Real-world efficacy of long-term teduglutide use in pediatric patients with short bowel syndrome
Claire Josey, George Mazariegos, Elizabeth King, Pamela Holzer, Jeffrey Rudolph, Vikram Kalathur Raghu

TL;DR
Teduglutide helps reduce the need for parenteral support in children with short bowel syndrome, showing real-world effectiveness over long-term use.
Contribution
This study provides real-world evidence of teduglutide's long-term efficacy in reducing parenteral support dependency in pediatric short bowel syndrome patients.
Findings
67% of patients experienced a ≥20% reduction in parenteral support volume.
30% of patients achieved enteral autonomy within a mean of 71.57 weeks.
Significant decreases in parenteral nutrition metrics were observed.
Abstract
In patients with short bowel syndrome (SBS), teduglutide reduces dependency on parenteral support (PS) by promoting intestinal growth and absorption. We aim to describe long-term outcomes using teduglutide in a large pediatric intestinal rehabilitation and transplant center. We performed a single-center, retrospective analysis of teduglutide use in patients with SBS ages 1–23 years. Sex, age, intestinal length, BMI, PS regimens, and isolated small bowel (ISB) transplant status are described. Subgroup analysis comparing younger and older patient cohorts was performed. Primary end point was a reduction in PS volume of ≥ 20 %. 27 patients (10 female; mean age 8.9 years) received subcutaneous teduglutide (0.05 mg/kg/d) once daily for mean 120.8 weeks. Mean bowel length was 56.9 (SD=52.1) cm. 5 were listed for ISB transplant, 2 were “inactive,” and 20 were not listed. 2 patients were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
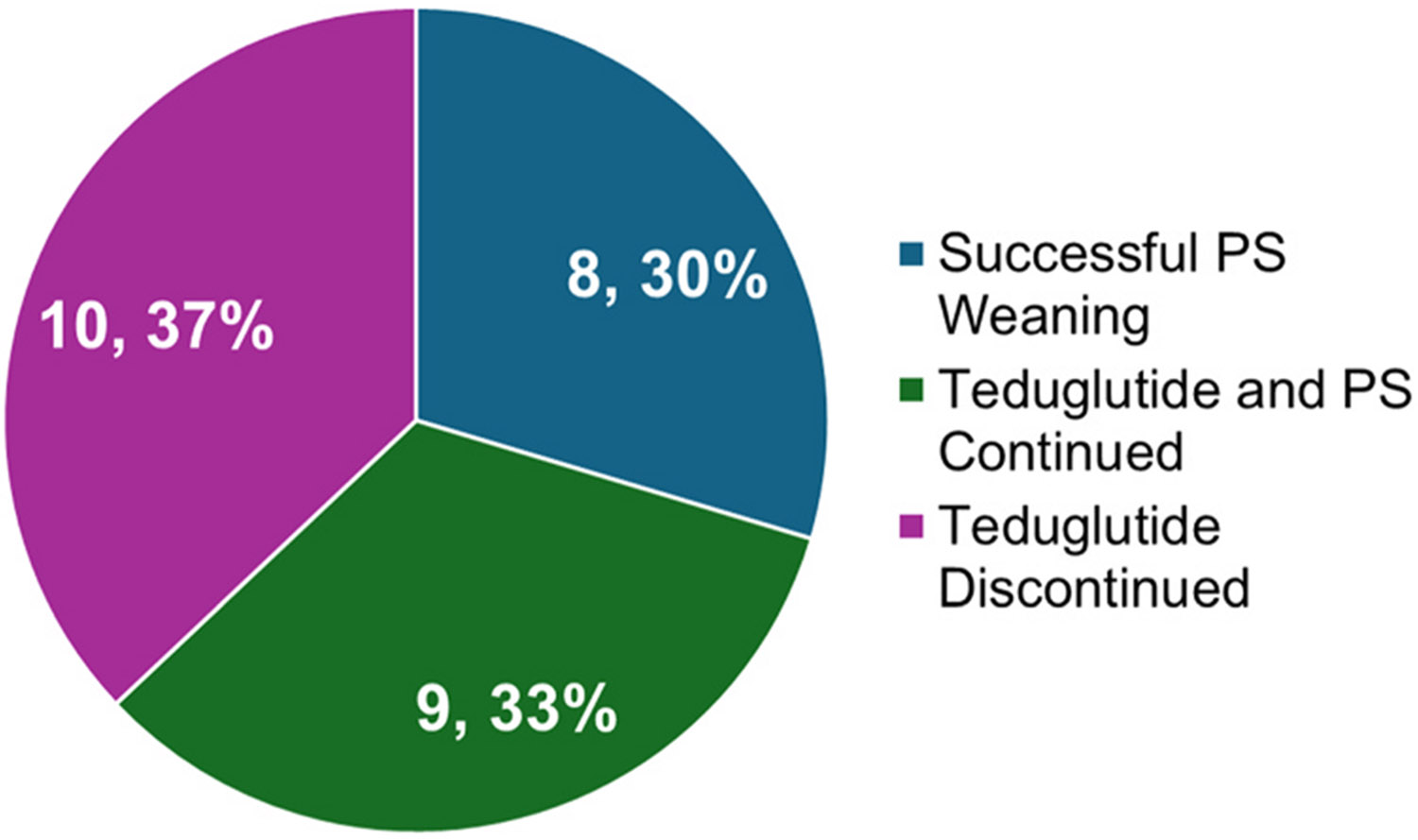 Figure 1
Figure 1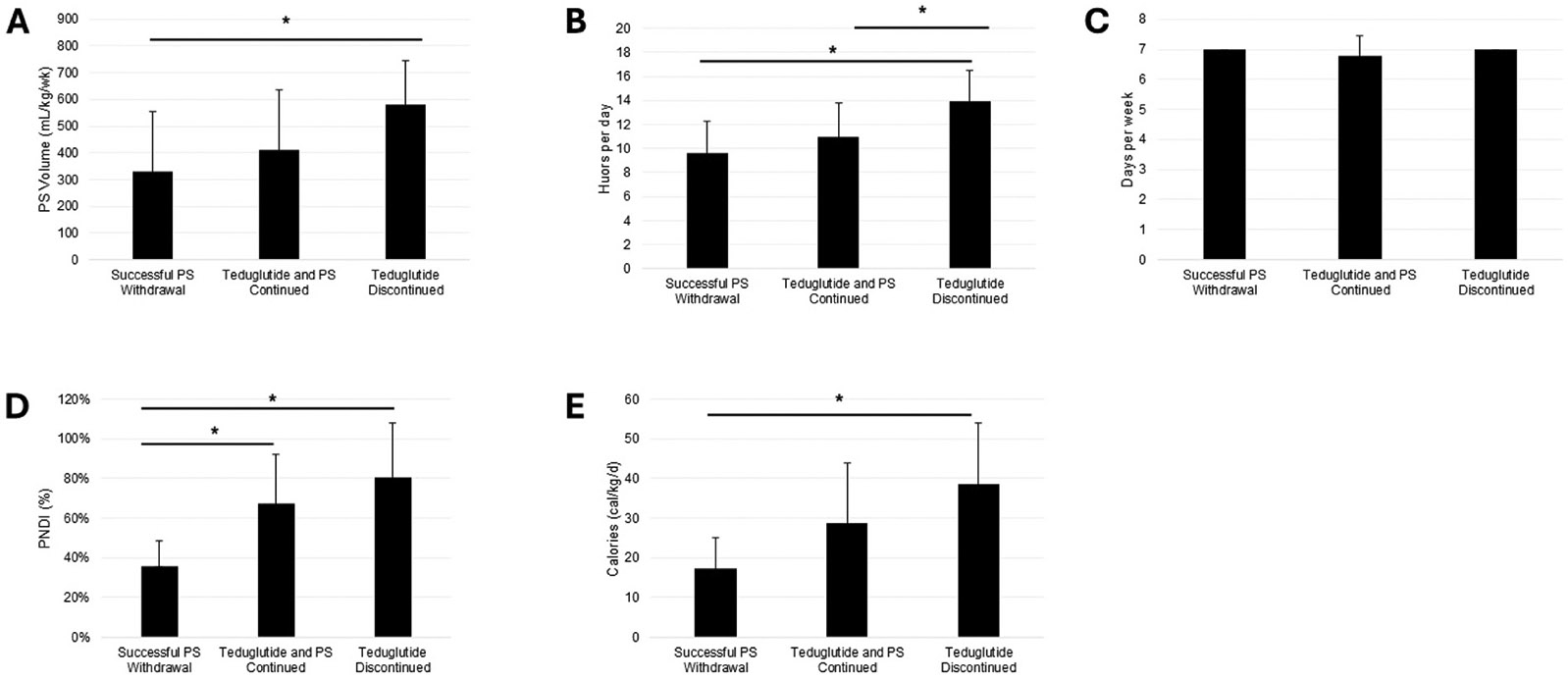 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClinical Nutrition and Gastroenterology · Gastroesophageal reflux and treatments · Pediatric Hepatobiliary Diseases and Treatments
Introduction
Short bowel syndrome (SBS) results from surgical resection or congenital defects and the subsequent loss of absorption, frequently necessitating dependency on parenteral support. Treatments which increase intestinal absorption present the opportunity to minimize dependency on parenteral support.
