Evaluation of Operative Vaginal Delivery Practices and Maternal-Neonatal Outcomes
Falak Baloch, Maryam Javed, Liliana Grosu

TL;DR
This study evaluated vaginal delivery practices at a hospital, finding high success rates but identifying areas for improvement in documentation and post-procedure care.
Contribution
The study provides a detailed audit of operative vaginal delivery practices and outcomes, highlighting specific areas needing improvement in a specific hospital setting.
Findings
Operative vaginal deliveries had a 100% procedural success rate with documented indications in 96.8% of cases.
Areas needing improvement included post-procedure debriefing (16.1%), antibiotic prophylaxis (70.9%), and postnatal VTE assessment (90.3%).
Abstract
Background Operative vaginal deliveries (OVDs), including vacuum and forceps-assisted births, are essential interventions for prolonged second-stage labor or fetal compromise. Despite declining global rates, adherence to clinical guidelines and proper documentation remains crucial for maternal and neonatal safety. This audit aimed to evaluate operative vaginal delivery practices at Bedford Hospital, including adherence to Royal College of Obstetricians and Gynaecologists (RCOG) and local guideline recommendations and associated maternal and neonatal outcomes. The audit also aimed to identify areas for improvement to enhance patient safety and quality of care. Methodology A retrospective audit included all women (n = 62) undergoing attempted OVDs from September to December 2024. Data were extracted from electronic maternity records and NerveCenter, assessing instrument type, success…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
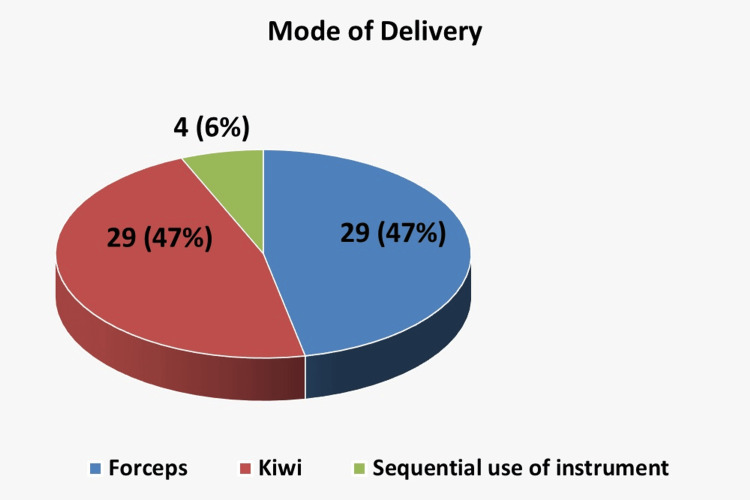 Figure 1
Figure 1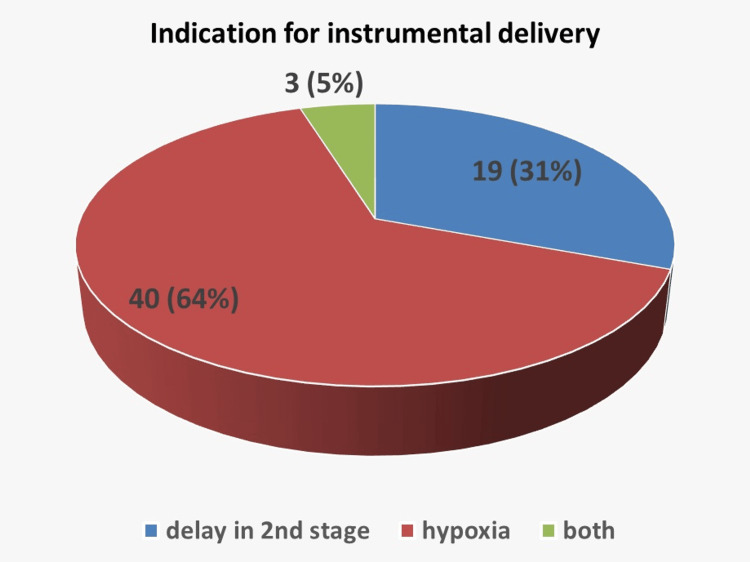 Figure 2
Figure 2| Characteristic | Category/Measurement | n (%) or mean ± SD |
| Mode of instrument | Vacuum | 29 (46.8%) |
| Forceps | 29 (46.8%) | |
| Sequential | 4 (6.4%) | |
| Operator | Registrar | 57 (91.9%) |
| Consultant | 5 (8.1%) | |
| Consultant presence | Present | 22 (35.5%) |
| Not present | 40 (64.5%) | |
| Delivery location | Delivery suite | 39 (62.9%) |
| Theater | 23 (37.1%) | |
| Maternal outcomes | Third-degree perineal tear | 4 (6.45%) |
| Estimated blood loss >1,000 mL | 8 (12.9%) | |
| MOH | 2 (3.2%) | |
| Antibiotic prophylaxis | Given | 44 (70.9%) |
| Not given | 18 (29.1%) | |
| Postnatal VTE assessment completed | Yes | 56 (90.3%) |
