of a surgical retractor under general anesthesia. After creation of marking-dots around the lesion, a lifting solution was injected into the subepithelium. Subsequently, circumferential mucosal incision was performed with the ESD knife, and subepithelial dissection was performed with the advantage of a double-scope traction method using a regular transoral scope for resection and an ultrathin transnasal scope for traction (Figures 2 and 3).^4^ During and after completion of ESD, hemostasis was provided by a DualKnife with a retracted tip, and major bleeding did not occur. Details of the ESD procedure are presented in Figures 2 and 3 and Table 1. Postoperative pain was well controlled with oral route acetaminophen 4 × 1,000 mg/d and extended-release morphine 10 mg/d. Oral intake could be initiated on postoperative day (POD) 0. She was discharged on POD 1, and no delayed complications occurred. After discharge, pain management was continued with the same oral medications, which she discontinued on POD 7. The final pathology diagnosis from ESD specimen was pharyngeal SCC (conventional type) in situ with tumor-free margin (0.3-mm vertical and 2-mm lateral margin) (Figure 4).
Preoperative and intraoperative photographs of procedure-setup. (A) FK-WO Laryngo-Pharyngoscope Retractor system. The blade for right-sided tongue base lesions (red arrow) was chosen in this case. (B) Patient positioning and laryngo-pharyngoscope retractor setup. A transoral retractor provided wide exposure of the pharynx. (C) Endoscopy room setup during the procedure. The primary display monitor (red arrow) for transoral gastroscopy and the secondary display monitor (yellow arrow) for transnasal ultrathin gastroscopy were placed. (D) The primary display monitor (red arrow) showed a video image from the transoral gastroscope for resection and the secondary display monitor (yellow arrow) showed the image from the transnasal ultrathin gastroscope for traction. FK-WO, Feyh-Kastenbauer-Weinstein-O’Malley.
Intraoperative endoscopic images. (A) A wide exposure of the oropharynx was achieved by lifting the larynx by the retractor blade (red arrow), providing adequate working space and optimal visualization of the lesion (yellow arrow). (B) The entire form of the tumor was observed as a 12-mm sized reddish flat lesion. (C) The lesion was visualized more clearly as a brownish area under narrow band imaging (NBI). (D) Marking was performed under near-focus NBI. Irregular intraepithelial papillary capillary loops were observed in the lesion, corresponding to type B1 vessels according to the magnifying endoscopic classification of the Japan Esophageal Society for esophageal squamous cell carcinoma.13 (E) Marking dots were placed around the lesion. (F) The border of the lesion was confirmed by iodine staining. The lesion was visualized as an unstained area. (G) Mucosal incision outside the marking dots. The typically thin mucosal epithelium of the pharynx was observed. (H) After circumferential incision, transnasal endoscopy with an ultra-slim gastroscope was performed to grasp the specimen for traction. (I) Double-scope traction method provided a better visualization of the layer for dissection.6
Postoperative endoscopic and histopathological images. (A) En block resection was achieved. (B) The view of the pharynx without the retractor. Most of the mucosal defect was covered by the lateral wall of the oropharynx. (C) Tumor was visualized as an unstained area by iodine staining in ESD specimen. (D) Histology of the resection specimen showing conventional squamous cell carcinoma in situ to the right and normal epithelium towards the left. Chronic inflammatory infiltration was present in underlying stroma (hematoxylin & eosin stain). (E) Higher power picture of conventional squamous cell carcinoma in situ in the resection sample showing full-thickness epithelial atypia. Lymphocytic infiltration was present in the underlying stroma, but no evidence of invasive tumor (hematoxylin & eosin stain). ESD, endoscopic submucosal dissection.
DISCUSSION
A systematic review and meta-analysis by Kamal et al found all the included studies on ESD for pharyngeal SCC were from Asia, highlighting the need for studies from Western countries to validate their findings.^5^ To date, only 2 endoscopically treated pharyngeal cancers have been reported in the West: 1 ESD in France and 1 endoscopic mucosal resection in the United States for hypopharyngeal SCCs.^7,8^
This disparity may stem from lack of screening programs, routine examinations in the pharynx, and experience in diagnosing and treating superficial pharyngeal SCC. Gastroenterologists typically exclude the examination in the pharynx from upper GI endoscopy, assuming it beyond their purview.^9^ However, we believe that early detection of pharyngeal cancers should fall within the gastroenterologist's domain, given its association with esophageal SCC, as both share etiological factors such as alcohol consumption and smoking.^1,9,10^ Gastroenterologists diagnose and treat esophageal SCCs using a high-resolution endoscope, which could be effectively extended to the pharynx.
For successful pharyngeal cancer screening, narrow band imaging (NBI) is efficient since the established NBI-findings in esophageal SCC are applicable to the pharynx.^10,11^ Adequate sedation is essential for proper examination to manage swallowing and avoid eliciting the gag reflex. It is also important to be aware of potential pitfalls due to the blind spots in the pharynx such as epiglottic vallecula, lateral wall of oropharynx, and deep hypopharynx.
