Emergence of BRCA Reversion Mutations in Prostate Cancer Prior to PARP Inhibitor Exposure: Clinical and Therapeutic Implications
Douglas I. Lin, Elizabeth Lawrence, Natalie Danziger, Huihui Ye, Brennan Decker, Ole Gjoerup, Ryon P. Graf, Jeffrey S. Ross, Richard S. P. Huang, Julia A. Elvin, Douglas A. Mata, Rana R. McKay

TL;DR
This study finds that BRCA reversion mutations can occur in prostate cancer patients before they receive PARP inhibitors, often after chemotherapy or radiation, which may lead to resistance.
Contribution
The study reveals that BRCA reversion mutations can emerge in prostate cancer prior to PARP inhibitor treatment, suggesting DNA-damaging therapies may promote resistance.
Findings
BRCA reversion mutations were detected in 30% of patients without prior PARP inhibitor exposure.
Patients with prior chemotherapy had shorter PARP inhibitor response durations compared to chemotherapy-naïve patients.
DNA-damaging therapies like chemotherapy and radiation may promote BRCA reversion mutations and primary resistance.
Abstract
Inactivating BRCA1/2 mutations confer sensitivity to poly(ADP‐ribose) polymerase inhibitors (PARPi) in prostate cancer (PCA). However, secondary BRCA1/2 reversion mutations (BRCArev) can restore BRCA function and mediate acquired PARPi resistance. While BRCArev typically arise under PARPi selective pressure, their occurrence in PARPi‐naïve settings remains incompletely understood. We sought to characterize the frequency, clinical context, and therapeutic correlates of BRCArev detection in men with advanced PCA, including those without prior PARPi exposure. We restrospectively analyzed clinical liquid biopsy results from men with PCA using FoundationOneLiquid CDx between January and December 2023. BRCArev were defined as sequence alterations predicted to restore open reading frame of BRCA1 or BRCA2 harboring pathogenic inactivating variants. Clinical and treatment histories, including…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
