Temporal Relationship Between Seasonal Burn Incidence and Clinical Severity in a Long-Term Regional Cohort
Saleh Alhotan, Abdulaziz Aljasser, Shoug Alaodah, Mona Almansour, Renad Alrish, Rawan Alkhalaf, Mansour Alharbi, Abdullah Alzain, Bassem Alomari

TL;DR
This study finds that in the Qassim region, burn severity in adults increases in winter, while overall burn rates remain stable year-round, especially due to pediatric injuries.
Contribution
The study reveals a dissociation between seasonal burn admission volume and injury severity in an arid region, emphasizing adult severity in winter.
Findings
Winter admissions had higher median TBSA compared to summer admissions.
Scald injuries were the most common across all seasons, with no significant severity difference in winter.
Cultural periods showed predictable injury clustering but no significant increase in admission volume.
Abstract
Background: Seasonal changes have a measurable impact on burn frequency and clinical implications, yet the relationship with injury severity remains understudied in arid regions. This study evaluated the association between seasonal and cultural burn trends in the Qassim region, focusing on the dissociation between admission volume and injury severity. Methods: A retrospective registry analysis was conducted for all acute burn admissions to the regional referral center from November 2018 to November 2025 (n=816). Monthly admission volume was examined using negative binomial regression, and injury severity, measured as percent total body surface area burned (%TBSA), was analyzed using RStudio (Posit, Boston, MA). A two-sided p-value < 0.05 was deemed statistically significant. Data were categorized by age, season, and cultural time (Ramadan/Eid). Results: Injury severity varied…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
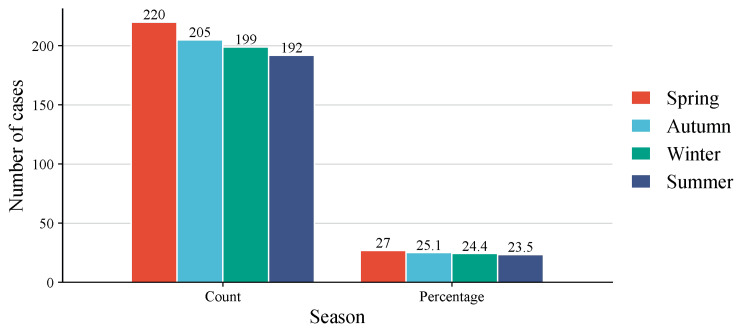 Figure 1
Figure 1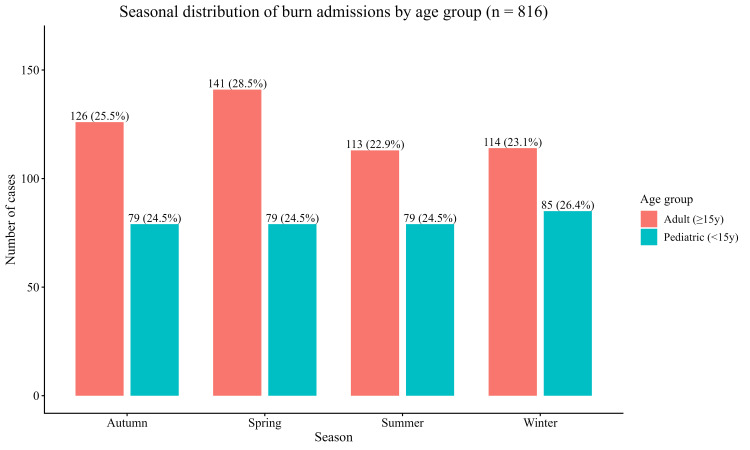 Figure 2
Figure 2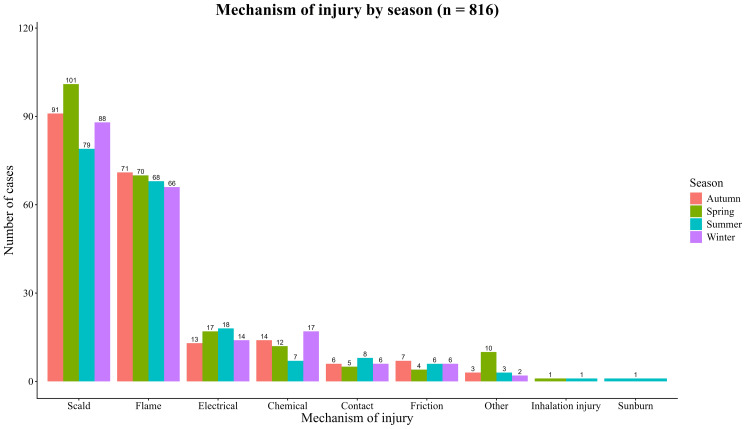 Figure 3
Figure 3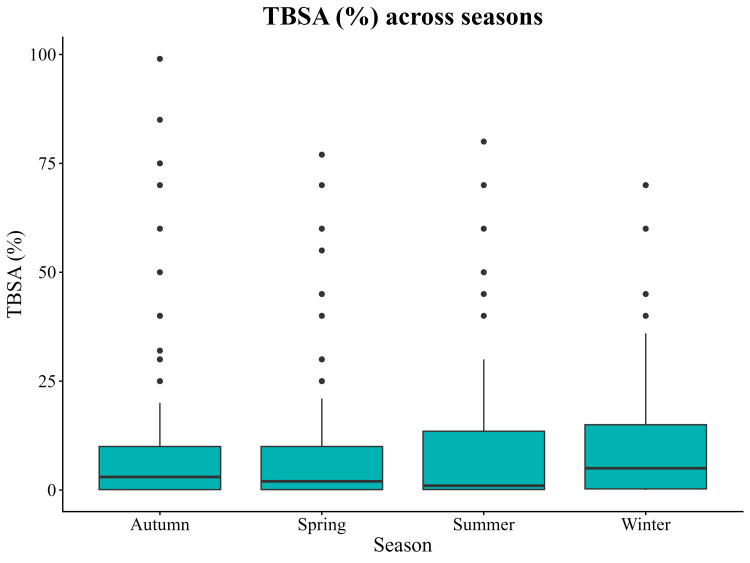 Figure 4
Figure 4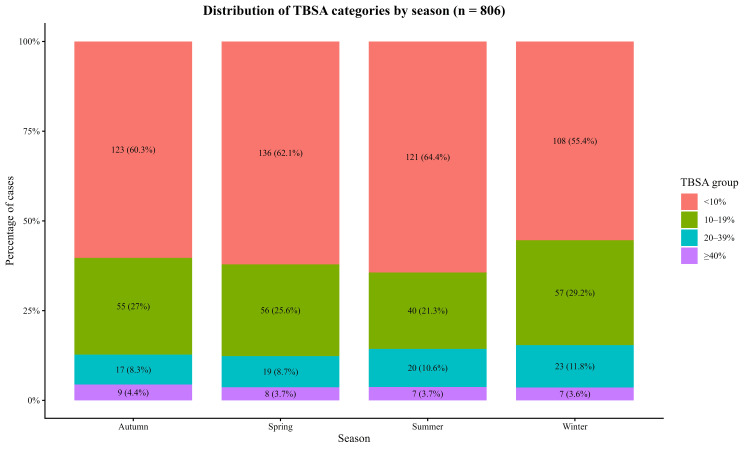 Figure 5
Figure 5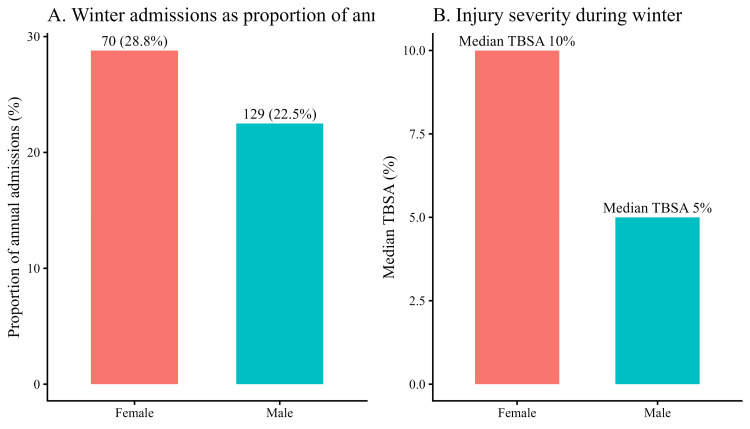 Figure 6
Figure 6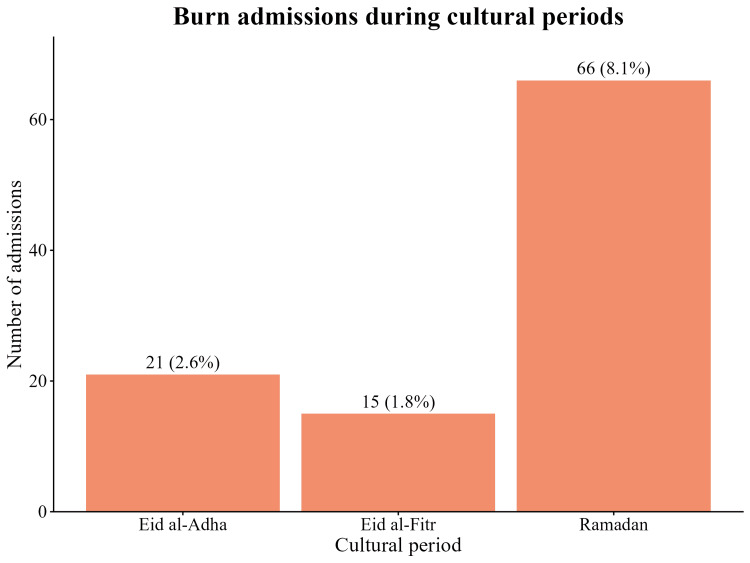 Figure 7
Figure 7| Variables | Values |
| Total patients | 816 |
| Age (n=816): | |
| Mean age | 24.1 years (SD 20.5) |
| Median age | 24 years (IQR 3-37) |
| Range | 1 day - 94 years |
| Sex: | |
| Male | 573 (70.2%) |
| Female | 243 (29.8%) |
| Mechanism of injury (n=816) | |
| Scald | 359 (44.0%) |
| Flame | 275 (33.7%) |
| Electrical | 62 (7.6%) |
| Chemical | 50 (6.1%) |
| Contact | 25 (3.1%) |
| Friction | 23 (2.8%) |
| Inhalation injury | 2 (0.2%) |
| Sunburn | 1 (0.1%) |
| Other | 18 (2.2%) |
| Missing | 1 (0.1%) |
| TBSA (n=806) | |
| Median | 5% (IQR 0.14-11%) |
| Mean | 8.7% (SD 13.1%) |
| Range | 0-99% |
| Season | Number of cases |
| Spring | 220 (27.0%) |
| Autumn | 205 (25.1%) |
| Winter | 199 (24.4%) |