| No | 6 (9.7%) | |
| Debrief documented | Yes | 10 (16.1%) |
| No | 52 (83.9%) | |
| Neonatal outcomes | SCBU admission | 2 (3.2%) |
| Shoulder dystocia | 4 (6.5%) | |
| APGAR <5 at birth | 1 (1.6%) | |
| APGAR <7 at 5 minutes | 1 (1.6%) | |
| Arterial pH <7.10 | 3 (4.8%) | |
| Birth weight >4 kg | 8 (12.9%) | |
| Maximum pulls required | 1–4 pulls | 1 case with 4 pulls (Kiwi vacuum) |
| Characteristic | Category/Measurement | n (%) or mean ± SD |
| Parity | Primiparous | 47 (75.8%) |
| Para 1 | 11 (17.7%) | |
| Para 2 | 3 (4.8%) | |
| Para 3 | 1 (1.6%) | |
| Gestational age (weeks) | 34–37 | 9 (14.5%) |
| 37–41 | 45 (72.6%) | |
| 41–42 | 8 (12.9%) | |
| Maternal BMI (kg/m²) | <20 | 3 (4.8%) |
| 20–25 | 25 (40.3%) | |
| 26–30 | 26 (41.9%) | |
| >30 | 11 (17.7%) | |
| Labor onset | Spontaneous | 36 (58.1%) |
| Induced | 26 (41.9%) | |
| Analgesia | Entonox | 29 (46.8%) |
| Pethidine | 10 (16.1%) | |
| Mode of instrument | Vacuum | 29 (46.8%) |
| Forceps | 29 (46.8%) | |
| Sequential | 4 (6.4%) | |
| Consultant presence | Present | 22 (35.5%) |
| Not present | 40 (64.5%) | |
| Delivery location | Delivery suite | 39 (62.9%) |
| Theater | 23 (37.1%) | |
| Maternal outcomes | Third-degree perineal tear | 4 (6.45%) |
| EBL >1,000 mL | 8 (12.9%) | |
| Neonatal outcomes | SCBU admission | 2 (3.2%) |
| Shoulder dystocia | 4 (6.5%) | |
| APGAR <5 at birth | 1 (1.6%) | |
| APGAR <7 at 5 minutes | 1 (1.6%) | |
| Arterial pH <7.10 | 3 (4.8%) | |
| Birth weight >4 kg | 8 (12.9%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and Perinatal Health Interventions · Surgical site infection prevention · Enhanced Recovery After Surgery
Introduction
Operative vaginal delivery (OVD) refers to a vaginal delivery in which forceps or a vacuum device are used to assist the birth [1]. Indications for performing an OVD include a prolonged second stage of labor, evidence or risk of fetal distress, and the need to expedite delivery to assist the mother [2].
Instrumental deliveries account for 10-15% of all births and are associated with higher maternal and neonatal morbidity, which contributes to an increased risk of litigation [3]. Instrumental deliveries carry an increased risk of maternal and neonatal injury. Maternal complications may result in significant functional issues, such as fecal incontinence, which can have a profound impact on quality of life. Therefore, it is essential to obtain informed consent before any medical procedure [4].