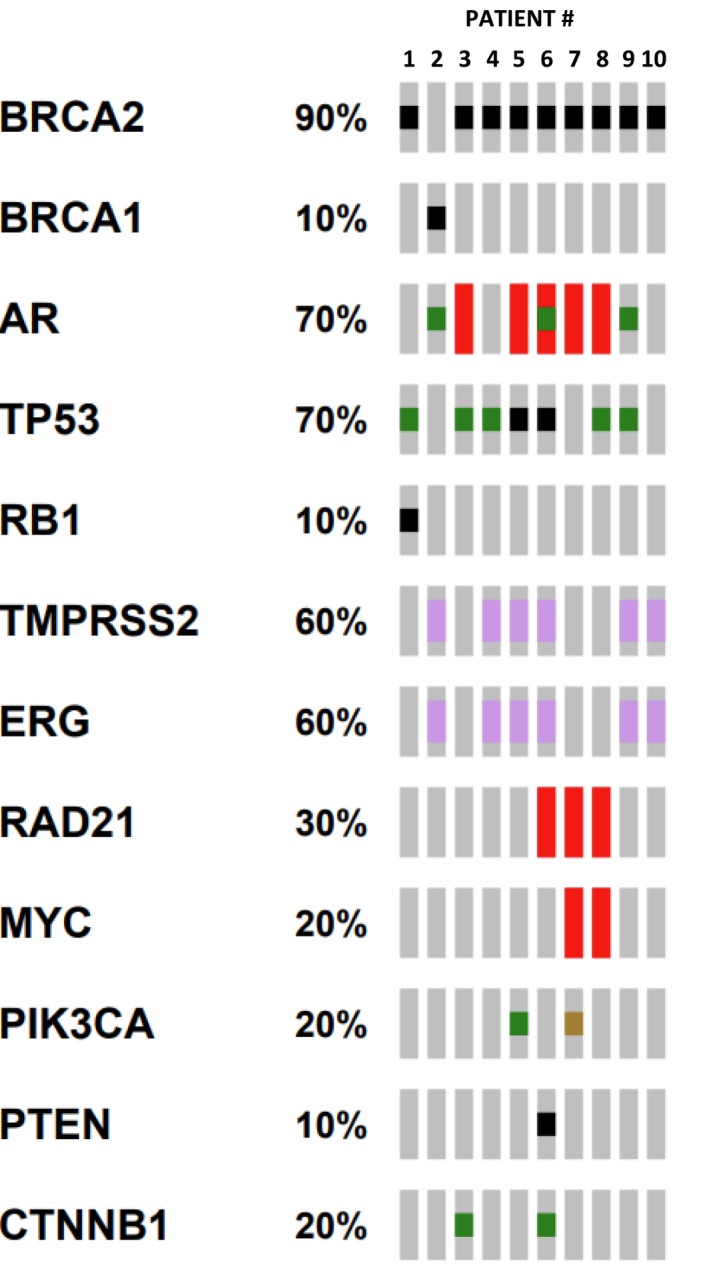 FIGURE 1
FIGURE 1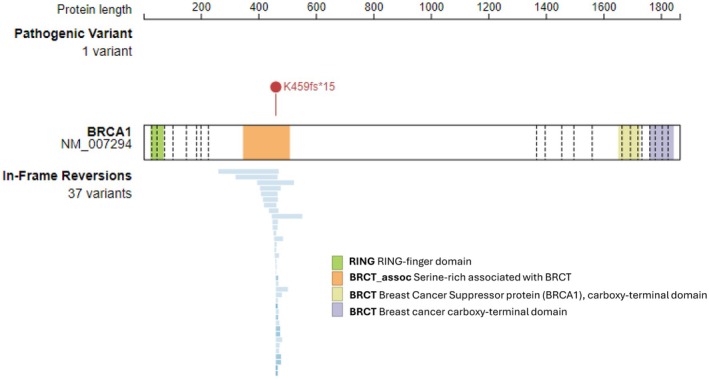 FIGURE 2
FIGURE 2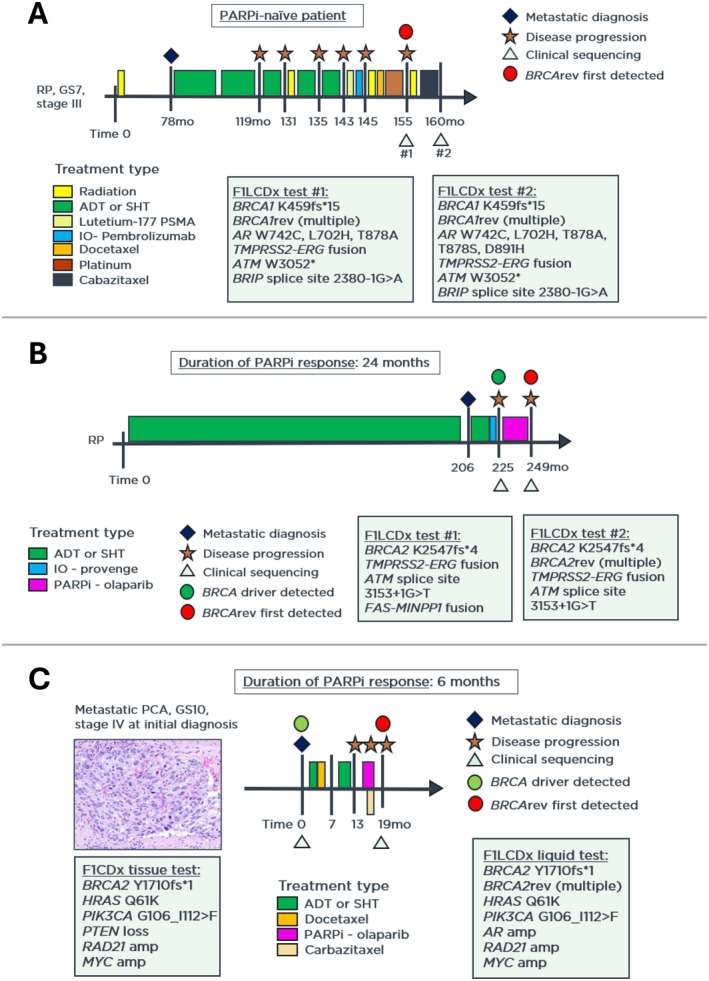 FIGURE 3
FIGURE 3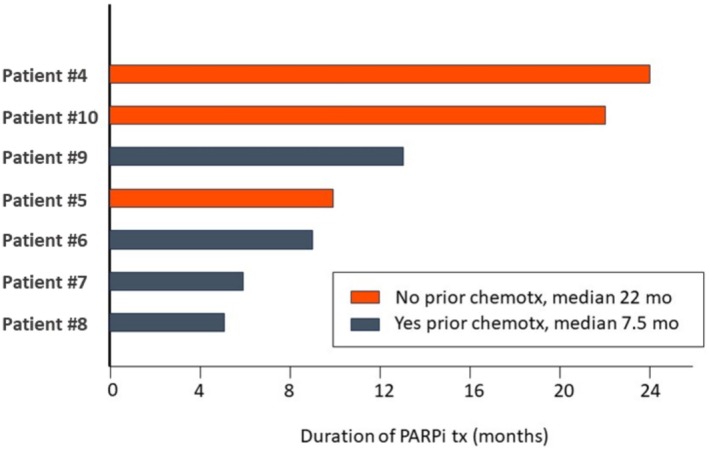 FIGURE 4
FIGURE 4| n | Original |
| PCA type | Prior PARPi | Duration of PARPi | Initial PARPi response | Castration resistant | Prior chemo | Prior XRT | Progression after PARPi |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 |
| T2542K, K2538fs*14, A2534fs*18 | NE | None | N/A | N/A | No | Yes, platinum | Yes | N/A |
| 2 |
|
K459_V477 > NLGKPIGRRQASP, K459_K467 > NLGIVFP, E404_H476del, A407_Y465del, K459_Y465 > NLGN, K459_K501 > NLGKPIGRRQASP, D435_K468 > E, E445_S551del, K459_V477 > NLGKPIGRRQASPI, G394_D522 > Y, K459_K468 > NL, K459_Y465 > NLGKP, K459_K467 > NLG, S454_G462del, K459_L474 > NLGKPIGR, D458_I460del, S454_I460 > RQ, H448_Y465del, N455_S470del, K459_A469 > NLG, K459_A469 > NLGKPIGR, K459_P472 > NLGKPIGRRQASK, K459_R466 > NLG, K459_Y465 > K459_S470 > NLGKPIG, E457_F461del, D458_G462del, E418_F461del, V447_R466del, S451_I460del, E453_G484del, D414_R466del, N319_Y465del, K459_L474 > NLGKPIGRRQASP, K459_L471 > NLGKPIGRRQAS, K459_N480 > NLGKLK, K459_L481 > NLGKPIGRRQASP | ACA | None | N/A | N/A | Yes | Yes, docetaxel + platinum | Yes | N/A |
| 3 |
| F1921_V2171del, F2000_Q2164del, E2082_L2092 > LSIV | ACA | None | N/A | N/A | Yes | Yes, docetaxel | Yes | N/A |
| 4 |
| Y2543_I2550 > Q, K2547_K2551 > | ACA | Olaparib | 24 months | Yes | Yes | No | No | No |
| 5 |
| H2563_F2568 > LHC, E2565_G2569 > VV, E2565_T2575 > VVR | ACA | Olaparib | 10 months | Yes | Yes | No | No | Yes |
| 6 |
| F2560L, Q2561fs*87, H2563fs*5 | ACA | Olaparib | 9 months | Yes | Yes | Yes, docetaxel | No | Yes |
| 7 |
| I1418_S1770 > T, I1633_S1741del, C1675_S1848del, A1708_S1720del, D1709_A1725del | ACA | Olaparib | 6 months | No | Yes | Yes, docetaxel | No | Yes |