| Summer | 192 (23.5%) |
| Number of cases per Season in percent | ||||
| Causes | Autumn | Spring | Summer | Winter |
| Scald | 44.4% | 45.9% | 41.0% | 44.2% |
| Flame | 34.6% | 31.8% | 35.6% | 33.2% |
| Electrical | 6.3% | 7.7% | 9.4% | 7.0% |
| Chemical | 6.8% | 5.5% | 3.7% | 8.5% |
| Contact | 2.9% | 2.3% | 4.2% | 3.0% |
| Friction | 3.4% | 1.8% | 3.1% | 3.0% |
| Inhalation injury | 0.0% | 0.5% | 0.5% | 0.0% |
| Other | 1.5% | 4.5% | 1.6% | 1.0% |
| sunburn | 0.0% | 0.0% | 0.5% | 0.0% |
| Season | No. of cases | Median | IQR | Mean | SD |
| Autumn | 204 | 3% | 0.1-10% | 8.65% | 14.40% |
| Spring | 219 | 2% | 0.1-10% | 8.01% | 12.40% |
| Summer | 188 | 1% | 0.1-13.5% | 8.14% | 12.80% |
| Winter | 195 | 5% | 0.3-15% | 9.91% | 12.90% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBurn Injury Management and Outcomes · Injury Epidemiology and Prevention · Thermal Regulation in Medicine
Introduction
Burn injuries are a well-established global public health concern, ranking among the main causes of trauma-related morbidity and mortality worldwide [1,2]. According to the Global Burden of Diseases, approximately nine million new burn injuries required medical attention in 2019 and resulted in over 120,000 fatalities, the majority of which occurred in low- and middle-income countries (LMICs) with limited acute care capacity [1,2]. Over 90% of fatal fire‑related burns occur in LMICs, and South‑East Asia alone accounts for more than half of these deaths [2].