Glucagon-like peptide-2 (GLP-2) is a naturally-occurring hormone secreted by intestinal cells during digestion. GLP-2 promotes epithelial proliferation and intestinal surface area. [1,2] Administration of teduglutide, a GLP-2 analog, enhances villous height and crypt depth and aims to reduce dependency on parenteral nutrition. [2] Teduglutide is approved for the treatment of pediatric patients with SBS with parenteral support dependency in North America, Europe, and Japan. [3] A pooled analysis of two open-label phase 3 studies investigating the efficacy and safety of teduglutide in 78 children with SBS found that 82 % of patients achieved a significant clinical response, defined as a 20 % reduction in parenteral nutrition or intravenous volume. 22 % of these patients achieved enteral autonomy at 96 weeks.
This report describes the real-world experiences of pediatric patients receiving long-term teduglutide treatments. This large pediatric intestinal rehabilitation and transplant center did not participate in clinical trials for teduglutide. Additionally, this study aims to identify factors that are predictive of treatment success or failure, which will contribute to clinical decision-making regarding the initiation and withdrawal of teduglutide treatment.
Material and Methods
We performed a retrospective, cross-sectional study of teduglutide use in children with SBS at a single center. The center’s intestinal rehabilitation team includes three providers who make independent clinical decisions and share patient caseloads. There is no formal protocol utilized for weaning PS; decisions including initiating and discontinuing teduglutide treatment are discussed in weekly conferences consisting of physicians, surgeons, nurses, and social workers.
Patient population
Inclusion criteria included a) past or current patients, b) diagnosis of SBS, c) documented dependency on parenteral support, including total parenteral nutrition (TPN) and/or IV fluids, and d) daily injections of teduglutide for at least three weeks.
Patients were excluded on the basis of noncompliance, use of teduglutide for less than three weeks, or a lack of documented dependency on parenteral support.
A retrospective chart review was conducted on the final cohort. Eligibility for teduglutide was determined through a safety assessment which included a colonoscopy.
Data collection
Demographic and clinical data were obtained from the electronic medical record system. Baseline characteristics included age, sex, BMI, SBS etiology, presence of a stoma, small bowel length, PS dependency, and isolated small bowel (ISB) transplant status. Dependency on PS was measured through combined parenteral nutrition (PN) and IV fluid volume (mL/kg/wk), days per week, hours per day, caloric intake (cal/kg/d), parenteral nutrition dependency index (PNDI), and lipid dose (g/kg/d).
PNDI is the ratio between non-protein energy intake (NPEI), or energy provided by parenteral nutrition, and resting energy expenditure (REE), estimated using the Schofield equation. PNDI serves as an indirect measure of intestinal absorption. PS dependency can be classified as “mild” (PNDI <80 %), “high” (80–120 %), or “very high” (>120 %). [4]
PS dependency was recorded at initiation of teduglutide therapy and at most recent clinical visit or at time of teduglutide discontinuation, if applicable. The primary end point was a reduction in PS volume of 20–100 %. Secondary end points included changes in days receiving PS, hours receiving PS, PNDI, PS nonprotein calories, and lipid dose. Subgroup analysis comparing patients below and above age 5 at baseline was also performed.
Statistical analysis
Descriptive statistics were used to characterize patients. Continuous variables were reported as mean with standard deviation (SD).
Results
Patient characteristics
We identified 32 patients of both sexes ages 1–23 years who received teduglutide for treatment of SBS between 8/2019 and 12/2024. Exclusion of patients due to noncompliance (n = 2), lost to follow-up (n = 2), and no documented PS dependency at baseline (n = 1) was conducted. Adverse events were reported on all patients and classified as “serious” if they resulted in hospitalization. The relatedness of adverse events was determined through clinician input found in medical records.