Rates of OVDs have been declining globally, with a particularly marked reduction in the use of obstetric forceps. This trend has occurred alongside rising cesarean section rates worldwide, raising concerns about the diminishing proficiency in OVD techniques as cesarean delivery (CD) becomes increasingly favored [5]. Over the past three decades, CD rates and the incidence of associated accreta spectrum disorders have risen steadily, while the use of OVD and trials of labor after cesarean have declined. The effects of obstetric surgery on reproductive outcomes and future fertility options remain clinically significant [6].
According to the Royal College of Obstetricians and Gynaecologists (RCOG) Green-Top Guideline No. 26 (April 2020), it is crucial to know when to discontinue the procedure, the maximum number of attempts or pulls permitted, and the point at which the instrument should be abandoned to ensure patient safety [7]. The safe and effective use of OVDs requires adherence to established guidelines, proper training, and continuous audit of clinical outcomes.
Audit and research on OVD practices help identify gaps in clinical practice, assess compliance with guidelines, and improve maternal and neonatal outcomes. This study aimed to evaluate the patterns, indications, and outcomes of OVDs in our institution over a specified period, providing insights into current practice and areas for quality improvement. This audit was conducted at Bedford Hospital, part of the Bedfordshire Hospitals NHS Foundation Trust in the East of England. The audit standards were based on the RCOG Green-top Guideline No. 26 as well as local trust guidelines.
Materials and methods
This was a retrospective audit conducted at Bedford Hospital, part of the Bedfordshire Hospitals NHS Foundation Trust in the East of England, over a four-month period from September to December 2024. All women who underwent attempted instrumental vaginal delivery during the study period were included, regardless of whether the procedure was successful. No specific exclusion criteria were applied. A total of 62 women met the inclusion criteria. A consecutive non-probability sampling approach was used, including all eligible cases during the audit period.
Data were extracted from electronic records (Mediviewer), including maternity and delivery notes, with additional information regarding antibiotic administration and venous thromboembolism (VTE) prophylaxis (Tinzaparin) obtained from the NerveCenter system. The audit assessed adherence to specific parameters outlined in the RCOG Green-top Guideline No. 26 (April 2020) and local trust protocols. These parameters included documentation of indication for OVD, type of instrument used, number of pulls, procedural success, decision-to-delivery intervals, operator grade, consultant presence, written consent, post-procedure debriefing, administration of antibiotic prophylaxis, and completion of postnatal VTE assessment. Maternal outcomes assessed included third-degree perineal tears, estimated blood loss >1,000 mL, and massive obstetric hemorrhage. Neonatal outcomes included special care baby unit (SCBU) admission, shoulder dystocia, APGAR scores, arterial pH, and birth weight.
Decision-to-delivery intervals were evaluated against standards: ≤30 minutes for cardiotocography concerns and ≤75 minutes for prolonged second stage of labor. Maternal and neonatal outcomes, documentation quality, and adherence to RCOG Green-top Guideline No. 26 and local trust guidelines were also assessed. Compliance with RCOG Green-top Guideline No. 26 and local trust guidelines was assessed for all parameters [7]. All parameters were pre-defined to ensure that the audit could be reproduced in other settings using the same standards.
Data were analyzed descriptively, with categorical variables presented as frequencies and percentages and continuous variables summarized using mean ± standard deviation where applicable. Ethical approval for the audit was granted by the Bedford Hospital audit department, and individual patient consent was not required due to the retrospective nature of the study and anonymization of data.
Results
Between September and December 2024, 62 OVDs were performed. The monthly rate of instrumental deliveries was 9/225 (4%) in September, 16/211 (7.58%) in October, 25/198 (12.6%) in November, and 12/224 (5.36%) in December. All procedures were successful, achieving a 100% (62/62) success rate. The indication for instrumental delivery was documented in 96.77% (60/62) of cases, with only two instances not documented by the doctor but noted in the midwife’s records. The distribution of indications is illustrated in Figure 1, showing the proportion of cases due to delay in the second stage of labor, suspected fetal hypoxia, or both.