Seasonal changes are a major modulator of burn epidemiology. Hence, retrospective analyses from Portugal, Turkey, North Carolina, and Switzerland demonstrate that burn admissions tend to cluster in the winter months, when indoor heating, open flame devices, and combustible fuels increase the risk of fire-related injuries [3-6]. In contrast, spring and summer peaks have been reported in Bangladesh, India, and Sub‑Saharan Africa, where outdoor cooking, agricultural work, and the preparation of traditional foods increase exposure to hot liquids and flames [2]. Notably, seasonality may alter both the frequency and severity of burns. A recent study from Turkey found that the number of people admitted to the hospital was varied across seasons and the severity of their injuries, assessed by TBSA (%), was different. There were different patterns in the summer and winter months [4].
Cultural periods significantly influence burn risk, particularly in the Middle East [7]. In Muslim regions, Ramadan is associated with altered cooking patterns, increased nighttime meal preparation, and fatigue-related lapses in supervision [2]. These behavioral shifts, especially among women responsible for domestic activities, have been linked to a rise in scald and flame injuries [8-10]. Similarly, the Eid al-Fitr and Eid al-Adha festivals contribute to short-term increases in thermal injury risk through large-scale festive cooking, outdoor grilling, and the use of fireworks [3,11].
More importantly, Children bear a disproportionate share of this burden; burns are the sixth most common cause of death among 5- to 14‑year‑old children and the fourth-ranked injury globally that requires medical attention [12-15]. Among pediatric populations, burn incidence peaks in children under five years of age, a group that depends entirely on caregivers and lacks self‑protection abilities [2,12]. According to studies from Ghana, Iran, the United Arab Emirates (UAE), and India, infants and toddlers (0-4 years) account for up to 50% of all pediatric burn hospitalizations, with scald injuries being the most common [2,16,17]. In Saudi Arabia, a systematic review conducted on 3,308 patients found that 52% of burn incidences occurred in children under the age of 10 years, and scalding accounted for 62% of injuries [18]. These patterns highlight the urgent need for age‑targeted prevention strategies.
Despite Saudi Arabia's tremendous socioeconomic progress, burn-related morbidity remains a significant concern. Local hospital-based studies from Riyadh, Jeddah, and Dammam show that 83% of burns occur at home, with males outnumbering females substantially [18,19]. However, most published papers are single-site, cross-sectional, or have short observation periods, making it impossible to conduct a thorough examination of temporal trends [18]. The Qassim region, characterized by a desert climate with extreme summer heat and cold winters, lacks longitudinal data on seasonal and cultural injury clustering. This study aims to evaluate a seven-year dataset from the region's central referral center. To decipher if burn admission volume and injury severity in Qassim have a seasonal pattern, as well as how cultural periods (Ramadan and Eid) and patient age affect these trends.
Materials and methods
Study design and setting
This study was a retrospective observational analysis conducted at King Fahad Specialist Hospital (KFSH) in Buraidah. KFSH is the principal burn referral facility for the Qassim Health Cluster, receiving patients from across the region. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [20] (see supplementary 1 in Appendices). The study utilized a seven-year dataset covering all acute burn presentations from November 1, 2018, to November 30, 2025. All patients admitted with acute thermal, chemical, or electrical burn injuries were eligible for inclusion. Exclusion criteria included friction injuries without tissue loss, chronic non-burn wounds, and readmissions for the same injury episode.
Variables and definitions
Temporal Variables
Seasonality was defined meteorologically: Winter (December-February), Spring (March-May), Summer (June-August), and Autumn (September-November). Cultural periods included Ramadan, which was coded using the full lunar-month date range for each Gregorian year and the Eid holidays (Eid al-Fitr and Eid al-Adha), which were captured using a three- to four-day window surrounding the holiday dates to account for pre-celebration preparations and festivities (see supplementary 2, 3, and 4 in Appendices).
