Assessment of Electrolyte Imbalances as an Early Manifestation of Refeeding Syndrome in Critically Ill Patients Receiving Total Parenteral Nutrition at a Tertiary Hospital in Mexico City
Alejandro Martinez-Esteban, Sofía Peña-Solórzano, Erika Paola Sanchez-Saavedra, Miguel M Rojas-Evaristo, Victor M de la Puente-Diaz de Leon

TL;DR
This study examines how electrolyte imbalances in critically ill patients receiving total parenteral nutrition are linked to refeeding syndrome, emphasizing the importance of early detection.
Contribution
The study identifies specific electrolyte imbalances as early indicators of refeeding syndrome in TPN patients.
Findings
Hypokalemia, hypophosphatemia, and hypomagnesemia were observed in 37%, 36%, and 24% of patients, respectively.
The risk of refeeding syndrome increases with the number of electrolyte imbalances present.
Abstract
Introduction The nutritional status of critically ill patients is a key determinant of their clinical outcomes. Total parenteral nutrition (TPN) is an essential intervention when oral or enteral routes are not feasible, but it carries important risks such as hepatic and infectious complications, and particularly the development of refeeding syndrome (RFS), a potentially life-threatening condition associated with severe metabolic disturbances. Objectives The primary objective of the study was to determine the primary electrolyte imbalances associated with the development of RFS in critically ill patients receiving TPN. Secondary objectives were to determine the prevalence of RFS and evaluate the most effective prevention strategies in this population. Methods We conducted a retrospective descriptive study including critically ill hospitalized adults receiving TPN at Hospital Medica…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
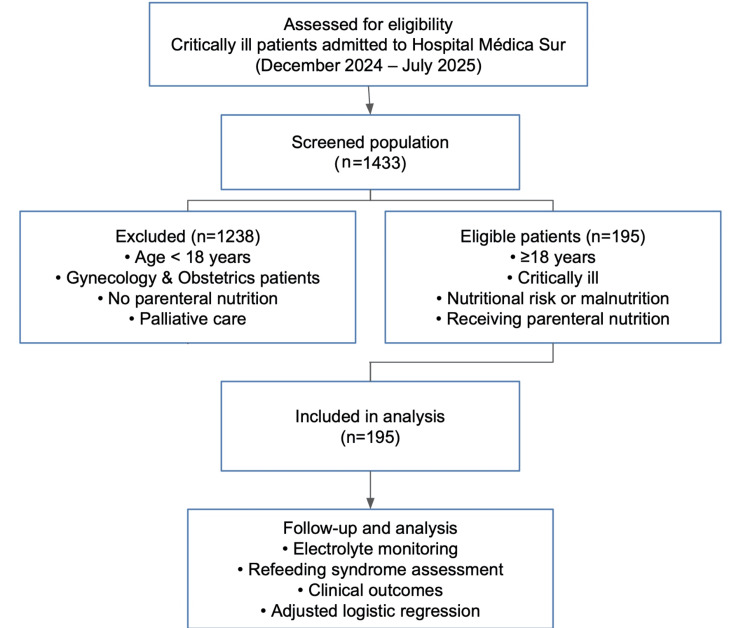 Figure 1
Figure 1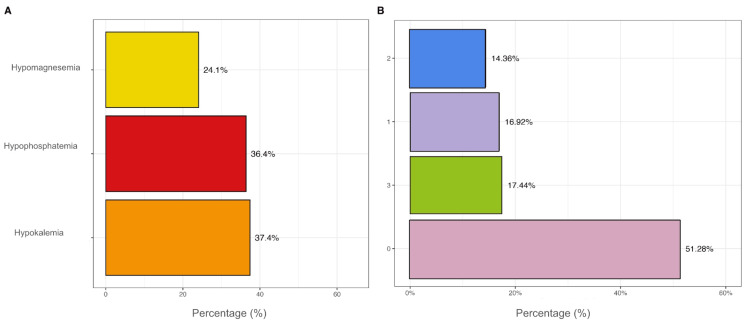 Figure 2
Figure 2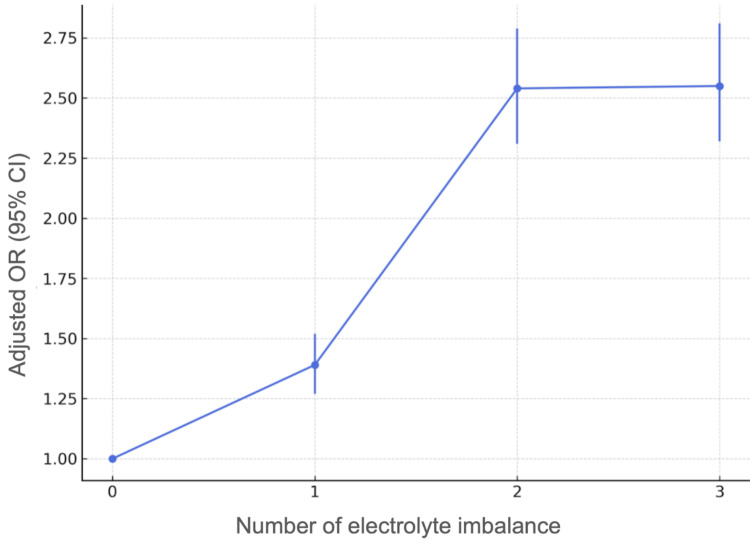 Figure 3
Figure 3| Parameter | Values |
| Age (years), median (IQR) | 67 (IQR: 52–76) |
| Sex, n (%) | |
| Male | 98 (50%) |
| Female | 97 (50%) |
| Weight (kg), median (IQR) | 65 (IQR: 57–74) |
| Height (meters), median (IQR) | 1.65 (IQR: 1.60, 1.73) |
| BMI (kg/m²), median (IQR) | 23.3 (IQR: 21.0–26.7) |
| Nutritional Classification, n (%) | |
| Malnutrition | 14 (7.2%) |
| Normal weight | 108 (55%) |
| Overweight | 55 (28%) |
| Obesity | 18 (9.2%) |
| Comorbidities | Frequency (Percentage) |
| Cardiopathies | 34 (17.4%) |