Distribution of operative vaginal deliveries by instrument type (vacuum, forceps, sequential use).
Overall, decision-to-delivery intervals ranged from 3 to 73 minutes. Five (5/62, 8.1%) cases did not meet the recommended decision-to-delivery interval criteria. Of these, one case was delayed due to temperature issues in the theater; an alternative theater was arranged, the incident was reported, and later investigated. Another case was delayed because an instrument was initially applied but removed due to absent contractions; oxytocin was subsequently initiated, and the instrument was reapplied. For the remaining three cases, no specific cause for the delay could be identified from the documentation.
Vacuum and forceps were used equally, with 29 cases each (29/62;46.8%), while sequential instruments were required in four (4/62; 6.4%) cases, as shown in Figure 2. Registrars performed 57 of the deliveries (57/62; 91.9%), and consultants performed five (5/62; 8.1%); a consultant was present in 22 (22/62; 35.5%) cases. Overall, 39 deliveries occurred in the delivery suite room (39/62; 62.9%), while 23 were conducted in theatre (23/62; 37.1%). All doctors performing the procedures were deemed competent. Appropriate trial of instrumental delivery was ensured in cases with occiput posterior, occiput transverse, or high head with caput/moulding. Indications for instrumental delivery were documented in 60/62 (96.8%) cases, and consent was documented in 96.8% of cases, either written (for theatre deliveries) or verbal (for delivery-suite births). The operative details, maternal outcomes, and neonatal outcomes are summarized in Table 1.
Pie chart showing the distribution of indications for operative vaginal delivery.
Maternal outcomes included four third-degree perineal tears (6.45%) and estimated blood loss over 1,000 mL in eight women. Two women experienced massive obstetric hemorrhage, which is described below to highlight learning points.
Case 1, with massive obstetric hemorrhage of 2,200 mL, was a 31-year-old primiparous, white British woman with a body mass index (BMI) of 25.9 kg/m² who underwent a Kiwi vacuum delivery for a full-term pregnancy at 09:05 with two pulls. The baby was born in good condition. The placenta was delivered at 09:44, but the cord snapped during controlled cord traction, and the placenta appeared incomplete. Two additional pieces of placenta were removed on vaginal examination. Despite administration of oxytocin, ergometrine, tranexamic acid, and a single dose of hemabate, bleeding continued. A code red was called at 1,000 mL estimated blood loss due to uterine atony and retained placenta. Bimanual compression was performed. Pre-delivery hemoglobin was 118 g/L, and post-delivery hemoglobin was 63 g/L; one unit of red blood cells was transfused. Surgery for manual removal of the placenta was delayed due to another ongoing emergency and consent process. Surgery was performed in the theater under spinal anesthesia at 11:32. She recovered well, but no debrief or senior review was documented. Learning point from this case was to escalate promptly to the consultant and matron on call.
Case 2, with massive obstetric hemorrhage of 1,940 mL, was a 30-year-old primiparous woman with a BMI of kg/m² who underwent a forceps delivery with episiotomy at 17:51 due to fetal tachycardia. Two pulls were performed in the delivery room, and the baby was born in good condition. Postpartum hemorrhage was both traumatic and atonic. Management included oxytocin bolus, ergometrine, tranexamic acid, and one dose of hemabate. Episiotomy suturing was completed at 18:24, and bleeding was brought under control. Learning point from this case was to improve monitoring of estimated blood loss, escalate promptly, initiate a massive obstetric hemorrhage call, and document debrief.
Sequential instruments were successfully used in four women, with only one neonate requiring SCBU admission. Antibiotic prophylaxis was administered in 70.9% of women, while postnatal VTE assessments were completed in 90%. Debriefing was documented in only 16% of cases.
Neonatal outcomes were favorable overall. Two babies were admitted to the SCBU, four experienced shoulder dystocia, and one had an APGAR score <5 at birth, while another had an APGAR score <7 at five minutes. Three babies had an arterial pH <7.10, and eight had a birth weight above 4 kg. The maximum pulls recorded were four, with only one case requiring four pulls using a Kiwi vacuum.