Clinical Variables
Data points included age, sex, mechanism of injury, and Total Body Surface Area (TBSA). To identify age-related risk factors, the population was divided into pediatric (<15 years) and adult (≥15 years) subgroups.
Outcomes
The primary outcomes were monthly admission volume and injury severity. Injury severity was assessed using burn size, measured as the percentage of total body surface area burned (TBSA, %). This seasonal analysis did not focus on mortality and length of stay, which were recorded in the registry.
Data handling
Baseline demographic and clinical data were extracted for the full cohort of 816 patients. Admission dates were complete for all cases. TBSA data was available for 806 patients (98.8%), and age was available for all 816 patients (100%). Missing data for other variables was negligible (<1%) and handled through complete-case analysis.
Statistical analysis
Categorical variables were summarized as counts and percentages, while continuous variables (TBSA, age) were reported as medians with interquartile ranges (IQR) due to non-normal distribution. (a) Group comparisons: burn mechanism distributions were compared across seasons using the chi-square test. Seasonal differences in injury severity, assessed by TBSA (%), were evaluated using the Kruskal-Wallis rank-sum test. Sex-based differences in TBSA during the winter season were evaluated using the Wilcoxon rank-sum test. Fisher’s exact test was applied to evaluate the association between the mechanism of injury and the defined cultural periods. (b) Time-series analysis: monthly case counts were analyzed using negative binomial regression adjusted for a calendar year to control for long-term population trends. Incidence rate ratios (IRRs) with 95% confidence intervals (CIs) were calculated. (c) Model selection: a Poisson regression model was initially used. Tests for overdispersion revealed a dispersion ratio of 1.14, indicating an acceptable match. However, a negative binomial model was used to ensure resilience against modest deviations from Poisson assumptions as well as conformity with normal burn epidemiology methodologies. All analyses were performed using RStudio (Posit, Boston, MA). A two-sided p-value < 0.05 was considered statistically significant.
Ethical approval
The study received formal approval from the Qassim Regional Research Ethics Committee (Registration No. 607-47-5877). Approval was granted under the expedited review category for implementation. The committee waived the requirement for informed consent because the study used retrospective, fully anonymized data with no direct patient contact.
Results
Baseline characteristics
A total of 816 patients were admitted during the seven-year study period (November 2018 to November 2025). The cohort was predominantly male (n = 573; 70.2%), with a male-to-female ratio of 2.4:1. The mean age was 24.1 years (SD 20.5), and the median age was 24 years (IQR 3-37), with a range from neonates (one day) to 94 years (Table 1).
Seasonal distribution and regression analysis
Descriptive analysis showed that Spring accounted for the highest proportion of admissions, followed by Autumn. However, a negative binomial regression, adjusted for calendar year, showed that these differences were not statistically significant. Summer (IRR 0.86, p = 0.10), Autumn (IRR 0.92, p = 0.35), and Winter (IRR 0.91, p = 0.28) did not indicate a significant difference in monthly case volume from Spring (reference). The regression for the calendar year was also non-significant (p = 0.97), indicating that admission volume remained stable during a seven-year period (Table 2 and Figure 1).
Seasonal distribution of acute burn admissions (n = 816)The bar chart illustrates total admission counts across the four meteorological seasons from November 2018 to November 2025. Percentages above the bars represent the proportion of total annual admissions. Negative binomial regression revealed no statistically significant seasonal variation in aggregate admission volume (p = 0.55), highlighting a stable year-round frequency of burn injuries in the Qassim region.
Age-specific seasonal patterns
Stratification by age group revealed that seasonal variance was mostly driven by adults. Pediatric admissions (<15 years, n = 322; 39.5%) were nearly similarly distributed over the year, where adult admissions (≥15 years, n = 494; 60.5%) showed evident seasonal variability, with a peak in Spring (n=141; 28.5%) and a relative nadir in Summer (n=113; 22.9%) (Figure 2).
Seasonal distribution of burn admissions stratified by age groupBars show the number of pediatric (<15 years) and adult (≥15 years) admissions across the four seasons (n = 816). Pediatric admissions are relatively evenly distributed, whereas adult cases show a peak in Spring.