| 8 |
| K985_E1036del, E1035L, E1035S | ACA | Olaparib | 5 months | No | Yes | Yes, docetaxel | No | Yes |
| 9 |
| V2151_V2171del, S2156_Q2157delinsL | ACA | Olaparib | 13 months | Yes | Yes | Yes, docetaxel | No | Yes |
| 10 |
| P999_K1018 > QFQITVLEVASEQ | ACA | Olaparib | 22 months | Yes | Yes | No | Yes | Yes |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPARP inhibition in cancer therapy · Prostate Cancer Treatment and Research · Prostate Cancer Diagnosis and Treatment
Introduction
1
Pathogenic alterations in *BRCA1/2 (*collectively referred as BRCA) occur in up 5%–10% of prostate cancers (PCA), particularly in the metastatic castration‐resistance setting (mCRPC) [1, 2, 3, 4]. BRCA loss of function results in homologous recombination deficiency (HRD), which impairs DNA double‐strand break repair and renders tumor cells sensitive to poly(ADP‐ribose) polymerase inhibitors (PARPi) through a synthetic lethality mechanism [5, 6]. Based on multiple Phase III clinical trials, including PROfound, TRITON3, and TALAPRO‐2, the U.S. Food and Drug Administration (FDA) has approved PARPi agents, such as olaparib, rucaparib, niraparib and talazoparib, for the treatment of BRCA‐mutated, metastatic castration‐resistant PCA [7, 8, 9, 10, 11].
Despite an initial clinical benefit, resistance to PARPi almost inevitably develops. One of the most characterized resistance mechanisms involves BRCA1/2 reversion mutations (BRCArev), defined as secondary somatic alterations that restore the open reading frame or functional protein expression of a previously inactivating BRCA mutation [12, 13, 14]. These reversions restore homologous recombination repair proficiency and eliminate susceptibility to PARPi [12]. BRCArev most commonly arise as short insertions, deletions, or point mutations that correct the original inactivating defect, though larger rearrangements have also been described [15, 16].