| Atrial fibrillation | 9 (4.6%) |
| Ischemic heart disease | 10 (5.1%) |
| Valvular heart disease | 1 (0.5%) |
| Heart failure | 6 (3.1%) |
| Others | 8 (4.1%) |
| Hepatic cirrhosis | 5 (2.6%) |
| Type 2 diabetes | 35 (18%) |
| Dyslipidemia | 22 (11%) |
| Thyroid disorders | 25 (13%) |
| Autoimmune diseases | 14 (7.2%) |
| Systemic lupus erythematosus | 1 (0.5%) |
| Rheumatoid arthritis | 6 (3.1%) |
| Coagulation disorders | 2 (1.0%) |
| Others | 5 (2.6%) |
| CKD | 9 (4.6%) |
| No CKD | 186 (95%) |
| Stage 3 | 5 (2.6%) |
| Stage 4 | 1 (0.5%) |
| Stage 5 | 3 (1.5%) |
| Neurological diseases | 17 (8.7%) |
| Ischemic stroke | 7 (3.6%) |
| Hemorrhagic stroke | 2 (1.0%) |
| Others | 8 (4.1%) |
| Oncologic disease | 76 (39%) |
| Pulmonary | 8 (4.1%) |
| Breast | 6 (3.1%) |
| Uterus and adnexa | 1 (0.5%) |
| Liver | 2 (1.0%) |
| Colon | 16 (8.2%) |
| Kidney | 1 (0.5%) |
| Pancreas | 12 (6.2%) |
| Hematologic | 9 (4.6%) |
| Prostate | 7 (3.6%) |
| Others | 36 (18%) |
| Hypertension | 59 (30%) |
| Pulmonary diseases | 13 (6.7%) |
| COPD | 6 (3.1%) |
| Asthma | 3 (1.5%) |
| Others | 4 (2.1%) |
| DVT/PE | 18 (9.2%) |
| Other comorbidities | 80 (41%) |
| Parameter | Value |
| Weight loss | 102 (52%) |
| Loss of Appetite | 133 (68%) |
| NRS-2002 (Points), median (IQR) | 5 (3, 5) |
| Nutritional risk, n (%) | |
| High | 140 (72%) |
| Moderate | 53 (27%) |
| Low | 2 (1.0%) |
| Days with TPN, median (IQR) | 8 (6, 14) |
| Indication for TPN, n (%) | |
| Fasting | 69 (35%) |
| Low enteral intake | 66 (34%) |
| Surgery | 50 (26%) |
| Malnutrition | 10 (5.1%) |
| Pre-formed TPN, n (%) | 96 (49%) |
| Caloric intake (kcal), median (IQR) | 1,135 (1,035–1,509) |
| Electrolyte imbalance, n (%) | |
| Hypophosphatemia | 71 (36%) |
| Hypokalemia | 73 (37%) |
| Hypomagnesemia | 47 (24%) |
| Any electrolyte imbalance | 95 (49%) |
| Cumulative number of electrolyte imbalance , n (%) | |
| 0 | 100 (51%) |
| 1 | 33 (17%) |
| 2 | 28 (14%) |
| 3 | 34 (17%) |
| Arrhythmias, n (%) | |
| Supraventricular tachycardia | 5 (2.6%) |
| Ventricular tachycardia | 1 (0.5%) |
| Atrioventricular block | 1 (0.5%) |
| Atrial fibrillation | 1 (0.5%) |
| Use of Multivitamin Solution | 96 (49.1%) |
| Clinical outcomes, n (%) | |
| Development of RFS | 73 (37%) |
| Clinical outcome, n (%) | |
| Death | 35 (18%) |
| Discharge | 160 (82%) |
| Hospital readmission | 43 (22%) |
| Parameter | Unadjusted Models | Adjusted Models | ||||
| OR | 95% CI | p value | OR | 95% CI | p value | |