Mechanism and TBSA%
Scald injuries were the most common mechanism in all seasons, followed by flame burns. Electrical, chemical, contact, and friction injuries were consistently less common, whereas inhalation injuries and sunburn were infrequent. The overall distribution of burn mechanisms did not change considerably over seasons (Table 3 and Figure 3).
Mechanism of injury by season (n = 816)Stacked bar chart showing the distribution of burn mechanisms (scald, flame, electrical, chemical, contact, friction, etc.) within each of the four seasons.
Injury severity, measured by TBSA %, demonstrated statistically significant seasonal variation (Kruskal-Wallis χ² = 10.88, df = 3, p = 0.012). Complete TBSA data were available for 806 cases. Winter admissions showed the highest burn severity. In contrast, summer admissions had the lowest severity. Spring and Autumn presented intermediate patterns. (Table 4 and Figures 4, 5).
Distribution of burn Total Body Surface Area (TBSA) across seasons (n = 806).Boxplots show the median, interquartile range, and whiskers representing 1.5×IQR. Winter admissions demonstrated the highest injury severity (median TBSA 5%, IQR 0.3-15%), while Summer showed the lowest (median TBSA 1%, IQR 0.1-13.5%). A Kruskal–Wallis test identified a statistically significant difference in TBSA across seasons (χ² = 10.88, df = 3, p = 0.012).
Distribution of burn extent categories (TBSA%) across seasons (n = 806)Stacked bar charts display the proportion and absolute number of cases within TBSA groups (<10%, 10-19%, 20-39%, ≥40%) for each season. Values are shown as n (%) within season. Mild burns (<10% TBSA) predominated across all seasons, while winter demonstrated a higher relative proportion of burns involving ≥10% TBSA, particularly within the 10–19% and 20–39% categories.
Sex-stratified winter analysis
During winter, males accounted for a higher absolute number of admissions (129) than females (70). However, when adjusted for annual admission volume, winter admissions accounted for a greater proportion of total cases among females (70, 28.8%) than males (129, 22.5%). Among patients with available TBSA data, the median burn size in winter was higher in females (10%) than in males (5%), although this difference did not reach statistical significance (Wilcoxon rank-sum test, p = 0.17) (Figure 6).
Sex-stratified analysis of winter burn admissionsPanel A shows winter admissions expressed as a proportion of each sex’s total annual admissions, with females accounting for 70 (28.8%) cases and males for 129 (22.5%). Panel B illustrates median injury severity during winter, measured by total body surface area (TBSA), which was higher among females (median 10%) than males (median 5%), although this difference did not reach statistical significance (Wilcoxon rank-sum test, p = 0.17).
Cultural periods
A total of 66 admissions occurred during Ramadan, accounting for 8.1% of all cases. This period showed an injury pattern aligned with household and domestic activity. Additional clusters were observed during the Eid holidays: 15 admissions (1.8%) occurred during the Eid al-Fitr window, and 21 admissions (2.6%) occurred during the Eid al-Adha window. The distribution of burn mechanisms during Ramadan did not differ significantly from non-Ramadan periods (Fisher’s exact test, p = 0.27). Scald and flame injuries accounted for the majority of cases during both Ramadan and non-Ramadan periods (Figure 7).
Burn admissions during cultural periodsNumber and percentage of admissions occurring during Ramadan (66 cases; 8.1%), Eid al-Fitr (15 cases; 1.8%), and Eid al-Adha (21 cases; 2.6%) across the seven-year study period (n = 816). These cultural clusters constitute a small proportion of total admissions but reflect identifiable temporal patterns aligned with domestic and holiday activities.