In this context, primary PARPi resistance refers to the lack of initial clinical response or rapid progression despite adequate therapy exposure, whereas acquired (secondary) resistance denotes disease progression after an initial response [17]. While most BRCArev events are associated with acquired PARPi resistance under therapeutic selective pressure, emerging evidence indicates that DNA‐damaging agents such as platinum‐based chemotherapy or radiation may also induce BRCArev in the absence of prior PARPi exposure, potentially leading to primary PARPi resistance [14]. Notably, PCAs with homozygous, biallelic BRCA loss (complete gene deletion) [18] or HRD arising through irreversible mechanisms (e.g., epigenetic silencing due to promoter methylation or inactivating complex structural rearrangements) are less likely to acquire reversion mutations and may exhibit a more durable PARPi response [16, 18].
Although BRCArev have been extensively reported in ovarian, breast and pancreatic cancers [13, 14, 19], their clinical context and temporal evolution in PCA remain poorly understood. Prospective analyses from the TRITON2 study revealed the emergence of BRCArev in up to 40% of mCRPC patients at the time of PARPi progression [20], but systematic evaluation of BRCArev in PARP‐naïve PCAs is lacking. Moreover, the impact of prior cytotoxic therapy on the development of BRCArev and subsequent PARPi treatment duration remains unclear [20].
We hypothesized that BRCArev may emerge in advanced PCA prior to PARPi exposure, particularly following DNA‐damaging chemotherapy or radiotherapy, and that such events could confer primary resistance to PARPi. The objectives of this study were therefore to (i) determine the prevalence of BRCArev in a real‐world cohort of men with advanced BRCA‐mutated PCA, including in PARPi‐naïve patients; (ii) characterize the clinical and therapeutic contexts associated with BRCArev detection; and (iii) explore the relationship between prior cytotoxic chemotherapy and subsequent PARPi response duration. By integrating genomic and clinical data, this study aims to clarify how treatment chronology influences the emergence of BRCArev and the effectiveness of PARPi in advanced PCA.
Methods
2
Study Design and Cohort Selection
2.1
This retrospective, observational study included adult male patients (> 18 years) with a confirmed diagnosis of PCA. Approval of this study, including a waiver of informed consent and Health Insurance Portability and Accountability Act waiver of authorization, was obtained from the Western Institutional Review Board (Protocol No. 20152817). This study was performed in accordance with the principles of the Declaration of Helsinki. Men with advanced or metastatic PCA patients who underwent liquid‐based comprehensive genomic profiling (CGP) between January 1, 2023 and December 31, 2023 during clinical care across various institutions across North America using FoundationOneLiquid CDx (F1LCDx, Foundation Medicine Inc. Boston, MA) were retrospectively evaluated.
Liquid biopsy results were screened for the presence of pathogenic, inactivating BRCA1/2 alterations and corresponding secondary BRCArev alterations. Clinical and treatment histories were extracted from medical records and/or from treating oncologists' notes accompanying test requisitions. Cases without accompanying treatment history were excluded from the final BRCArev patient cohort.
Of 25 PCA patients in whom BRCArev identified during the study period, 15 were excluded due the lack of treatment histories, resulting in a final analytic cohort of 10 BRCArev patients with documented clinicopathologic data. Randomization and blinding were not applicable due to the retrospective observational design. Response or progression on PARPi was determined based on prostate‐specific antigen (PSA) dynamics (≥ 50% reduction or increase from baseline) and/or radiographic evidence of response or progression per treating physician assessment.
Liquid Biopsy Collection, Processing and Sequencing
2.2
Peripheral whole blood (2 × 8.5 mL) was collected into Streck Cell‐Free DNA BCT tubes as part of routine clinical care. Samples were shipped at ambient temperature and processed at Foundation Medicine's CLIA‐certified, CAP‐accredited, and New York State‐approved laboratory. Plasma was isolated via centrifugation and used for the extraction of circulating cell‐free DNA (cfDNA).
Library preparation and hybrid capture‐based next‐generation sequencing (NGS) were performed as previously described [21]. Briefly, cfDNA underwent end‐repair, A‐tailing, and ligation to barcoded sequencing adapters containing unique molecular identifiers (UMIs). Hybrid capture was conducted using a custom‐designed probe set targeting exonic regions of 324 cancer‐related genes, including BRCA1 and BRCA2, as well as select intronic regions frequently involved in genomic rearrangements. Captured libraries were sequenced on the Illumina NovaSeq platform to high uniform depth (median unique coverage > 5000×).