| Hypophosphatemia | 2.34 | 2.17, 2.53 | <0.001 | 2.26 | 2.09, 2.45 | <0.001 |
| Hypokalemia | 2.04 | 1.85, 2.26 | <0.001 | 1.93 | 1.75, 2.14 | <0.001 |
| Hypomagnesemia | 1.98 | 1.75, 2.25 | <0.001 | 1.83 | 1.61, 2.10 | <0.001 |
| Any electrolyte imbalance | 2.11 | 1.94, 2.30 | <0.001 | 2.02 | 1.85, 2.20 | <0.001 |
| Cumulative number of electrolyte imbalances | ||||||
| 0 | Ref | — | Ref | — | ||
| 1 | 1.38 | 1.27, 1.51 | <0.001 | 1.39 | 1.27, 1.52 | <0.001 |
| 2 | 2.60 | 2.37, 2.85 | <0.001 | 2.54 | 2.31, 2.79 | <0.001 |
| 3 | 2.69 | 2.47, 2.93 | <0.001 | 2.55 | 2.32, 2.81 | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClinical Nutrition and Gastroenterology · Nutrition and Health in Aging · Infant Nutrition and Health
Introduction
The nutritional status of an individual is a multifactorial concept encompassing factors such as caloric intake, absorption, nutrient utilization, body composition, and overall health. Thus, there is a need to determine inadequate or excessive intakes to design interventions that improve health and prevent diet-related diseases [1].
The Nutritional Risk Screening-2002 (NRS-2002) is a nutritional assessment system used to identify patients at risk of malnutrition who may require dietary or nutritional interventions. [1,2]. It evaluates three main components: weight loss, body mass index (BMI), and food intake. A higher score indicates greater nutritional risk and the need for intervention [2].
Total parenteral nutrition (TPN) refers to the administration of dextrose, lipids, amino acids, electrolytes, vitamins, minerals, and trace elements via intravenous parenteral route [3-5]. It is a lifesaving intervention for patients who are unable to receive oral or enteral nutrition. Despite its benefits, this treatment is costly and carries a risk of hepatobiliary, infectious, and electrolyte complications [6-8].
In general, half of the daily requirements are administered on the first day and, if tolerated without uncontrolled hyperglycemia, sudden electrolyte changes, or lipid abnormalities, the full target is reached on the second day [9-11]. TPN must be prescribed daily due to the potential for shifting electrolyte imbalances. In general, oral feeding is preferred over enteral or parenteral support; however, patient comorbidities may affect this decision. In the intensive care unit (ICU), most patients are unable to receive enteral feeding due to comorbidities, clinical condition, and other causes, primarily related to alterations in gastrointestinal function [12-14].