ESD offers a high en-block resection rate, which is advantageous over endoscopic mucosal resection.^5^ Although comparative studies with minimally invasive surgical treatment modalities are lacking, potential advantages of ESD include cost effectiveness, and precise function sparing resection due to the maneuverability of the flexible endoscope.^5^
Nevertheless, there are some special properties for ESD in the pharynx compared with other GI tract areas that are important to note. It carries a risk of respiratory failure due to laryngeal edema or delayed bleeding. In addition, it demands unique technical expertise in the limited working-space and requires general anesthesia and larynx-lifting.
The current case demonstrated the feasibility of early-stage SCC detection by a meticulous endoscopic inspection, integrating risk factor awareness; prior esophageal SCC, and excessive alcohol/tobacco consumption. Although routine screening endoscopic investigations in the pharynx may be impractical in the West, targeted evaluation in high-risk individuals could be valuable. Oropharyngeal lesions are frequently overlooked in upper GI endoscopy due to anatomical complexity, as shown in Figure 4, but the use of NBI, an attachment cap, and awareness of blind spots helped early detection in our case, demonstrating typical findings of superficial SCC (Figures 1 and 2)^9–11^.
Modifying routines and mindsets to incorporate the pharynx in upper GI endoscopy, based on individual risk profiles, may be more crucial and challenging than the actual process of learning how to recognize pharyngeal SCC.
ESD access in the pharynx requires larynx-lifting, often achieved with support from otolaryngologists/head and neck surgeons, and specialized retractor.^3–5^ In this case, A common retractor system for head and neck surgery was successfully applied by endoscopists and anesthesiologist, allowing for an efficient procedure (Figure 1). Double-scope traction method efficiently facilitated dissection (Figure 3)^4^. ESD allowed for resection without excess margin, minimizing mucosal defect and muscularis damage, as shown in Figure 4. This probably contributed to rapid postoperative recovery.
In conclusion, early detection of pharyngeal SCC should preferably be incorporated in the objectives of upper GI endoscopy when indicated. ESD for pharyngeal SCC may offer potential benefits in patient management; however, further studies from the West are needed to validate current findings. As Western centers gain more experience with ESD in other GI locations, the time has come to consider broader implementation into the pharynx.^12,13^
DISCLOSURES
Author contributions: K. Namikawa and M. Konradsson substantially contributed to the conception of the work. K. Namikawa, HK Sigmundsson, G. Tryggvason, and M. Konradsson made contribution to collecting and analysis in clinical data. ST Nikulasso and JG Jonasson made contribution to collecting and analysis in pathological data. K. Namikawa made the manuscript drafting ES Bjornsson and M. Konradsson made substantial contribution to the manuscript editing. All authors critically reviewed and revised the manuscript draft and approved the final version for submission. K. Namikawa is the article guarantor.
Financial disclosure: None to report.
Previous presentation: This case was presented at the European Society for Diseases of the Esophagus (ESDE) congress 2025; May 11–13, 2025; Amsterdam, the Netherlands.
Informed consent was obtained for this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Johnson DE Burtness B Leemans Cr Lui VWY Bauman JE Grandis JR. Head and neck squamous cell carcinoma. Nat Rev Dis Primers. 2020;6(1):92. Erratum in: Nat Rev Dis Primers. 2023 Jan 19;9(1):4.36658129 10.1038/s 41572-023-00418-5 · doi ↗ · pubmed ↗
- 2Hall SF Groome PA Irish J . The natural history of patients with squamous cell carcinoma of the hypopharynx. Laryngoscope. 2008;118(8):1362–71.18496152 10.1097/MLG.0b 013e 318173 dc 4a · doi ↗ · pubmed ↗
- 3Iizuka T Kikuchi D Hoteya S . Clinical advantage of endoscopic submucosal dissection over endoscopic mucosal resection for early mesopharyngeal and hypopharyngeal cancers. Endoscopy. 2011;43(10):839–43.21833903 10.1055/s-0031-1271112 · doi ↗ · pubmed ↗
- 4Yoshio T Tsuchida T Ishiyama A . Efcacy of double-scope endoscopic submucosal dissection and long-term outcomes of endoscopic resection for superfcial pharyngeal cancer. Gastroenterol Endosc. 2017;59:2750–9.10.1111/den.1271227525634 · doi ↗ · pubmed ↗
- 5Kamal F Khan MA Lee-Smith W . Outcomes of endoscopic submucosal dissection for treatment of superficial pharyngeal cancers: Systematic review and meta-analysis. Dig Dis Sci. 2022;67(8):3518–28.34505257 10.1007/s 10620-021-07225-6 · doi ↗ · pubmed ↗
- 6Swei E Wagh MS. Endoscopic submucosal dissection in the pharynx: Let's start at the very beginning! Gastrointest Endosc. 2021;93(4):828–30.33741087 10.1016/j.gie.2020.09.010 · doi ↗ · pubmed ↗
- 7Jacques J Rivory J Lépilliez V . Tunnel and clip endoscopic submucosal dissection of a pharyngeal superficial squamous cell carcinoma detected with narrow-band imaging. Endoscopy. 2017;49(S 01):E 48–E 50.28068703 10.1055/s-0042-122142 · doi ↗ · pubmed ↗
- 8Mou S Kaltenbach T Yao M Soetikno R. Superficial pharyngeal cancer can be diagnosed in the West. Endoscopy. 2011;43(Suppl 2 UCTN):E 248–9.21837597 10.1055/s-0030-1256419 · doi ↗ · pubmed ↗