Sequencing data were analyzed using Foundation Medicine's proprietary bioinformatics pipeline to identify base substitutions, short insertions/deletions (indels), copy number alterations, and genomic rearrangements. Variant calling incorporated local realignment, read deduplication, and error suppression using UMIs to enhance sensitivity and specificity for low frequency variants. Tumor fraction (TF) was estimated using a combination of genome‐wide copy number modeling and variant allele frequency (VAF) distribution.
Identification of Pathogenic BRCA1/2 Alterations and Reversion Mutations
2.3
Pathogenic BRCA1 and BRCA2 alterations and corresponding BRCArev were detected using F1LCDx. Somatic versus germline origin predictions for pathogenic BRCA1/2 mutations were determined using a proprietary algorithm that integrates VAF, copy number modeling, and circulating tumor DNA tumor fraction (ctDNA TF). An alteration was classified as a BRCArev mutation if it was predicted to restore BRCA1/2 function by nullifying the effect of a pathogenic BRCA1/2 alteration. BRCArev detection is contingent upon the presence of a pathogenic BRCA1/2 alteration in the sample.
Initial BRCArev identification was performed using a computational algorithm that evaluates the presence of two BRCA variants and tests for six distinct reversion mechanisms: (1) pathogenic variant encompassed by an in‐frame deletion; (2) pathogenic variant replaced by a missense substitution; (3) frameshift pathogenic variant corrected by frame‐restoring indel; (4) exon containing a pathogenic variant predicted to undergo skipping due to splice site mutation; (5) pathogenic variant removed by an exon‐level deletion; and (6) biallelic deletion of the region containing the pathogenic variant. Following computational flagging, all candidate BRCArev events underwent manual review by scientists and molecular pathologists to confirm the biological plausibility and ensure final classification accuracy.
To exclude that BRCArev were derived from clonal hematopoiesis (CH), we applied the investigational short variant origin prediction (VOP) algorithm developed for the F1LCDx assay. This machine learning model incorporates fragmentomics and other sequencing features and was trained on liquid biopsy samples with matched‐depth sequencing of plasma and white blood cells. The algorithm outputs probabilistic origin classifications (germline, tumor‐somatic, or CH). A high‐confidence threshold (probability > 0.95) was used to designate CH origin and exclude such variants from the BRCArev cohort.
Results
3
Overall BRCArev Prostate Cancer Cohort
3.1
Between January and December 2023, a total of 416 men with PCA harbored a pathogenic BRCA1/2 alteration after undergoing blood‐based CGP via liquid biopsy (F1LCDx). Among these, 25 patients (6%) co‐harbored BRCA1/2 variants predicted to restore gene function (BRCArev). Of these, 10 patients (40%) patients had clinical and treatment histories available and were included in the final BRCArev analysis cohort.
Pathogenic alterations involved BRCA2 in 9 of 10 patients (90%) and BRCA1 in one patient (10%). Multiple BRCArev mutations were observed per sample in 9 of 10 patients (90%) (Table 1). All BRCArev events were classified as somatic and tumor‐derived, with no evidence of CH origin based on an investigational short variant VOP algorithm integrated into the F1LCDx pipeline.
Common co‐occurring alterations included AR (70%), TP53 (70%), TMPRSS2‐ERG fusion (60%) (Figure 1). None of the patients exhibited MSI‐H status or pathogenic alterations in POLE, SPOP, DNA mismatch repair genes (MSH2, MSH6, PMS2, MLH1) (Figure 1).
Oncoprint demonstrating co‐occurring alterations within liquid biopsies of 10 BRCA‐mutated patients with BRCArev. Each column represents one patient. Patients #1–3 are PARPi‐naïve. Patients #4–10 are PARPi‐treated. Black squares = truncating mutation; green squares = missense mutation; marron square = short variant inframe insertion; red rectangles = amplification; purple rectangles = fusion.
BRCArev mutations were detected in 3 of 10 patients who had not received prior PARP inhibitor (PARPi) therapy (PARPi‐naïve group) and in 7 of 10 patients (70%) with prior PARPi exposure (all olaparib) (Table 1). Subsequent analyses were stratified by treatment exposure history.
PARPi‐Naïve Patients With BRCA Reversion Mutations
3.2
Three patients (Table 1, Patients #1–3) exhibited somatic BRCArev in the absence of prior PARPi therapy. All three had previously received cytotoxic chemotherapy (platinum or docetaxel) and radiation before genomic testing. Radiation was directed to bone metastases in all three cases, and to primary tumor sites in two patients.