Patient demographics showed 47 primiparous women (47/62; 75.8%), 11 para 1 (11/62; 17.7%), 3 para 2 (3/62; 4.8%), and 1 para 3 (1/62; 1.6%). The majority (45) had gestational ages between 37 and 41 weeks, nine between 34 and 37 weeks, and eight between 41 and 42 weeks. BMI distribution included three women <20 kg/m², 25 women 20-25 kg/m², 26 women 26-30 kg/m², and 11 women >30 kg/m². Induction of labor was performed in 26 (26/62; 41.9%) women, with the remaining 36 undergoing spontaneous onset of labor (36/62; 58.1%). Analgesia was appropriately provided in all cases, with 29 women receiving Entonox (29/62; 46.8%) and 10 receiving pethidine (10/62; 16.1%). Patient demographics and clinical characteristics are summarized in Table 2.
Overall, the audit demonstrated that OVDs in this cohort were conducted safely with high success rates and appropriate indications. Areas for improvement included documentation of debriefing, postnatal VTE assessment completion, and ensuring antibiotic prophylaxis adherence. The two massive obstetric hemorrhage cases emphasize the importance of timely escalation, senior review, and structured debriefing to optimize patient safety.
Discussion
This audit reviewed 62 OVDs over a four-month period. The overall rate of instrumental deliveries ranged from 4% to 12.6% monthly, which aligns with national and international reports indicating rates ranging between 5% and 15% depending on the obstetric population and institutional practice [7,8]. The 100% procedural success rate demonstrates safe and effective practice, consistent with studies showing that with proper training, OVDs can be performed with high success and low morbidity [9]. This aligns with recent studies indicating high success rates for vacuum-assisted deliveries, with one study reporting a 97.3% success rate for vacuum attempts [10].
Documentation of indications and consent was achieved in most cases (96.77% and 92%, respectively), although this remains similar to the previous audit, indicating persistent gaps in record-keeping. A recent study highlighted that documentation compliance remains a challenge, with many OVDs lacking complete documentation, including indications and consent [11]. This underscores the need for standardized documentation practices to enhance clinical accountability and communication.
Compliance with decision-to-delivery intervals was comparable to the previous audit (92% versus 93%), which is in line with current guidelines recommending timely intervention in second-stage complications [12]. Maternal outcomes were largely favorable, with low rates of third-degree perineal tears (6.45%), and most patients experienced manageable blood loss. While two cases of massive obstetric hemorrhage were observed, it is important to note that these are recognized complications that can also occur in spontaneous vaginal deliveries. Therefore, these events cannot be attributed solely to the use of instruments but highlight the importance of prompt escalation, senior review, and structured debriefing, as recommended in national guidelines for the management of postpartum hemorrhage [13]. Recent guidelines emphasize the use of a treatment bundle for the management of postpartum hemorrhage, which was followed in these cases, including uterotonics, tranexamic acid, and escalation of care if bleeding persists [14].
Sequential instruments were used safely in four women, all resulting in successful deliveries, demonstrating that complex operative techniques can be performed effectively with appropriate supervision [15]. This is consistent with recent studies indicating that when performed by trained professionals, sequential instrument deliveries can be safe and effective [12].
Neonatal outcomes were reassuring, with minimal need for SCBU admission and isolated cases of low APGAR scores or shoulder dystocia. These findings are consistent with previous studies indicating that OVD, when appropriately indicated and performed by trained staff, is generally safe for the neonate [16,17]. Areas for improvement identified include post-procedure debriefing (documented in only 16%), completion of postnatal VTE assessment (90%), antibiotic prophylaxis adherence (70.9%), and paired cord gas collection (77.4%). Addressing these gaps aligns with best-practice recommendations and will further enhance patient safety and quality of care.