A final cohort of 27 patients were identified. Baseline characteristics were collected and summarized in Table 1. Mean age at baseline was 8.90 (SD=5.22) years. The most common SBS etiologies included gastroschisis (37 %), necrotizing enterocolitis (26 %), volvulus (11 %), and Hirschsprung’s Disease (11 %). A stoma was present for 15 % of patients. Mean small bowel length was 56.9 (SD=52.1) cm. Mean continuous period of PS dependence prior to teduglutide initiation was 3.70 (SD=3.10) years. 5 were listed for ISB transplant, 2 were “inactive,” and 20 were not listed. 2 patients were post-enterectomy. Patients received teduglutide for mean 120.8 (SD=80.7) weeks.
Efficacy
Primary end point
The primary end point was a reduction in PS volume of 20–100 %. 18 patients (67 %) achieved this end point, with 8 patients (30 %) successfully weaning from PS completely.
Secondary end points
Secondary end points included a significant reduction in PS volume (−150.82 mL/kg/wk, p = 0.0087), hours/day receiving PS (−3.37 h, p = 0.0014), days/week receiving PS (−2.22 days, p = 0.0013), nonprotein calories received through PS (−8.78 cal/kg/d, p = 0.0022), PNDI (−19.67 %, p = 0.0016), and lipid dose (−0.34 g/kg/d, p = 0.0495). Indicators of treatment response at baseline and final follow up are detailed in Table 2.
Of the 5 patients listed for ISB transplant at baseline, 2 remained listed, 2 were removed, and 1 was reclassified as “inactive.” 1 was newly listed and 2 “inactive” patients were removed. 19 patients remained unlisted. The 2 patients who received teduglutide post-enterectomy experienced significant decreases in PS volume (46.5 % and 43.7 %).
Successful PS weaning
patients (30 %) successfully weaned to intravenous fluids at mean 45.35 (SD=59.28) weeks and achieved enteral autonomy at mean 71.57 (SD=56.37) weeks. At teduglutide initiation, these patients had a significantly lower PS volume (p = 0.0150), PS hours per day (p = 0.0032), PNDI (p = 0.0006), PS nonprotein calories (p = 0.0027), and PS lipid dose (p = 0.0017) at baseline than patients who ultimately discontinued teduglutide treatment (Figs. 1 and 2). Characteristics of these patients are described in Table 3.
BMI did not change significantly between baseline, PS withdrawal, and most recent clinic visit at mean 181.95 (SD=63.31) weeks.
Teduglutide and PS continued
patients (33 %) continued teduglutide treatment without complete PS withdrawal at mean 131.30 (SD=83.07) weeks after teduglutide initiation. These patients experienced a significant reduction in the number of hours per day receiving PS (−2 h, p = 0.0039) and in lipid dose (−0.69 g/kg/d, p = 0.0345). No patients discontinued lipids. 5 patients (56 %) achieved a significant reduction in PS volume of ≥ 20 %. BMI did not change significantly from baseline (0.72, p = 0.1925). Nonsignificant decreases in PS volume, days per week, nonprotein calories, and PNDI were observed.
Teduglutide discontinued
Teduglutide treatment was discontinued for 10 patients (37 %) at mean 62.59 (SD=55.55) weeks. PS volume, hours per day, PNDI, nonprotein calories, and lipid dose were significantly higher for patients who discontinued teduglutide compared to those who successfully weaned from PS. 4 patients discontinued teduglutide for reasons related to treatment (2 stomal prolapse, 1 increased ostomy output, 1 gallstones), 6 for unrelated reasons (2 unrelated infections and hospitalizations, 4 electively or due to plateaus in improvement). 5 patients (50 %) achieved a significant reduction in PS volume of ≥ 20 %. BMI did not change significantly over the course of teduglutide treatment.
Subgroup analysis by age at baseline
Subgroup analysis was performed comparing patients below and above the age of 5 at baseline. 8 patients (35 %) were under age 5 at the time of teduglutide initiation. These patients experienced a nonsignificant decrease in PS volume (p = 0.6172) whereas older patients experienced a significand decrease (p = 0.00162). Older patients also experienced significant decreases in days receiving PS, PNDI, and nonprotein calories provided by PS.