One patient (Patient 1) presented with de novo high‐stage small cell neuroendocrine carcinoma of the prostate without prior androgen deprivation therapy (Table 1). This diagnosis was supported by concurrent TP53 and RB1 alterations and absence of AR pathway resistance mutations (Figure 1). The other two patients (Patients 2 and 3, Table 1) had mCRPC, which was supported by the presence of AR resistance‐associated alterations (Figure 1).
Two of the three patients harbored pathogenic BRCA2 truncating variants (Table 1), T2542fs9 (Patient 1; VAF 45%) and L2092fs7 (Patient 3; VAF 52%), which were of predicted germline origin. The third patient (Patient 2) harbored a pathogenic BRCA1 K459fs*15 mutation (VAF 22%) of unknown germline status.
Multiple BRCA reversion mutations were identified per patient (n = 3, n = 37, and n = 3, respectively), all detected after chemotherapy and/or radiation exposure. The cumulative variant allele frequencies (VAF) of BRCArev in these patients were 1.6%, 9.5% and 8%, respectively, consistent with subclonal or polyclonal emergence of reversion events. A representative schematic of the primary pathogenic BRCA1 alteration and associated BRCArev variants from a PARPi‐naïve patient (Patient 2) is shown in Figure 2, and the patient's treatment timeline in Figure 3A.
Schematic of the primary pathogenic BRCA1 K459fs15 mutation and associated BRCA1 reversion mutations (n = 37) for one PARPi‐naïve prostate cancer patient (Patient 2). Blue bars denote amino acid span of BRCA1 reversion mutations.*
Treatment timelines for patients with PCA and BRCArev. (A) PARPi‐naïve patient (Patient 2). (B) PARPi‐treated patient with no prior chemotherapy or radiation (Patient 4). (C) PARPi‐treated patient with prior chemotherapy (Patient 7). ADT, androgen deprivation therapy; GS, Gleason score; IO, immunotherapy; RP, radical prostatectomy; SHT, secondary hormone therapy.
Patients With BRCA Reversion Mutations and Prior PARPi Exposure
3.3
Seven patients (Patients 4–10, Table 1) developed BRCArev following treatment with olaparib (300 mg, twice a day, by mouth). All seven harbored inactivating BRCA2 mutations as the primary pathogenic event: K2547fs4 (Patient 4; 2.3% VAF), E2565fs80 (Patient 5; 21.1% VAF), F2560fs5 (Patient 6; 38% VAF), Y1710fs1 (Patient 7; 87.5% VAF), E1035* (Patient #8; 49.8% VAF), Q2157fs18 (Patient 9; 50% VAF), and P999fs44 (Patient 10; 58.9% VAF). The latter four of these variants were predicted to be germline in origin. One patient (Patient 10) exhibited a single BRCArev mutation, while the remaining six patients displayed multiple independent reversion mutations (n = 3, 3, 3, 5, 3, 2 per case, respectively). The cumulative VAF percentage of BRCArev accross the seven patients ranged from 0.2% to 36.2% (median 14.3%), suggesting variable degrees of subclonal BRCA reversions within the ctDNA compartment.
All seven PARPi‐treated patients had mCRPC at the time of BRCArev detection (Table 1). Four of the seven (57%) had been previously pre‐treated with chemotherapy (all docetaxel) prior to PARPi initiation, and two had undergone prior radiation therapy (Table 1). The duration of PARPi treatment before detection of BRCArev ranged from 5 to 24 months.
Notably, the duration of PARPi response was shorter in patients with prior chemotherapy exposure compared with those who were chemo‐naïve (median 7.5 vs. 22 months, respectively Figure 4). Representative clinical timelines and molecular profiles for two illustrative PARPi‐treated patients, one chemotherapy‐naïve (Patient 4) and one chemotherapy‐pretreated (Patient 7) are shown in Figure 3B,C.
Swimmer plot of 7 BRCA‐mutated patients who developed BRCArev following PARPi (all olaparib) therapy. Duration of PARPi treatment was compared between patients that were pre‐treated with chemotherapy (all docetaxel) versus patients that received no prior chemotherapy before PARPi.
Discussion
4
Current guidelines recommend germline and/or somatic testing for homologous recombination gene mutations, including BRCA1 and BRCA2, in all patients with metastatic PCA to identify candidates for PARPi therapy [22]. In this study, we identified a subset of patients with BRCA‐mutated PCA who developed BRCA reversion mutations in the absence of PARPi therapy, suggesting that exposure to chemotherapy and/or radiation may induce or select for these reversions. These findings have potential implications for treatment sequencing and resistance mechanisms in advanced PCA.