Refeeding syndrome (RFS) is a potentially life-threatening condition resulting from rapid shifts in fluids and electrolytes when malnourished patients receive oral, enteral nutrition, or TPN [15]. The first cases were reported in the 1940s, when a series of World War II prisoners suffering from severe malnutrition were found to develop cardiovascular and neurological manifestations after they had been repleted with nutrients following prolonged starvation [16]. The first systematic review addressing refeeding syndrome was published by Friedli et al. in March 2017, focusing on its definition and the development of preventive and treatment strategies. It is considered a life-threatening condition that involves severe metabolic abnormalities, such as impaired glucose metabolism, electrolyte imbalances (hypophosphatemia, hypokalemia, hypomagnesemia), and thiamine deficiency [17]. The primary aim of this study was to determine the primary electrolyte imbalances associated with the development of RFS in critically ill patients receiving TPN.
Materials and methods
This was a retrospective descriptive study conducted at Hospital Medica Sur, Mexico City, Mexico, from December 2024 to July 2025. Every individual admitted as a patient to the hospital signed a privacy notice authorizing the use of their data for research purposes. The study was approved by the Research Ethics Committee of Médica Sur (approval number: 2024-EXT-922).
Objectives
The primary objective of the study was to determine the primary electrolyte imbalances associated with the development of RFS in critically ill patients receiving TPN. Secondary objectives were to determine the prevalence of RFS and evaluate the most effective prevention strategies in this population
Study population
The study inclusion criteria were adult patients over 18 years of age hospitalized in critical condition and at risk of malnutrition. The exclusion criteria were patients hospitalized in the Gynecology and Obstetrics area, patients in palliative care, and any other patient who did not require TPN.
The study population consisted of 1433 critically ill adult patients hospitalized at the hospital. Of these, 1238 patients were excluded for not meeting the inclusion criteria, and 195 patients who met all the criteria were included in the final cohort (n = 195). Data were obtained from medical records and electronic health records with clinical and laboratory follow-up within seven days after the start of TPN. The reference range for laboratory values for electrolyte imbalances comes from the ranges established by the laboratory and Clinical Pathology service of the hospital. Figure 1 shows the flow chart for the selection of participants.
Cohort flow diagram of patient selection and inclusion in the studyPatient eligibility was assessed, and data were acquired from 1433 critically ill adult patients admitted to the hospital between December 2024 and July 2025. Of these, 1238 patients were excluded, and 195 patients who met all criteria were included in the final cohort. The presence of electrolyte imbalances and the occurrence of refeeding syndrome were assessed, and the results were analyzed using adjusted logistic regression models.
Data collection
The independent variables considered in the study include: sex (female and male), age (years), reason for admission to ICU (shock, desaturation, bleeding, etc.), comorbidities (pre-existing conditions), and severity criteria (low, high, very high risk). The dependent variables are: electrolyte imbalance (hypophosphatemia, hypokalemia, and hypomagnesemia), diagnosis of RFS according to the NICE Criteria Guidelines [18] (yes or no), and clinical outcomes. The information was collected directly from clinical records and organized in a database designed specifically for this study.
Data analysis
The clinical and laboratory evolution of the patients was evaluated within the first seven days, documenting the development of RFS, the interventions performed to prevent its progression, and each patient's outcome. This information allowed the identification of modifiable risk factors and the strengthening of strategies for the prevention and timely management of RFS in critically ill patients.
Quantitative variables were summarized by the median (interquartile range (IQR)), and qualitative variables by frequencies and percentages. All analyses were conducted using R statistical software version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria, https://www.R-project.org/). A value of P < 0.05 was considered to be statistically significant. To evaluate the association between electrolyte imbalances (hypophosphatemia, < 3.2 mg/dL, reference interval: 3.2-4.6 mg/dL; hypokalemia, < 3.9 mg/dL, reference interval: 3.9-5.3 mg/dL; hypomagnesemia, < 1.8 mg/dL, reference interval: 1.8-2.5 mg/dL) and the development of RFS according to the NICE Criteria Guidelines [18].