Discussion
Although seasonal burn patterns are widely recognized, the distinction between seasonal frequency and injury severity is often overlooked, particularly in arid regions. Elucidating whether seasonal risks drive exposure volume or injury intensity is vital for refining public health interventions and understanding the specific epidemiological nuances of the Qassim region. This seven-year retrospective analysis is the most thorough assessment of temporal burn patterns in the Qassim region to date, providing a detailed understanding of how injury epidemiology interacts with season and culture. By separating admission frequency from injury severity, this study reveals a key epidemiologic feature that aligns with findings from other studies in high-income and low-and middle-income settings. While burn admissions remain statistically consistent throughout the year, injury severity changes dramatically by season. Specifically, despite stable admission counts, burn severity measured by total body surface area (TBSA) increased during the winter months, revealing a clear dissociation between frequency and severity that mirrors winter's severity peaks, which was reported in other studies from Portugal, Turkey, and Switzerland, where colder months are associated with greater TBSA and deeper injuries [3-5]. Our finding underscores that seasonality can manifest as either frequency-driven or severity-driven, depending on local exposure contexts.
The stability of overall admission rates is a novel observation for this region and is explained by the consistent pediatric baseline: pediatric admissions (<15 years) were evenly distributed across seasons and showed no seasonal influence on regression analysis, reflecting a continuous domestic risk that persists regardless of environmental conditions [21]. This pediatric “steady state” has been documented in the WHO Global Burn Registry, where children aged 1-5 years constitute 62% of pediatric entries and exhibit scald predominance year-round [21]. Adult admissions, in contrast, displayed predictable seasonal fluctuations, with a clear peak in spring and a nadir in summertime, which is a pattern reminiscent of the spring peak observed in German and Dutch burn unit data, where longer daylight hours and increased outdoor work correlate with higher flame burn incidence [4]. However, these adult‑specific differences did not achieve statistical significance after adjustment for exposure time and were insufficient to alter aggregate admission patterns because the stabilizing effect of pediatric cases buffered overall volume. This explains why the visually apparent adult seasonality did not persist in the final regression models and highlights how pediatric epidemiology can mask adult temporal trends when analyzed in aggregate.
The most clinically significant finding of the study is the increase in burn intensity during the winter. The median TBSA in winter was five times higher than in summer (p = 0.012), indicating a significant seasonal increase in injury severity despite a steady admission volume, which is in alignment with Turkish and Iranian studies reporting similar TBSA outcomes across seasons [4,16]. Similarly, the probability of severe burns (≥20% TBSA) was numerically higher in winter, but not statistically significant. Taken together, these patterns suggest a seasonal shift in exposure rather than a change in burn mechanisms. In practical terms, winter creates several risk conditions at home, including extended contact with hot water, higher tap-water temperatures from heating systems, and increased use of heaters, all of which can exacerbate scald severity while remaining coded under the same mechanism. Furthermore, cultural habits in the region, particularly the preparation and consumption of hot tea and Arabic coffee around open fires during winter gatherings, increase the risk of accidental spills and contact injuries. As a group, these factors offer a more plausible explanation for the rise in burn intensity during winter than mechanism distribution alone.
Sex-stratified analysis provides further context for the observed winter increase in burn severity. Although winter admissions represented a higher proportion of annual cases among females than males, injury severity did not differ significantly between genders. This pattern contrasts with reports from the UAE and Southwestern Saudi Arabia, where male predominance in burn admissions has been linked to workplace-related exposures [17,19]. In our cohort, the absence of a sex-based difference in TBSA suggests that occupational exposure is unlikely to be the primary driver of winter-associated burn severity. Instead, the findings point toward shared household risk factors affecting both sexes. Winter-related domestic exposures, including elevated hot-water temperatures from household heating systems, prolonged bathing during colder months, and contact with heating-related devices, including hot-water bags or warming pads, may increase burn extent while remaining classified under broad mechanism categories such as scalds. This interpretation is consistent with evidence from an East Mediterranean systematic review, which identified the home as the injury location in 72-94% of burn cases and highlighted indoor heating practices as major contributors to winter burns [7].
Cultural periods revealed distinct but circumscribed temporal clustering. Ramadan accounted for 8.1% of admissions, a proportion consistent with its duration in the lunar calendar, suggesting no aggregate surge in burn volume. Although the distribution of burn mechanisms during Ramadan did not differ significantly from that in non-Ramadan periods, the observed predominance of scald and flame injuries suggests a predictable risk window associated with intensified evening meal preparation, echoing trends across the Middle East where holiday-related cooking spikes correlate with pediatric injuries [2,7]. Similarly, while Eid al-Fitr and Eid al-Adha were associated with identifiable admission clusters, these did not constitute statistically significant elevations in daily rates. Rather, their temporal concentration reflects predictable exposure patterns linked to holiday-specific activities. Consequently, these findings advocate for targeted, event-specific prevention messaging over broad seasonal interventions, supporting the established efficacy of culturally tailored education [19].