Chemotherapy and Radiation as Potential Drivers of BRCA Reversion
4.1
Our analysis demonstrated that BRCA reversions were somatic and tumor‐derived, often emerging after exposure to platinum‐based or taxane chemotherapy and radiation. These reversions are predicted to abrogate the effect of the original, pathogenic BRCA 1/2 mutations and restore the open reading frame and BRCA1/2 protein function, consistent with mechanistic basis or PARPi resistance reported in ovarian, breast and PCAs [12]. Prior studies have established that BRCArev can restore homologous recombination proficiency and confer cross‐resistance to platinum and PARPi therapies [23, 24].
Notably, in the TRITON2 clinical trial, no baseline BRCArev was detected in any patient prior to PARPi treatment [20], likely because enrolled patients were platinum‐naïve. In contrast, our study observed baseline BRCArev in three PARPi‐naïve patients, all of whom had received chemotherapy and radiation [20]. This suggests that cytotoxic DNA‐damaging therapies may create selective pressure for BRCA reversion clones before PARPi exposure. Prior, rare case reports describing BRCArev emergence after platinum exposure but before PARPi therapy support this hypothesis [19, 25].
Implications for Treatment Sequencing and Clinical Practice
4.2
Our findings support the concept that earlier introduction of PARPi therapy, before chemotherapy, may preserve therapeutic sensitivity in patients with BRCA1/2‐mutated PCA. In our cohort, patients who were chemotherapy‐naïve prior to PARPi exhibited longer PARPi response durations than those pretreated with chemotherapy (median 22 vs. 7.5 months). This observation aligns with emerging evidence from the TRITON‐3 trial, in which a subset analysis demonstrated efficacy of rucaparib in BRCA‐mutated mCRPC before docetaxel chemotherapy [10]. Similarly, olaparib has shown durable activity in pre‐docetaxel mCRPC [11], and recent approvals of niraparib plus abiraterone and talazoparib plus enzalutamide provide additional options for earlier HRR‐targeted treatment [7, 8].
Collectively, these data suggest that PARPi use prior to cytotoxic chemotherapy may delay or prevent the emergence of BRCArev clones and improve therapeutic outcomes. Conversely, in heavily pre‐treated, PARPi‐naïve patients, screening for BRCArev before PARPi initiation could identify individuals at risk for primary PARPi resistance and guide alternative treatment strategies [25, 26].
Clinical and Translational Relevance of Liquid Biopsy
4.3
Liquid biopsy via peripheral blood offers a minimally invasive approach to detect BRCArev mutations and monitor clonal evolution in real time. This is particularly relevant in PCA, where bone‐predominant metastases often preclude repeat tissue sampling for molecular testing [27]. Circulating tumor DNA (ctDNA) assays, such as F1LCDx can capture temporal and spatial heterogeneity across metastatic sites, enabling clinicians to identify BRCA reversion mutations that emerge under therapeutic pressure [28]. As shown in our cohort, BRCArev often arise late in the disease course, potentially after multiple lines of therapy, highlighting the limitations of relying on archival tissue for molecular decision making.
Integrating ctDNA profiling into standard care could therefore improve treatment stratification, resistance monitoring, and clinical trial enrollment. For example, identifying BRCA reversions pre‐PARPi could redirect patients towards alternative therapies or combination trials targeting secondary resistance mechanisms.
Limitations and Future Directions
4.4
This study is limited by its retrospective design and small sample size, which constrain definitive statistical conclusions. Sequetial pre‐ and post‐treatment samples were not available to confirm the precise timing of BRCArev emergence. Nonetheless, the temporal association between chemotherapy/radiation and reversion detection, together with prior case‐based evidence, supports the plausibility of therapy‐induced reversion as a mechanism of PARPi resistance. Future prospective, longitudinal studies incorporating serial ctDNA testing before and after treatment are warranted to confirm these findings.
While novel therapeutic combinations (e.g., ATR, WEE1, USP1, or POLθ inhibitors) are under investigation to overcome PARPi resistance [29, 30, 31, 32, 33], such approaches remain experimental and were beyond the scope of our study. Their relevance may become more pronounced once BRCArev can be readily identified and longitudinally monitored in clinical practice.
Conclusions
4.5
In summary, our study provides evidence that BRCA reversions can arise in BRCA1/2‐mutated PCA in the absence of prior PARP inhibitor therapy, likely as an adaptive response to chemotherapy and/or radiation. These findings suggest that prior cytotoxic exposure may promote primary PARPi resistance and shorten subsequent treatment benefit. Early use of PARPi, before chemotherapy, may therefore optimize outcomes for patients with BRCA‐altered metastatic PCA.