Given that one of the primary dependent variables was binary (presence or absence of electrolyte imbalance), a logistic regression analysis was performed to identify factors that increase or decrease the probability that a patient at risk will develop an electrolyte imbalance during TPN administration. Binary logistic regressions were performed, adjusted for the following confounding variables: age, sex, BMI, significant weight loss, NRS-2002 score, duration of TPN, and nutritional risk.
Results
A total of 195 patients with severe illness were recruited from December 2024 to July 2025; 50% of the patients were men (n = 98) and 50% women (n = 97), with a median age of 67 years (IQR: 52-76) (Table 1); thus representing mainly older adults, a patient category prone to comorbidities, and in-hospital nutritional decline. Regarding anthropometric characteristics, the median weight was 65 kg (IQR: 57-74), and the BMI was 23.3 kg/m² (IQR: 21.0-26.7). When classifying patients according to BMI, most were within the normal weight range at 55% (n = 108), followed by overweight at 28% (n = 55), obesity at 9% (n = 18), and malnutrition at 7% (n = 14). This result is interesting, as there may be nutritional deficiencies in the obese patient.
Table 2 shows the associated comorbidities. Hypertension was the most prevalent at 30% (n = 59), followed by type 2 diabetes at 18% (n = 35), thyroid disorders at 13% (n = 25), and dyslipidemia at 11% (n = 22). CKD was identified in 4.6% of patients (n = 9), most frequently in the. advanced stages of CKD (Grade 3-5). Various cardiovascular histories were noted, including atrial fibrillation (4.6%, n = 9) and ischemic heart disease (5.1%, n = 10), as well as several pulmonary conditions, mainly chronic obstructive pulmonary disease (COPD) (3.1%, n = 6). Liver cirrhosis was documented in 2.6% of patients (n = 5). Any oncologic disease was reported in 39% of patients (n = 76), predominantly colon cancer (8.2%, n = 16), lung cancer (4.1%, n = 8), pancreatic cancer (6.2%, n = 12), and hematologic malignancies (4.6%, n = 9). Other comorbidities included deep vein thrombosis (DVT) and pulmonary embolism (PE) in 9.2% of patients (n = 18) and autoimmune diseases, the most frequent being rheumatoid arthritis at 4% (n = 8). Up to 41% of the sample (n = 80) reported other comorbidities, including osteoporosis, benign prostatic hyperplasia, gout, gastroesophageal reflux disease, peptic ulcer disease, and irritable bowel syndrome.
Upon admission to the hospital, more than half of the patients (52%, n = 102) reported significant weight loss, while 68% (n = 133) presented with loss of appetite. The median score on the NRS 2002 scale was 5.0 (IQR: 3.0-5.0), classifying 72% (n = 140) as being at high nutritional risk. The high prevalence of malnutrition in patients with obesity highlights the importance of systematic nutritional assessment upon hospital admission for the assessment of nutritional risk using the NRS 2002 score (Table 3). The median duration of TPN (personalized or pre-formed) was eight days (IQR: 6-14). The main indications for initiating TPN were prolonged fasting (35%, n = 69), low enteral intake (34%, n = 66), and during the postoperative period (26%, n = 50). Almost half of the patients (49%, n = 96) received commercial pre-formed TPN with a median caloric intake of 1135 kcal (IQR: 1035-1509).
The reported prevalence of electrolyte imbalances was high. Hypokalemia was documented in 37% of the study population (n = 73), hypophosphatemia in 36% (n = 71), and hypomagnesemia in 24% (n = 47) (Figure 2A). Regarding the cumulative number of disorders, 1/3 of patients had more than one imbalance, while 51.3% (n = 100) showed no manifestations. The concurrence of all three disorders affected 17.4% (n = 34) (Figure 2B).
Presentation of electrolyte imbalancesThis figure describes the most common electrolyte imbalances (yellow: hypomagnesemia, red: hypophosphatemia and orange: hypokalemia) (2A), as well as the total electrolyte imbalances presented in the study (purple: 1 imbalance, blue: 2 imbalances, green: three imbalances, pink: no imbalance) (2B).