Safety
Adverse events were reviewed for 32 patients, including patients excluded from final analysis. 29 patients (90.6 %) experienced a total of 112 AEs over the course of treatment. AEs recorded for > 5 % of teduglutide-treated patients are listed in Table 4. Most frequently noted AEs include pyrexia (excluding central line infection) (50 %); central line systemic infection (47 %); abdominal pain, (19 %); vomiting (16 %), diarrhea (13 %), stomal prolapse (9 %). 94 events (85 %) were considered serious. 11 events (10 %) were related to teduglutide treatment (Table 5).
Narratives of patients discontinuing teduglutide because of an adverse event considered related to treatment
Patient 1. This was a one-year-old patient with Hirschsprung’s Disease and a jejunostomy. 20 weeks after teduglutide initiation, the patient experienced an approximately 3-inch stomal prolapse requiring repeat reduction and subsequent hospitalization for monitoring. Teduglutide was stopped due to known associations with intestinal and stomal obstructions.
Patient 2. This was a nine-year-old patient with Hirschsprung’s Disease and a jejunostomy. 19 weeks after teduglutide initiation, the patient experienced significant worsening of his stomal prolapse. Teduglutide was stopped; however, the stomal prolapse required surgical correction.
Patient 3. This was a three-year-old patient with Hirschsprung’s Disease and an ileostomy. 7 weeks after teduglutide initiation, the patient was admitted with increased ostomy output. Biopsies revealed villous blunting, crypt hyperplasia, and an increase in inflammatory cells in the lamina propria. Teduglutide was discontinued after increased ostomy output was assessed to be secretory diarrhea.
Patient 4. This was an 11-year-old patient with volvulus who received teduglutide for 72 weeks. The patient developed obstructive gallstones requiring endoscopic retrograde cholangiopancreatography. Teduglutide was discontinued as there is a reported association with gallstones.
Discussion
In this retrospective review, teduglutide was effective in reducing dependency on parenteral support. 67 % of patients achieved the primary end point defined as a reduction in PS volume of ≥ 20 % from baseline and 30 % achieved enteral autonomy. This finding is consistent with randomized controlled trials in pediatric populations. [3,5,6] Treatment outcome (reaching enteral autonomy versus discontinuing treatment) was associated with the level of dependency on PS at baseline. Patients who achieved enteral autonomy had significantly lower PS volume, hours per day, PNDI, nonprotein calories, and lipids compared to those who discontinued teduglutide. Successful PS weaning was not observed in patients with a PNDI value over 53 %, indicating that a higher PNDI may predict unsuccessful weaning. Cumulatively, these results suggest that reaching a certain degree of freedom from PS without teduglutide may serve as a predictor of complete discontinuation with teduglutide. This may be more strongly indicated by minimal caloric needs compared to fluid needs as the difference in caloric needs for those that successfully achieved enteral autonomy seemed more notable. Baseline PNDI values for the 8 patients who achieved enteral autonomy ranged from 15 % to 53 %. A control group was unable to be established due to the center’s practice of enrolling all eligible patients onto teduglutide. In this case, a control group would have consisted of patients with major complications in which teduglutide was contraindicated.
Subgroup analysis by age indicated that older patients experienced more significant decreases in PS dependency compared to patients under age 5.
Lipid dosage decreased significantly over the course of treatment. None of the patients who continued PS were able to discontinue lipids, suggesting that lipid discontinuation may indicate a patient is nearing enteral autonomy. Perhaps normal lipid metabolism to avoid biochemical essential fatty acid deficiency is a precursor to successful weaning from parenteral support that requires further investigation. Furthermore, lipids delivered through parenteral nutrition solution may contribute to liver injury, subsequently necessitating transplantation. [7] While we hypothesized that in some instances teduglutide may decrease liver damage and thus eliminate liver transplant need, there have been no such examples in clinical practice in our institution.