Routine incorporation of liquid biopsy‐based BRCArev testing before and during therapy could refine patient selection, guide sequencing strategies, and enable real‐time monitoring of tumor evolution. Finally, enhanced clinician education and improved molecular report annotation, explicitly distinguishing BRCA‐sensitizing from BRCA resistance variants, are needed to ensure accurate interpretation and optimal use of precision oncology data in clinical care.
Author Contributions
Douglas I. Lin: conceptualization (equal), data curation (equal), formal analysis (equal), investigation (equal), project administration (equal), supervision (equal), visualization (equal), writing – original draft (equal), writing – review and editing (equal). Elizabeth Lawrence: data curation (equal), investigation (equal), project administration (equal), visualization (equal), writing – review and editing (equal). Natalie Danziger: data curation (equal), investigation (equal), visualization (equal), writing – review and editing (equal). Huihui Ye: investigation (equal), writing – review and editing (equal). Brennan Decker: investigation (equal), validation (equal), visualization (equal), writing – review and editing (equal). Ole Gjoerup: investigation (equal), resources (equal), writing – review and editing (equal). Ryon P. Graf: investigation (equal), writing – review and editing (equal). Jeffrey S. Ross: investigation (equal), supervision (equal), writing – review and editing (equal). Richard S. P. Huang: investigation (equal), writing – original draft (equal). Julia A. Elvin: investigation (equal), supervision (equal), writing – review and editing (equal). Douglas A. Mata: investigation (equal), supervision (equal), writing – review and editing (equal). Rana R. McKay: investigation (equal), writing – review and editing (equal).
Funding
The authors have nothing to report.
Ethics Statement
Approval for this study, including a waiver of informed consent and a Health Insurance Portability and Accountability Act waiver of authorization, was obtained from the Western Institutional Review Board, Protocol No. 20152817. The study was performed in accordance with the Declaration of Helsinki.
Conflicts of Interest
H.Y. and R.M. declare no conflicts of interest. At the time of the study, all remaining authors were full‐time employees of Foundation Medicine Inc. a whole subsidiary of Roche.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1C. C. Pritchard , J. Mateo , M. F. Walsh , et al., “Inherited DNA‐Repair Gene Mutations in Men With Metastatic Prostate Cancer,” New England Journal of Medicine 375 (2016): 443–453, 10.1056/NEJ Moa 1603144.27433846 PMC 4986616 · doi ↗ · pubmed ↗
- 2D. Robinson , E. M. Van Allen , Y. M. Wu , et al., “Integrative Clinical Genomics of Advanced Prostate Cancer,” Cell 161 (2015): 1215–1228.26000489 10.1016/j.cell.2015.05.001PMC 4484602 · doi ↗ · pubmed ↗
- 3W. Abida , J. Armenia , A. Gopalan , et al., “Prospective Genomic Profiling of Prostate Cancer Across Disease States Reveals Germline and Somatic Alterations That May Affect Clinical Decision Making,” JCO Precision Oncology 2017 (2017): 1–16.10.1200/PO.17.00029 PMC 555826328825054 · doi ↗ · pubmed ↗
- 4J. H. Chung , N. Dewal , E. Sokol , et al., “Prospective Comprehensive Genomic Profiling of Primary and Metastatic Prostate Tumors,” JCO Precision Oncology 3 (2019): 1–23.10.1200/PO.18.00283 PMC 658391531218271 · doi ↗ · pubmed ↗
- 5T. Helleday , “The Underlying Mechanism for the PARP and BRCA Synthetic Lethality: Clearing Up the Misunderstandings,” Molecular Oncology 5 (2011): 387–393.21821475 10.1016/j.molonc.2011.07.001PMC 5528309 · doi ↗ · pubmed ↗
- 6C. J. Lord and A. Ashworth , “PARP Inhibitors: Synthetic Lethality in the Clinic,” Science 355 (2017): 1152–1158.28302823 10.1126/science.aam 7344 PMC 6175050 · doi ↗ · pubmed ↗
- 7N. Agarwal , A. A. Azad , J. Carles , et al., “Talazoparib Plus Enzalutamide in Men With First‐Line Metastatic Castration‐Resistant Prostate Cancer (TALAPRO‐2): A Randomised, Placebo‐Controlled, Phase 3 Trial,” Lancet 402 (2023): 291–303.37285865 10.1016/S 0140-6736(23)01055-3 · doi ↗ · pubmed ↗
- 8K. N. Chi , D. Rathkopf , M. R. Smith , et al., “Niraparib and Abiraterone Acetate for Metastatic Castration‐Resistant Prostate Cancer,” Journal of Clinical Oncology 41 (2023): 3339–3351.36952634 10.1200/JCO.22.01649 PMC 10431499 · doi ↗ · pubmed ↗