Arrhythmias were rare, occurring in only 4.1% (n = 8) of patients. The study identified the use of commercial multivitamin solution in 49.1% (n=96). Finally, regarding clinical outcomes, 37% (n = 73) developed RFS, 18% (n = 35) died during hospitalization, and 22% (n = 43) were readmitted after discharge.
The development of the three electrolyte imbalances was statistically significantly associated with a higher probability of presenting RFS. In the adjusted models, hypophosphatemia increased this probability by 2.26 times (95% CI: 2.09-2.45), hypokalemia by 1.93 times (95% CI: 1.75-2.14), and hypomagnesemia by 1.83 times (95% CI: 1.61-2.10). The presence of any imbalance doubled the risk of developing this syndrome (OR = 2.02; 95% CI: 1.85-2.20) (Table 4). In addition, a dose-response relationship was evident, as compared to patients without alterations, the risk of RFS increased progressively with the presence of one (OR = 1.39, 95% CI: 1.27-1.52), two (OR = 2.54, 95% CI: 2.31-2.79), and three imbalances (OR = 2.55, 95% CI: 2.32-2.81) (Figure 3).
Increased risk of RFS with the number of electrolyte imbalances developedRFS: refeeding syndrome
Discussion
Due to the lack of a precise definition, the true prevalence of RFS is not described in most published studies, and only focuses on hypophosphatemia [19]. Reported prevalence varies from 0-2% to 50-80% in systematic reviews and other case series [20]. Malnourished patients have a higher risk of hypophosphatemia, with mortality rates as high as 18.2% in severe cases, compared to 4.6% in those without malnutrition. Critically ill patients receiving TPN for ≥48 hours have a 34% probability of developing hypophosphatemia [21].
Patients with prolonged periods of minimal or no nutritional intake related to critical illness or major surgery are at high risk of developing RFS. The NICE criteria provide guidance on clinical nutritional status for critically ill and chronically ill populations at high risk for RFS [18,22]. Continuous monitoring is essential to identify early signs and symptoms of this condition, such as hypophosphatemia, hypokalemia, hypomagnesemia, selenium deficiency, glucose abnormalities, neurological changes such as delirium or seizures, arrhythmias, heart failure, and respiratory failure [23-25].
In this study, a total of 195 patients were included and analyzed during their stay in the ICU with TPN. The results obtained show a high prevalence of electrolyte imbalances, particularly hypokalemia (37%), hypophosphatemia (36%), and hypomagnesemia (24%). It is noteworthy that 37% of the patients developed RFS, a figure considerably higher than that reported in the pre-existing literature. This could be attributed to the specific clinical profile of the studied population, as well as to comorbidities and metabolic conditions prior to the initiation of TPN. Furthermore, it is important to mention that the severity of RFS in most patients did not have a significant clinical impact or produce serious complications and did not have an associated fatal outcome; in fact, the cause of death was due to other factors.
The most significant finding was a clear dose-response relationship between the cumulative number of electrolyte imbalances and the risk of developing RFS, with a progressive, statistically significant increase in risk. This finding suggests that not only does the presence of hypophosphatemia, hypokalemia, or hypomagnesemia alone represent a considerable risk, but their combination increases the likelihood of triggering RFS. This shows that having pot-TPN administration three or more associated imbalances doubles the risk, even after performing the corresponding multivariable adjustment. This reinforces the importance of close monitoring of electrolyte changes as a prevention strategy. In addition, the use of personalized supplemental nutrition can modify the development of RFS, as it is adapted to the needs of each patient and the underlying condition that led to their hospitalization, along with close monitoring in the ICU [15].
The study results are consistent with those reported in the literature by Friedli et al., which highlight hypophosphatemia as the sentinel marker of RFS [17]. However, the cumulative effect of multiple alterations on the development of RFS has not been specifically reported, which can be considered a highly relevant contribution of the present study. On the other hand, the high prevalence of nutritional risk (72% with NRS ≥5) coincides with previous findings in hospital populations, highlighting the need to strengthen and standardize systematic nutritional screening upon hospital admission, as well as continuous reassessment during their stay [1,2].