Patients who discontinued teduglutide treatment experienced modest decreases in PS volume, PNDI, and PS nonprotein calories over the course of treatment. 50 % of these patients achieved the primary end point, comparable to the rate observed in patients who continued to receive teduglutide treatment and PS at the most recent clinic visit. These findings suggest that teduglutide may have had some clinical value for these patients by contributing to PS weaning. One challenge in determining appropriate teduglutide use has been valuing these more modest reductions in PS against the high cost of the drug itself. While population-based models suggest that teduglutide use may not reach traditional cost-effectiveness thresholds, individual considerations focused on the value of more modest changes in parenteral support may alter those considerations, especially for children in whom a modest reduction in parenteral support may facilitate school attendance, developmentally appropriate activities, or other significant contributors to quality of life. [8-10]
Teduglutide was generally well-tolerated, with 4 patients (15 %) discontinuing treatment due to related adverse events. The most frequently recorded AEs included pyrexia and central line systemic infections, which are to be expected for this population due to the nature of SBS and the age of patients. Most events of pyrexia resulted in hospitalization due to patients’ vulnerability to life-threatening infection. These events were consequently classified as SAEs; however, none of these events were considered related to teduglutide treatment. Pyrexia, central line infections, and abdominal pain occurred at similar rates in previously published studies in pediatric populations. [11] Vomiting was observed less frequently in this report than in many publications. This could be due to the retrospective nature of this report and limited frequency of clinic visits in some cases. The two cases of stomal prolapse, including one where surgical correction was required, do lead to some pause in our consideration for teduglutide use in children with severe type 1 anatomy with limited likelihood of achieving meaningful parenteral support reduction. Additionally, 3 patients with Hirschsprung’s disease were included in the study but all discontinued teduglutide use at mean 15.9 weeks. This was likely due to the presence of a small bowel stoma in two of these patients and subsequent stomal prolapse.
While limitations of this case series include its retrospective nature at a single center, the relatively large sample size adds to the growing body of evidence supporting GLP-2 analogues. In particular, we propose two potential indicators of successful teduglutide therapy when attempting to predict enteral autonomy achievement: baseline PNDI and lipid discontinuation while receiving teduglutide. Future prospective work may utilize these along with other suggested indicators in the literature, such as baseline oral intake, to develop more realistic decision support for children considering teduglutide therapy. [12]
Conclusion
In conclusion, this real-world assessment of pediatric patients with SBS treated with teduglutide demonstrated significant reductions in PS dependency over mean 120.8 weeks, with 30 % achieving enteral autonomy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Duggan CP, Jaksic T. Pediatric intestinal failure. N Engl J Med 2017;377(7):666–75. 10.1056/nejmra 1602650.28813225 · doi ↗ · pubmed ↗
- 2Drucker DJ. Glucagon-like peptide 2. J Clin Endocrinol Metab 2001;86(4):1759–64. 10.1210/JCEM.86.4.7386.11297614 · doi ↗ · pubmed ↗
- 3Wales PW, Hill S, Robinson I, Long-term teduglutide associated with improved response in pediatric short bowel syndrome-associated intestinal failure. J Pedia Gastroenterol Nutr 2024;79(2):290–300. 10.1002/jpn 3.12276. · doi ↗
- 4Norsa L, Goulet O, Alberti D, Nutrition and intestinal rehabilitation of children with short bowel syndrome: a position paper of the ESPGHAN committee on nutrition. Part 2: Long-Term Follow-Up on home parenteral nutrition. J Pedia Gastroenterol Nutr 2023;77(2):298–314. 10.1097/MPG.0000000000003850. · doi ↗
- 5Kocoshis SA, Merritt RJ, Hill S, Safety and efficacy of teduglutide in pediatric patients with intestinal failure due to short bowel syndrome: a 24-Week, phase III study. J Parenter Enter Nutr 2020;44(4):621–31. 10.1002/jpen.1690. · doi ↗
- 6Chiba M, Masumoto K, Kaji T, Efficacy and safety of teduglutide in infants and children with short bowel syndrome dependent on parenteral support. J Pedia Gastroenterol Nutr 2023;77(3):339–46. 10.1097/MPG.0000000000003867. · doi ↗
- 7Żalikowska-Gardocka M, Przybyłkowski A. Review of parenteral nutrition-associated liver disease. Clin Exp Hepatol 2020;6(2). 10.5114/ceh.2019.95528. · doi ↗
- 8Raghu VK, Binion DG, Smith KJ. Cost-effectiveness of teduglutide in adult patients with short bowel syndrome: Markov modeling using traditional cost-effectiveness criteria. Am J Clin Nutr 2019;111(1):141. 10.1093/AJCN/NQZ 269. · doi ↗