Recommendations
Based on the findings of this audit, several measures are recommended to improve the safety and quality of OVDs. Implement the use of a delivery categorization sticker to classify deliveries, operative vaginal or cesarean, based on urgency (Category 1 or 2) and indicate the recommended location (delivery suite room or theatre). This tool will support timely decision-making, ensure appropriate escalation of care, and improve adherence to recommended decision-to-delivery intervals in line with RCOG guidelines. Although the sticker is copyright-protected and cannot be shared externally, its implementation is intended to further enhance compliance with guidelines and support quality improvement in future audits. The delivery categorization sticker has been implemented to improve decision-making and adherence to decision-to-delivery intervals.
A standardized documentation template should be developed to capture essential details, including in-room consent, a clear indication for the procedure, and a structured post-procedure debrief, which will help address persistent gaps in record-keeping. Antibiotic prophylaxis should be administered consistently as a single dose post-delivery when indicated, and paired cord gases should be collected for all babies to ensure comprehensive neonatal assessment and documentation. Re-audit in six months is recommended to evaluate the effectiveness of these interventions and monitor ongoing compliance with best practice standards.
Limitations
This audit has a few limitations. As it was conducted at a single center, the findings may not apply to other hospitals. Only short-term maternal and neonatal outcomes were assessed, and no long-term follow-up was performed. It is important to note that the primary aim of this audit was to evaluate adherence to guidelines and recommendations for OVDs, including documentation, decision-to-delivery intervals, and immediate procedural outcomes. Long-term follow-up of women who sustained obstetric anal sphincter injuries was not within the scope of this audit, but can be explored in a separate prospective study focusing on maternal recovery and patient perceptions after OVD.
Conclusions
This audit demonstrated that OVDs in this cohort were performed safely, with high success rates and appropriate indications. Maternal and neonatal outcomes were generally favorable, including in cases requiring sequential instruments. However, rare but significant complications, such as massive obstetric hemorrhage, underscore the importance of timely escalation, senior review, and structured debriefing. Focused efforts on improving documentation, adherence to post-delivery protocols, and systematic monitoring will help maintain and further enhance the quality of care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Operative vaginal delivery Obstet Gynaecol Reprod Med Horan MA Murphy DJ 358363262016
- 2Comparison of maternal and fetal outcomes of operative vaginal deliveries using vacuum and forceps in a tertiary hospital Compr Med Buhur A ÖncüN 95100172025 http://10.14744/cm.2025.55707
- 3Operative vaginal deliveries at a district general hospital - an audit Arch Dis Child Fetal Neonatal Ed Latheef R Makandar R Roberts L 08952010
- 4Are women adequately informed about the use of instrumentation during vaginal delivery? A prospective review of the information on instrumental delivery provided to pregnant women and a retrospective review of the quality of consent for instrumental delivery Colorectal Dis Orlando A Thomas GP Fernando R Murphy J Elsaid N Dilke S Vaizey CJ 027202510.1111/codi.70050 PMC 1189741640069948 · doi ↗ · pubmed ↗
- 5Trends in operative vaginal delivery rates: a 20-year retrospective analysis in Ireland Int J Gynaecol Obstet Kane D Daly R Tunney E 1339134016820253942259010.1002/ijgo.15973 PMC 11823293 · doi ↗ · pubmed ↗
- 6Fostering excellence in obstetrical surgery J Healthc Leadersh Wilson RD 355373152023 http://10.2147/JHL.S 4044983804653410.2147/JHL.S 404498 PMC 10691271 · doi ↗ · pubmed ↗
- 7Royal College of Obstetricians and Gynaecologists. Assisted vaginal birth (Green-top guideline No 26 10 2025 2020 https://www.rcog.org.uk/guidance/browse-all-guidance/green-top-guidelines/assisted-vaginal-birth-green-top-guideline-no-26/10.1111/1471-0528.1609232346983 · doi ↗ · pubmed ↗
- 8Trends in operative vaginal delivery rates and associated maternal complication rates in an inner-city hospital Am J Obstet Gynecol Kabiru WN Jamieson D Graves W Lindsay M 1112111418420011134917210.1067/mob.2001.115178 · doi ↗ · pubmed ↗