Early identification of electrolyte imbalances as a manifestation of RFS should be a priority in the ICU, since early diagnosis and preventive measures can prevent fatal complications such as arrhythmias or death. Furthermore, medical staff should be trained on this topic to raise awareness and incorporate an active monitoring plan to asses metabolic and biochemical safety of nutritional support. Likewise, reinforcing the routine use of supplemental regimens should be considered part of the primary strategies in these patients [15,18].
Regarding the study's limitations, it is important to note that it is a single-center study, which may limit the generalizability of the results. Furthermore, although multivariate adjustment was performed during the statistical analysis, variables related to liver function or nitrogen balance that could influence the occurrence of liver-related syndrome (LRS) were not included; also, by identifying frequent use of preformed TPN presentations, it provides variability due to the multiple presentations available and used in the hospital and there was also no objective and measurable assessment of sarcopenia, even though it is a very common nutritional condition in these patients. However, the inclusion of all available cases with well-defined inclusion criteria, as well as the analysis performed, strengthens the study's internal validity.
Finally, the study not only reinforces what has been described in the literature, but also proposes and expands clinical knowledge by demonstrating the cumulative effect of electrolyte imbalances in this condition. This highlights the urgent need to incorporate clinical protocols for screening and proactive prevention from the first 24-28 hours of nutritional support, as suggested by the guidelines of the American Society for Parenteral and Enteral Nutrition (ASPEN) [3] and the European Society for Clinical Nutrition and Metabolism (ESPEN) [7].
This original research provides concrete and scientifically rigorous evidence that supports institutional changes in nutritional support practices in other ICUs. Currently, there is no research in Mexico on this condition, and this study also raises new questions for future research, such as the role of other biomarkers such as albumin and pre-albumin, transferrin, C-reactive protein, and interleukins in the diagnosis and management of RFS.
Conclusions
RFS is a common complication in critically ill patients receiving TPN. The presence of electrolyte imbalances is directly and significantly associated with the development of this syndrome, so identifying them early allows the establishment of preventive interventions to reduce morbidity and mortality associated with this nutritional support.
The findings of this study reinforce the need to implement a systematic, standardized nutritional assessment for all hospitalized patients and to monitor TPN administration closely to reduce associated morbidity and mortality. The identification of the RFS should be mandatory and is a standard of quality of care in the ICU, as well as an indicator of safety and clinical excellence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials Clin Nutr Kondrup J Rasmussen HH Hamberg O Stanga Z 3213362220031276567310.1016/s 0261-5614(02)00214-5 · doi ↗ · pubmed ↗
- 2Educational and Clinical Practice Committee, European Society of Parenteral and Enteral Nutrition (ESPEN). ESPEN guidelines for nutrition screening 2002 Clin Nutr Kondrup J Allison SP Elia M Vellas B Plauth M 4154212220031288061010.1016/s 0261-5614(03)00098-0 · doi ↗ · pubmed ↗
- 3A.S.P.E.N. parenteral nutrition safety consensus recommendations JPEN J Parenter Enteral Nutr Ayers P Adams S Boullata J 2963333820142428012910.1177/0148607113511992 · doi ↗ · pubmed ↗
- 4A.S.P.E.N. clinical guidelines: parenteral nutrition ordering, order review, compounding, labeling, and dispensing JPEN J Parenter Enteral Nutr Boullata JI Gilbert K Sacks G 3343773820142453170810.1177/0148607114521833 · doi ↗ · pubmed ↗
- 5Standardized competencies for parenteral nutrition prescribing: the American Society for Parenteral and Enteral Nutrition Model Nutr Clin Pract Guenter P Boullata JI Ayers P 5705763020152607828810.1177/0884533615591167 · doi ↗ · pubmed ↗
- 6Parenteral nutrition overview Nutrients Berlana D 44801420223636474310.3390/nu 14214480 PMC 9659055 · doi ↗ · pubmed ↗
- 7ESPEN practical guideline: clinical nutrition in chronic intestinal failure Clin Nutr Cuerda C Pironi L Arends J 519652204020213447917910.1016/j.clnu.2021.07.002 · doi ↗ · pubmed ↗
- 8ESPEN practical guideline: clinical nutrition in surgery Clin Nutr Weimann A Braga M Carli F 474547614020213424291510.1016/j.clnu.2021.03.031 · doi ↗ · pubmed ↗