This study has limitations due to its retrospective, single-center methodology. Although King Fahad Specialist Hospital serves as the regional referral center, small burns treated in primary care or private clinics may be underrepresented, thereby biasing the cohort towards more serious injuries. Burn mechanisms were defined using broad clinical categories, which may have obscured contextual distinctions within mechanisms, particularly for scald injuries. Detailed information on water temperature, duration of exposure, heating device type, and prehospital delay was unavailable, making it impossible to draw definitive causal conclusions about winter harshness. Furthermore, socioeconomic indicators were not collected, limiting the estimation of household vulnerability. Future prospective or mixed-methods investigations should incorporate these characteristics.
Conclusions
This seven-year regional analysis elucidates a distinct dissociation between seasonal burn frequency and burn extent (TBSA %) in the Qassim region. While admission volume remained statistically stable year-round, underpinned by a persistent and consistent pediatric baseline, TBSA % increased significantly during the winter months. This seasonal escalation in TBSA % was independent of shifts in mechanism distribution, flame-specific severity, or sex, highlighting the decisive impact of winter-associated domestic exposures. These data support a bifurcated prevention strategy: pediatric burn prevention must remain a continuous, year-round domestic priority, while population-level interventions should be intensified during winter to mitigate injury severity through targeted education on domestic hot-water safety and heating device regulation. Ultimately, incorporating a focus on severity mitigation alongside traditional frequency-reduction efforts allows for a more precise public health response, optimizing the allocation of specialized burn resources and enhancing overall patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The epidemiological characteristic and trends of burns globally BMC Public Health Yakupu A Zhang J Dong W Song F Dong J Lu S 15962220223599611610.1186/s 12889-022-13887-2PMC 9396832 · doi ↗ · pubmed ↗
- 2Burns in low- and middle-income countries: a review of available literature on descriptive epidemiology, risk factors, treatment, and prevention Burns Forjuoh SN 5295373220061677734010.1016/j.burns.2006.04.002 · doi ↗ · pubmed ↗
- 3Seasonal impact in burn profiles in a dedicated burn unit Burns Mata Ribeiro L Vieira LG Sousa JM Guerra AS 118911984520193094827910.1016/j.burns.2019.03.008 · doi ↗ · pubmed ↗
- 4Seasonal effects on the mechanisms of burn injuries Turk J Surg ÇomçalıB Ceylan C Altun Özdemir B OcaklıS Pehlevan Özel H Çınar YastıA 5103820223587374010.47717/turkjsurg.2022.5377 PMC 9278355 · doi ↗ · pubmed ↗
- 5To everything there is a season: impact of seasonal change on admissions, acuity of injury, length of stay, throughput, and charges at an accredited, regional burn center Ann Plast Surg Hultman CS Tong WT Surrusco M Roden KS Kiser M Cairns BA 30346920122262749610.1097/SAP.0b 013e 31823 f 3df 0 · doi ↗ · pubmed ↗
- 6Trauma mechanisms and injury patterns in pediatric burn patients Burns Moehrlen T Szucs T Landolt MA Meuli M Schiestl C Moehrlen U 3263344420182885506010.1016/j.burns.2017.07.012 · doi ↗ · pubmed ↗
- 7Epidemiology of burn injuries in the East Mediterranean Region: a systematic review BMC Public Health Othman N Kendrick D 831020102017052710.1186/1471-2458-10-83PMC 2841676 · doi ↗ · pubmed ↗
- 8Epidemiology and outcomes of cooking- and cookstove-related burn injuries: a World Health Organization Global burn registry report J Burn Care Res Mehta K Thrikutam N Hoyte-Williams PE Falk H Nakarmi K Stewart B 5085164420233485002110.1093/jbcr/irab 166PMC 10413420 · doi ↗ · pubmed ↗